










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.108 no.5 Madrid may. 2016
PICTURES IN DIGESTIVE PATHOLOGY
Endoscopic diagnosis of asymptomatic perforation of colonic diverticulum
Diagnóstico endoscópico de perforación asintomática de divertículo de colon
Luis María Merino Peñacoba1, María Lourdes Ruiz-Rebollo2, Íñigo López-de-Cenarruzabeitia1, Elvira González-Obeso3 and Juan Beltrán-de-Heredia-y-Rentería1
1 Departmet of General Surgery and Digestive Diseases.2 Department of Digestive Diseases.
3 Department of Pathology. Hospital Clínico Universitario de Valladolid. Valladolid, Spain
Background
Colonic perforation as complication of acute diverticulitis is a relatively frequent pathology and generally very symptomatic. Nevertheless, when it occurs in the mesenteric border, the course can be indolent.
Case Report
An 82-year-old woman with a history of acute diverticulitis without any clinic or radiologic complications was treated medically with a satisfactory evolution. She remained asymptomatic 7 weeks after the acute process until control colonoscopy was performed.
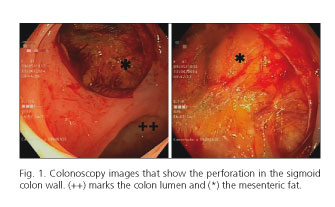
Twenty-two centimetres from the anal margin, multiple colonic diverticula were found and one covered a perforation (Fig. 1). The test was cancelled and a CT was performed, showing an important retroneumoperitoneum secondary to a diverticular perforation (Fig. 2).

The patient underwent emergency surgery, during which a sigmoid colon perforation was found in the mesenteric border. A Hartmann type intervention was performed and postoperative period was uneventful.
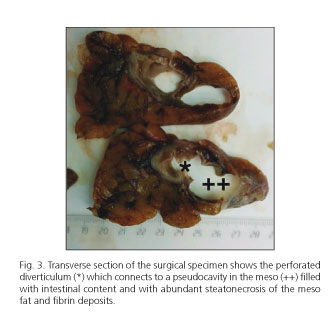
The anatomopathological report confirmed the existence of a plastron secondary to a perforated diverticulum that opened to a cavity in the mesentery that contained fecaloid matter and focus of steatonecrosis fibrin deposits (Fig. 3), which confirmed the existence of a perforation prior to colonoscopy.
Discussion
Colonoscopy is indicated 4-6 weeks after an episode of acute diverticulitis, in order to confirm the diagnosis and rule out malignant processes and other inflammatory diseases. Iatrogenic perforations have been described; however, we have not found any report that supports this case.
Fortunately for this patient, the perforation occurred in the mesenteric border and was covered by the mesosigma. This avoided peritonitis keeping the patient asymptomatic for weeks.
References
1. Choi YH, Koh SJ, Kim JW, et al. Do we need colonoscopy following acute diverticulitis detected on computed tomography to exclude colorectal malignancy? Dig Dis Sci 2014;59:2236-42. DOI: 10.1007/s10620-014-3151-1. [ Links ]
2. Wilkins T, Embry K, George R. Diagnosis and management of acute diverticulitis. Am Fam Physician 2013;87:612-20. [ Links ]
3. Polter DE. Risk of colon perforation during colonoscopy at Baylor University Medical Center. Proc (Bayl Univ Med Cent) 2015;28:3-6. [ Links ]
4. García Martínez MT, Ruano Poblador A, Galán Raposo L, et al. Perforación tras colonoscopia: experiencia en 16 años. Rev Esp Enferm Dig 2007;99:588-92. DOI obtained: 10.4321/S1130-01082007001000005. [ Links ]
