










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkCASE REPORT
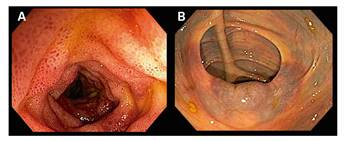
An 84-year old woman was admitted to the Emergency Room with abdominal pain and nausea of a 24 hour duration. She had a medical history of auricular fibrillation which was treated with acenocumarol. Physical examination revealed diffuse abdominal tenderness and there was no history of trauma. Laboratory tests showed a prolonged prothrombin time (> 180 seconds; normal control of 13.7 seconds) with a non-measurable international normalized ratio (> 10) and a prolonged activated partial thromboplastin time (> 240 seconds; normal range 28-40 seconds). Bowel ultrasound identified a thickening of the terminal ileum and an echogenic thickened submucosa and of the cecum walls with segments of partial loss of the wall stratification (Fig. 1A). The ileocecal valve appeared diffusely hyperechogenic (Fig. 1B). The coagulation status was corrected and an ileocolonoscopy was performed that revealed congestive terminal ileum mucosa (Fig. 2A) that caused a narrowing of the lumen. The ileocecal valve and cecum had a dark bluish colored mucosa (Fig. 2B). Biopsies samples showed foci of intraparietal bleeding which reflected intramural hemorrhage. The symptoms resolved and the bowel ultrasound was normal one month later.
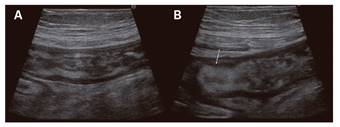
Fig. 1 A. Thickening of the terminal ileum and cecum walls with an echogenic thickened submucosa and segments of partial loss of the wall stratification. B. Hyperechogenic ileocecal valve (arrow).
DISCUSION
Spontaneous intramural intestinal hemorrhage associated with oral anticoagulation therapy is rare and often associated with an abnormal coagulation profile 1. The jejunum and ileum are the most frequently involved bowel segments 2. Clinical presentation may range from abdominal pain to intestinal hemorrhage or obstruction 1. Reported sonography findings are non-specific, as they can also occur in inflammatory conditions. The main findings include a thickened bowel wall with an echogenic submucosa that is indicative of bleeding in this layer 2) (3. It is important to recognize this clinical entity in order to avoid unnecessary interventions.
