










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.10 Madrid oct. 2017
https://dx.doi.org/10.17235/reed.2017.4645/2016
ORIGINAL PAPERS
Is it possible to predict the presence of colorectal cancer in a blood test? A probabilistic approach method
¿Es posible predecir la presencia de cáncer colorrectal en el análisis sanguíneo? Método de aproximación probabilística
José Manuel Navarro-Rodríguez1, Javier Gallego-Plazas2, Fernando Borrás-Rocher3, Rafael Calpena-Rico4, José Antonio Ruiz-Macia5 and Miguel Ángel Morcillo-Ródenas6
Services of 1General and Digestive Surgery, and 5Pathology. Hospital Vega Baja-Orihuela. Orihuela, Alicante. Spain.
Services of 2Medical Oncology, and 4General and Digestive Surgery. Hospital General Universitario de Elche. Elche, Alicante. Spain.
3Department of Statistics and Operative Research. Universidad Miguel Hernández. Elche, Alicante. Spain
ABSTRACT
Introduction: The assessment of the state of immunosurveillance (the ability of the organism to prevent the development of neoplasias) in the blood has prognostic implications of interest in colorectal cancer. We evaluated and quantified a possible predictive character of the disease in a blood test using a mathematical interaction index of several blood parameters. The predictive capacity of the index to detect colorectal cancer was also assessed.
Methods: We performed a retrospective case-control study of a comparative analysis of the distribution of blood parameters in 266 patients with colorectal cancer and 266 healthy patients during the period from 2009 to 2013.
Results: Statistically significant differences (p < 0.05) were observed between patients with colorectal cancer and the control group in terms of platelet counts, fibrinogen, total leukocytes, neutrophils, systemic immunovigilance indexes (neutrophil to lymphocyte ratio and platelet to lymphocyte ratio), hemoglobin, hematocrit and eosinophil levels. These differences allowed the design of a blood analytical profile that calculates the risk of colorectal cancer. This risk profile can be quantified via a mathematical formula with a probabilistic capacity to identify patients with the highest risk of the presence of colorectal cancer (area under the ROC curve = 0.85).
Conclusions: We showed that a colorectal cancer predictive character exists in blood which can be quantified by an interaction index of several blood parameters. The design and development of interaction indexes of blood parameters constitutes an interesting research line for the development and improvement of programs for the screening of colorectal cancer.
Key words: Colorectal cancer. Early detection. Screening. Blood test. Immunosurveillance.
RESUMEN
Introducción: la valoración del estado de inmunovigilancia (capacidad del organismo para evitar el desarrollo de neoplasias) en el análisis sanguíneo presenta connotaciones pronósticas de interés en el cáncer colorrectal. Evaluamos un posible carácter predictivo de la enfermedad en el análisis sanguíneo y su cuantificación mediante el diseño de un índice de interacción matemático entre varios parámetros sanguíneos, con capacidad predictiva probabilística de presencia de la enfermedad.
Método: estudio casos y controles de análisis comparativo de la distribución de parámetros sanguíneos, sobre 266 pacientes con cáncer colorrectal y 266 pacientes sanos, durante el periodo comprendido entre 2009-2013.
Resultados: los sujetos con cáncer colorrectal presentaron, con respecto a los controles, diferencias estadísticamente significativas (p < 0,05) en los niveles de plaquetas, fibrinógeno, leucocitos totales, neutrófilos, índices de inmunovigilancia sistémica (ratio neutrófilo/linfocito y ratio plaqueta/linfocito), hemoglobina, hematocrito y eosinófilos. Estas diferencias permitieron el diseño de un perfil analítico sanguíneo de riesgo de enfermedad, cuantificable mediante la aplicación de una fórmula matemática con capacidad de identificación probabilística de los sujetos con mayor riesgo de presencia de enfermedad (área bajo la curva del espacio ROC = 0,85).
Conclusiones: Ante la posible existencia de un carácter predictivo de presencia de cáncer colorrectal en el análisis sanguíneo, mostramos que es posible su cuantificación mediante el diseño de un índice de interacción entre varios parámetros sanguíneos. El diseño y desarrollo de índices de interacción entre parámetros sanguíneos constituye una línea de investigación de interés para el desarrollo y mejora de programas de cribado de la enfermedad.
Palabras clave: Cáncer colorrectal. Detección precoz. Cribado. Análisis sanguíneo. Inmunovigilancia.
Introduction
Colorectal cancer (CRC) has an important socio-sanitary impact in Western countries, and it is the most frequent digestive neoplasia and the third leading cause of cancer death (1,2). The understanding of its development from an adenomatous polyp to a malignant lesion (3) has allowed the establishment of programs for early detection coordinated by international organizations (4-6). These are based on the occult blood detection tests in feces with endoscopic and radiological techniques for the evaluation of the colorectal lumen. However, the gold standard method for CRC diagnosis is still colonoscopy (7).
The establishment of CRC early detection programs in Spain has required an additional effort from health services. The implementation of a screening program in our hospital resulted in an increased mean waiting time for a colonoscopy. This was caused by the need to optimize resources to ensure that a colonoscopy was performed in patients referred from the screening program as quickly as possible, without negatively affecting the care of patients on the colonoscopy waiting list referred for reasons other than the screening program (8,9). The temporary saturation of the logistic resources in the Digestive Medicine and Pathological Anatomy departments was resolved via an increase and optimization of the resources in these services. In addition, this situation was the motivation for the development of a method to optimize the prioritization criteria, with the purpose of ordering the colonoscopy waiting list including patients that are not part of the screening program.
We designed this study to evaluate the state of immunosurveillance for CRC as a possible method for the prioritization of colonoscopies in patients that are not part of a screening program. This study was based on recent lines of research that report on the evaluation of immunosurveillance (the body's ability to prevent the development of neoplasia) and its relation to the development of neoplasia such as CRC (10).
The evaluation of the immunosurveillance status and its clinical applicability in CRC has been described both histologically (via the study of the peritumoral immune infiltrate) (11) and at the systemic level (via the evaluation of blood parameters) (12). In this regard, blood indexes such as the neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR) or the systemic inflammation-based Glasgow Prognostic Score have shown a prognostic impact in CRC (13-15). Moreover, these studies demonstrate a lower risk of developing CRC in patients with higher levels of certain blood parameters, usually related to the inflammatory response (16).
The main aim of the study was the evaluation and quantification of the predictive character of CRC in a blood test (BT) as a possible method of evaluating the systemic state of immunosurveillance against CRC. This could be of interest for the identification of patients with the highest risk of developing CRC and optimizing the prioritization of colonoscopy waiting lists for patients that are not part of a screening program.
Material and methods
We performed a retrospective case-control study with a comparative analysis of the distribution of typical blood parameters in a routine BT. We recruited patients that underwent elective surgery for CRC in the Department of General and Digestive Surgery of our hospital from 2009 to 2013 into the case group. Patients who had an elective colonoscopy that ruled out the presence of CRC by the Department of Digestive Medicine of our hospital during the same period (2009-2013) were recruited into the control group.
The inclusion criteria of the case subjects who underwent elective surgery for CRC were the following: a) histological diagnosis of colorectal adenocarcinoma obtained by a biopsy sample from a previous colonoscopy, regardless of their stage and performed as a non-urgent surgery without any neoadjuvant treatment; and b) patients who received elective surgical treatment motivated by advanced colorectal adenomas (hairy adenomas that due to their size or the presence of high-grade dysplasia cannot be treated with a colonoscopic approach). Candidates for the study control group were patients who underwent a non-urgent colonoscopy in the medical department and were not part of the screening program and the presence of CRC has been ruled out.
BTs performed on the day prior to surgical intervention (case group) and the day prior to the completion of colonoscopy (group control) were selected for the comparative analysis. This was performed in order to obtain a representative BT of the basal status of the patients in order to allow an adequate evaluation of their systemic immunosurveillance status.
We excluded all patients with circumstances that could influence their immunosurveillance status such as a history of previous treatments with immunosuppressive drugs, patients with a pharmacological allergic history, autoimmune diseases, inflammatory bowel disease and a previous personal history of other neoplasia.
An adequate representation of patients within both groups was ensured via patient matching by sex and age. For each BT in the case group, there was a BT in the control group from a patient of the same sex and age. When there was more than one control subject matched by sex and age, control subject selection was performed by simple randomization. In cases with no control subject of the same sex and age, patients of the same sex and one year older than the case subject were selected.
The blood analytical parameters evaluated in the study were: hemoglobin (g/dl), hematocrit (%), glucose (g/dl), platelet count (x109/l), fibrinogen (g/dl), leukocytes (absolute count, x109/l), neutrophils (absolute count, x109/l and relative value, %), lymphocytes (absolute count, x109/l and relative value, %), monocytes (absolute count, x109/l and relative value, %) eosinophils (absolute count, x109/l and relative value, %), basophils (absolute count, x109/l and relative value, %), neutrophil to lymphocyte ratio (NLR, the ratio of the absolute count of neutrophils and lymphocytes [13]) and platelet to lymphocyte ratio (PLR, the ratio of the platelet count and absolute number of lymphocytes [14]).
The comparative statistical analysis of the distribution of blood analytical parameters between the study groups was performed using the Student's t test. The IBM® SPSS Statistics® statistical software support version 21 was used. The distribution of the parameters was described by mean and standard deviation and statistical significance was set at a p value < 0.05.
After the comparative analysis of the distribution of blood parameters between the study groups, a second statistical analysis was performed exclusively with the parameters for which a statistically significant distribution between the groups was obtained. A multivariate logistic regression was used for the statistical analysis. A probability formula to evaluate the best combination of blood parameters with the ability (via their interaction and mathematical combination) of probabilistic prediction of CRC presence in function of the results obtained in a BT was designed. Several mathematical predictive CRC formulae were obtained during the logistic regression steps, all with different combinations of parameters. The regression formulae with the highest probabilistic percentage of CRC presence in the BT were selected by calculating the area under the ROC curve (17).
The study was approved by the ethics and research committee of our hospital.
Results
Between 2009 and 2013, a total of 1,204 patients were selected, 320 were surgically intervened for CRC or advanced adenomas and 884 had no disease as verified by colonoscopy during the same period. Fifty-four patients with CRC and 372 patients without the disease were discarded as they did not meet the study criteria.
The case group of the study was constituted by 266 patients. The stage distribution according to the TNM classification of the AJCC (American Joint Committee on Cancer) (7) was: stage 0 or advanced colorectal adenomas (9.02%, 15 patients), stage I (15.03%, 40 patients), stage II (39.47%, 105 patients), stage III (30.82%, 82 patients) and stage IV (5.64%, 15 patients). During the initial selection of the control group, 532 patients were recruited. After the process of matching by sex and age with the case group, the control group was made up of 266 patients.
Table 1 shows the distribution by sex and age of both study groups. There was no loss of the blood analytical data as all data were stored in the computerized databases.

Comparative analysis of the distribution of blood analytical parameters within the study groups
Statistically, significant differences in the distribution of several blood parameters was shown by univariate analysis. Table 2 shows the distribution of the means of all blood parameters evaluated in the study and the statistical value obtained after the comparative analysis between both groups. The group of patients with CRC had a higher platelet count (305.80 ± 113.21 vs 231.26 ± 45.46 x109/l), fibrinogen (465.62 ± 110.36 vs 321.05 ± 70.85 g/dl), absolute leukocyte count (7.37 ± 2.40 vs 6.72 ± 1.68 x109/l), absolute neutrophil count (4.80 ± 2.18 vs 3.60 ± 1.17 x109/l) and systemic immunosurveillance scores (NLR 3.44 ± 3.38 vs 1.69 ± 0.74, PLR 213.64 ± 193.95 vs 109.41 ± 39.61). All differences were statistically significant. On the other hand, the patients in the case group had lower hemoglobin levels (12.02 ± 2.34 vs 13.81 ± 1.69 g/dl), hematocrit (38.02 ± 5.98 vs 41.95 ± 4.79%) and absolute eosinophil count (0.16 ± 0.12 vs 0.23 ± 0.12 x109/l).

Probabilistic analysis of logistic regression
After the previous univariate analysis where statistically significant differences in several blood parameters were shown (Table 1), a multivariate logistic regression analysis was performed with the intention of designing an interactive index of blood parameters with a probabilistic ability to predict CRC presence in the BT. This index could be regarded as a possible mathematical prototype to detect the disease in blood. We performed six sequences or logistic regression steps to evaluate different combinations of blood parameters. We determined the percentage of predicted probabilistic accuracy as well as the value of the area under the ROC curve (17) for each of the combinations.
After each regression step, a mathematical formulae was obtained with a predictive ability for CRC presence in the BT which was composed by the blood parameters used in the combination multiplied by a specific impact factor and a regression constant. The application of the mathematical regression formulae to the BT results obtained probabilistic values between "0" and "1". A value of "0" was equivalent to zero probability or 0% probability of CRC presence in the BT, and "1" was the maximum probability or 100% probability of the presence of the disease in the BT. Table 2 shows the logistic regression combinations performed and their probabilistic accuracy percentage. Steps 5 (five parameter combination) and 6 (six parameter combination) obtained the same percentage of probabilistic accuracy.
Finally, regression step 5 was selected as the most favorable combination of blood parameters for a predictive method for CRC presence in the BT. The step 5 combination was chosen as it was simpler than the step 6 combination and obtained the same percentage of probabilistic risk accuracy. This regression step (step 5) was constituted by five parameters: fibrinogen (g/dl), platelets count (x109/l), neutrophils relative value (%), hemoglobin (g/dl) and absolute eosinophil count (x109/l). Table 3 shows the value of the specific impact factor relative to each blood parameter in the different regression steps for the constitution of the probabilistic formulae derived from each of these steps.

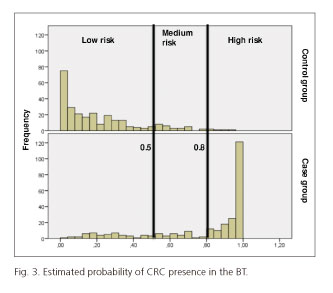
The right mathematical formulae was selected from regression step 5. This mathematical formulae consisted of a combination of the five blood parameters (fibrinogen, hemoglobin, relative neutrophil value and absolute platelet and eosinophil counts), all with a specific numerical multiplier factor plus a regression constant (Fig. 1). The behavior of the mathematical formulae obtained (Fig. 1) was evaluated, which must be understood as a parametric interrelationship index with a probabilistic ability to predict CRC presence in the BT via the calculation of the area under the ROC curve. The value obtained was 0.85 (17) (Fig. 2). Figure 3 shows the behavior of the mathematical formulae in order to evaluate its probabilistic predictive ability for the presence of CRC in the BT via its individual calculation in the 532 BTs evaluated in the study.


In order to understand the clinical application of this probabilistic formulae to predict CRC presence in a BT, the BT results in two hypothetical patients are shown:
- Subject A: hemoglobin (7.8 g/dl), platelets count (186,000 x109/l), fibrinogen (432 g/d), absolute eosinophil count (0.19 x109/l) and relative neutrophil value (73.3%).
- Subject B: hemoglobin (13.9 g/dl), platelets count (158,000 x109/l), fibrinogen (365 g/dl), absolute eosinophil count (0.34 x109/l) and relative neutrophil value (58.3%).
Using the probabilistic formulae designed in this study (Fig. 1), subject A obtained a probabilistic result for the presence of CRC in the BT of 0.86, whereas subject B had a value of 0.11. In other words, taking into account the blood values obtained in the two BT of two hypothetical patients, subject A would have a probability of 86% of presenting the disease, while subject B would have a considerably lower probability (11%).
Discussion
The present study was motivated by recent lines of research which are related to the evaluation of the immunosurveillance status or the basal protective status of the organism against neoplasia development. Our main aim was the evaluation of the BT as an exploratory method of the systemic immunosurveillance against CRC. In this sense, the identification of a possible interaction index within blood parameters for the evaluation of the basal status of immunosurveillance against CRC has a clinical interest, as patients with greater risk of disease can be identified via a simple BT (18). This would be of great interest due to its potential clinical application as a method to optimize the prioritization of the colonoscopy waiting list with regard to patients that are not part of a screening program.
We compared the distribution of several parameters of the BT within two clearly differentiated groups: a group of BTs from CRC patients (case group) and another group where the disease was excluded by colonoscopy (control group). The results of this analysis showed statistically significant differences in the distribution of several blood parameters between the study groups (Table 2). We then performed a second statistical analysis using logistical regression to include the greatest number of these parameters in a blood index, with a probabilistic ability to predict the risk of CRC presence in the BT (Fig. 1).
Currently, there are several interaction indexes of blood parameters with prognostic connotations in CRC such as the neutrophil to lymphocyte ratio (NLR), platelet to lymphocytic ratio (PLR) and the Glasgow systemic prognostic index (13-15). According to lines of investigation that indicate the presence of a certain predictive character of CRC in BT via the evaluation of the systemic status of immunosurveillance, the inter-relation index within blood parameters designed in our study would be included in the predictive field of the disease (10,16,19).
In this study, the case group (elective surgery patients with a CRC diagnosis) had statistically significant higher levels of blood parameters usually related with inflammatory processes compared to the control group. These included platelet count, absolute leukocytes count, neutrophils (absolute and relative value) and fibrinogen. In addition, the recent prognostic indexes that evaluate the deterioration of immunosurveillance at the systemic level, such as NLR and PLR, were also higher in the case group. These results are consistent with similar studies which describe the BT as a possible exploratory method to evaluate the systemic immunosurveillance of an organism against CRC by evaluating the interrelationship of some blood parameters (12-16).
The blood parametric index designed in this study (Fig. 1) was obtained via a sequence of multivariate logistic regression steps (Table 3). The index was defined by a mathematical formulae which included the evaluation of five common blood parameters: hemoglobin (g/dl), platelets count (x109/l), fibrinogen (g/dl), absolute eosinophils value (x109/l) and relative neutrophils value (%). This blood parametric interaction index could be used as a predictive mathematical method to access the probabilistic risk of CRC presence in a BT. This index obtains possible probabilistic results from "0" (null probabilistic risk of CRC presence or 0%) to "1" (maximum probabilistic risk or 100%).
There are several other blood probabilistic methods for other neoplasia such as breast cancer. In addition, there are other studies that predict neoplasia development using special and high cost BTs which assess the genetic vulnerability of blood components after they are subjected to ultraviolet radiation (23,24). However, these studies have not demonstrated similar characterization and quantification references of the predictive risk of CRC presence via a simple, economical and easily accessible medical tool such as the routine BT (18). We would like to point out that our blood mathematical formulae should not be considered as an alternative method to the currently established methods for early CRC detection but rather as an experimental mathematical method with a probabilistic ability to detect CRC presence in function of a BT result.
The relationship between inflammatory phenomena, the deterioration of the immunosurveillance status and neoplasia development has been known for a long time. However, its use as a systemic marker of immunosurveillance against neoplasia development is relatively new (10,11,19,20). Our results show differences in the distribution of several blood parameters. We found differences in parameters related to the adequate functioning of systemic immunosurveillance against neoplasia development such as the absolute count of eosinophils, basophils and lymphocytes as well as the immune ratios NLR and PLR (Table 1). These results are consistent with other studies that describe the possibility of detecting a deterioration in the systemic immunosurveillance status in a BT, with predisposition, prognostic and predictive clinical implications (16,21). The statistically significant differences in the distribution of hemoglobin and hematocrit between the study groups cannot be explained by the theory of immunosurveillance deterioration status in CRC patients, but rather it could be a consequence of physio-pathological conditioning and blood loss due to digestive bleeding in CRC (4-6).
There are limitations of the study with regard to design (retrospective case-control) that limit the strength of the scientific evidence obtained. However, the number of patients included in the study (532) as well as the matching of the control group by sex and age allowed the identification of statistically significant differences in the distribution of certain blood parameters (Table 2). In addition, a blood interaction index with a probabilistic ability to predict CRC presence in a BT (Fig. 1) was designed.
There are several studies of the evaluation of individual immunosurveillance status of CRC patients, both histologically and systemically (12-15,19,20). These are clinically relevant from the prognostic point of view and allow an improvement in CRC staging and individualized treatment by detecting patients with a greater risk of relapse (19,20). However, studies of the impact of immunosurveillance assessment for CRC as a predictor of disease development are scarce. Prizment y cols. (16) describe an inverse relationship between absolute eosinophil count and CRC incidence, a higher eosinophil count confers a protective effect against disease development. The eosinophil distribution within the study groups showed similar results (Table 2). The role of eosinophilia as a protective factor against neoplasm development is controversial (16,20), and in order to avoid misunderstandings, any patient with any allergic history (including pharmacological allergies) was excluded from the study (21). We also considered other possible interference factors in the evaluation of the baseline status of systemic immunosurveillance in the BT such as immunosuppressive or chemotherapeutic treatments, previous history of another neoplasia, as well as any non-scheduled BT (e.g., motivated by acute processes or emergency surgical intervention).
There are limitations of the study in relation to the heterogeneity of the stage distribution of the case group and the selection of the control group. Thus, the different distribution by CRC stage in the case group could mask the clinical relevance of some blood parameters, distorting or even over exaggerating them, such as the hemoglobin parameter, which is usually altered in CRC patients due to the natural physiopathology of the disease (4-6).
The performance time of the BT is also a possible criticism of the study. In the case group, BTs were obtained the day before the surgical intervention and therefore, after the diagnostic colonoscopy. In contrast, the BTs of the control group were obtained the day prior to the colonoscopy for ruling out the presence of the disease. This could be a limitation of the study, as the potential subjective effect and possible influence of the blood parameter interaction and the immunosurveillance status in the case group is unknown. In other words, the BTs were obtained from the case group in patients that knew that they had CRC, whereas the control group were unaware of their disease status. The results and the design of the blood interaction index can be easily reproduced (Fig. 1). However, the inclusion of an alternative case group in order to assess the behavior of the probabilistic CRC index (Fig. 1) in BTs taken before a diagnostic colonoscopy could provide more consistency to the results.
A selection in case subjects exclusively with initial stages of CRC would have possibly allowed a better characterization of the probabilistic index as a predictive tool for CRC presence in the BT. In this sense, the inclusion of patients with advanced stages (fundamentally stage II and III and even stage IV) has overestimated differences in the distribution of certain blood parameters and altered its correct functioning as a mathematical tool that is predictive of disease. However, we show that it is possible to characterize in a mathematical way the risk of CRC presence in the BT due to the presence of certain predictive characters of the disease in blood (10-16). This consideration constitutes an interesting research line with clinical potential in the development and improvement of CRC screening programs.
We evaluated this blood index (Fig. 1) as a method for the predictive evaluation of CRC presence in a BT by calculating the area under the ROC curve and obtained a value of 0.85 (Fig. 2). Whilst bearing in mind the limitations of the study, we can infer that there is a predictive CRC character in the BT in mathematical terms (16), which can be quantified via the application of mathematical methods. We wish to highlight the originality of our study as there is no evidence of similar publications in the sources reviewed. Obtaining an area under the ROC curve greater than 0.5 allows us to conclude that our mathematical formulae or blood CRC presence index (Fig. 1) constitutes a probabilistic approach method for the presence of CRC in a BT. In addition, it could be considered as an exploratory indicator of the systemic immunosurveillance status against the disease (17) (Fig. 2). The application of this blood index to a BT provides a probability value of CRC presence. The possible values are between "0" and "1": "0" is equivalent to zero probability of CRC presence and "1" is the maximum probability for the presence of the disease. As mentioned in the results section, the results of CRC presence were calculated (Fig. 1) via individual calculations of the 532 BTs evaluated in the study (Fig. 3).
In order to evaluate the mathematical formulae as a probabilistic screening method in the BT, the sensitivity and specificity in function of different cut-off points was calculated with the purpose of selecting the most discriminative value for the identification of the BTs with the greatest probabilistic risk of CRC presence. Three areas of probabilistic risk were used to evaluate the clinical character of the blood index for the presence of CRC (Fig. 1). These areas were: a low risk zone (with probability values in the BT of less than 0.5), a moderate risk zone (with values between 0.5 and 0.8) and a high risk zone (with probability values greater than 0.8). The selection of a critical discrimination value in the BT equal to or greater than 0.80 would provide a sensitivity and specificity of 93% and 61% respectively. The selection of the 0.5 cut-off point value would obtain sensitivity and specificity values of 82% and 88% respectively (Table 3). The selection of the optimum cut-off points (Fig. 1) should be determined after an adequate cost-sanitary evaluation with the best sensitivity/specificity profile. Assuming that the selection of values close to 1 would imply a higher sensitivity with lower specificity and the selection of values close to 0 would produce the opposite effect.
It would be of great interest to perform studies to evaluate the blood parameter in other common neoplasms. In addition, the design of new blood interaction indexes to complement those already known such as NLR, PLR or the Glasgow systemic prognostic index (13-15). Also, other blood indexes that go beyond the mere evaluation of a BT at a specific time and provide information about trends of the temporal evolution would also be of use. This would allow the implementation of the clinical information that could be obtained via a BT, improving the understanding of the complex interaction of blood parameters, inflammatory states and immunosurveillance. The probabilistic CRC index designed in this study (Fig. 1) would be an example in this regard. We consider this a prototype tool for an approach to assess the blood parameter interaction with the systemic immunosurveillance status against CRC from a mathematical point of view, after the evaluation of its probabilistic CRC predictive ability in a sample of 532 BTs.
In conclusion, our results are in agreement with other studies about the importance of the evaluation of the systemic immunosurveillance status (10,12,16,20). These results allowed the creation of a multi-parametric blood index with a probabilistic ability to predict CRC presence in a BT (Fig. 1). This would be of great interest due to its potential clinical applicability as an optimization method for the prioritization of the colonoscopy waiting list of patients that are not part of a screening program. We are aware of the limitation of the applicability of the results. In this sense, we should make it clear that this blood interaction index (Fig. 1) is not an alternative method to the currently established methods for early CRC detection. As the importance of the evaluation of systemic immunosurveillance status against some neoplasms (13-16) is well known, we encourage the development of similar studies with a greater number of patients and evaluated parameters. This would create new blood indexes for CRC. These tests and other tests with a proven clinical applicability such as NLR, PLR or the Glasgow systemic inflammatory gradation system (13-15) would provide a greater clinical impact of the information obtained from a BT. In this sense, new indexes of blood interaction could be prognostic tools and an additional element with clinical utility in the currently used tools in CRC screening.
The evaluation of the systemic immunosurveillance status via a BT is important. We encourage the development of blood indexes similar to that described here (Fig. 1) as possible methods to evaluate and clarify the impact of the systemic immunosurveillance status against certain neoplasms such as CRC. These could have a potential clinical utility in the implementation of early screening programs.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin 2015;65:5. DOI: 10.3322/caac.21254. [ Links ]
2. Sociedad Española de Oncología Médica (SEOM). Accedido el 30 de septiembre de 2015. Disponible en: http://www.seom.org. [ Links ]
3. Vogelstein B, Papadopoulos N, Velculescu VE, et al. Cancer genome landscapes. Science 2013;339:1546. DOI: 10.1126/science.1235122. [ Links ]
4. Red de programas de cribado de cáncer. Guía de control de calidad en cribado y diagnóstico de cáncer colorrectal. Disponible en: http://www.programascancerdemama.org/index.php/guia-europea-colon. Accedido el 11 de octubre de 2015. [ Links ]
5. Minozzi S, Armaroli P, Segnan N. European guidelines for quality assurance in colorectal cancer screening and diagnosis. 1st ed. Principles of evidence assessment and methods for reaching recommendations. Endoscopy 2012;44(Supl. 3):SE9-14. DOI: 10.1055/s-0032-1309781. [ Links ]
6. US Preventive Services Task Force, Bibbins-Domingo K, Grossman DC, et al. Screening for colorectal cancer: US preventive services task force recommendation statement. JAMA 2016;315(23):2564-75. DOI: 10.1001/jama.2016.5989. [ Links ]
7. Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol 2010;17(6):1471-4. DOI: 10.1245/s10434-010-0985-4. [ Links ]
8. Marcos Prieto HM, Velasco-Guardado A, Álvarez Delgado A, et al. Increasing incidence of colorectal cancer in the province of Salamanca. Comparison of two periods: 2004-2006 and 2010-2012. Rev Esp Enferm Dig 2016;108(7):417-20. DOI: 10.17235/reed.2016.3981/2015. [ Links ]
9. López-Torres Hidalgo J, Rabanales Sotos J, Simarro Herráez MJ, et al. Effectiveness of three interventions to improve participation in colorectal cancer screening. Rev Esp Enferm Dig 2016;108(6):315-22. DOI: 10.17235/reed.2016.4048/2015. [ Links ]
10. Mantovani A, Allavena P, Sica A, et al. Cancer-related inflammation. Nature 2008;454:436. DOI: 10.1038/nature07205. [ Links ]
11. Park JH, Richards CH, McMillan DC, et al. The relationship between tumour stroma percentage, the tumour microenvironment and survival in patients with primary operable colorectal cancer. Ann Oncol 2014;25:644. DOI: 10.1093/annonc/mdt593. [ Links ]
12. Kozak MM, Von Eyben R, Pai JS, et al. The prognostic significance of pretreatment hematologic parameters in patients undergoing resection for colorectal cancer. Am J Clin Oncol 2015;3:11. [ Links ]
13. Ozdemir Y, Akin M, Sucullu I, et al. Pretreatment neutrophil/lymphocyte ratio as a prognostic aid in colorectal cancer. Asian Pac J Cancer Prev 2014;15:2647. DOI: 10.7314/APJCP.2014.15.6.2647. [ Links ]
14. Arnoud J, Templeton J, Olga A, et al. Prognostic role of platelet to lymphocyte ratio in solid tumors: A systematic review and meta-analysis. Cancer Epidemiol Biomarkers Prev 2014;23:7. [ Links ]
15. McMillan DC. The systemic inflammation-based Glasgow Prognostic Score: A decade of experience in patients with cancer. Cancer Treat Rev 2013;39:534. DOI: 10.1016/j.ctrv.2012.08.003. [ Links ]
16. Prizment A, Anderson K, Visvanathan K, et al. Inverse association of eosinophil count with colorectal cancer incidence: Atherosclerosis risk in communities study. Cancer Epidemiol Biomarkers Prev 2011;20:1861. DOI: 10.1158/1055-9965.EPI-11-0360. [ Links ]
17. Florkowski CM. Sensitivity, specificity, receiver-operating characteristic (ROC) curves and likelihood ratios: Communicating the performance of diagnostic tests. Clin Biochem Rev 2008;29:83. [ Links ]
18. Universidad de León. Tarifas: Analíticas de sangre y orina. Accedido el 11 de diciembre de 2016. Disponible en: http://servicios.unileon.es/lti-ir/lti/tarifas/personal0801. [ Links ]
19. Galon J, Mlecnik B, Bindea G, et al. Towards the introduction of the "Immunoscore" in the classification of malignant tumours. J Pathol 2014;232:199. DOI: 10.1002/path.4287. [ Links ]
20. Laird B, Kaasa S, McMillan D, et al. Prognostic factors in patients with advanced cancer: A comparison of clinicopathological factors and the development of an inflammation-based prognostic system. Clin Cancer Res 2013;19:5456. DOI: 10.1158/1078-0432.CCR-13-1066. [ Links ]
21. Valdivia J. Mast cells and basophils: Its new functions in immunity. Dermatol Peru 2012;23:2. [ Links ]
22. Engkilde K, Thyssen J, Menne T, et al. Association between cancer and contact allergy: A linkage study. BMJ Open 2011;10:1136. DOI: 10.1136/bmjopen-2011-000084. [ Links ]
23. Gómez F. Evaluación cuantitativa del riesgo de cáncer de mama. Rev Med Clin Condes 2006;17:149. [ Links ]
24. Anderson D, Najafzadeh M, Gopalan R, et al. Sensitivity and specificity of the empirical lymphocyte genome sensitivity (LGS) assay: Implications for improving cancer diagnostics. FASEB J 2014;28:4563. DOI: 10.1096/fj.14-254748. [ Links ]
![]() Correspondence:
Correspondence:
José Manuel Navarro-Rodríguez.
Services of General and Digestive Surgery.
Hospital Vega Baja-Orihuela.
Ctra. Orihuela-Almoradí, s/n.
03314 San Bartolomé, Alicante. Spain
e-mail: jomanarrocir@hotmail.com
Received: 06-10-2016
Accepted: 24-05-2017
