










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Sanidad Penitenciaria
versión On-line ISSN 2013-6463versión impresa ISSN 1575-0620
Rev. esp. sanid. penit. vol.19 no.2 Barcelona 2017
Chronic acromioclavicular dislocation and torture allegations in detention
Dislocación acromioclavicular crónica y alegaciones de torturua en custodia
M. Yassine Braham, M. Jedidi, Y. Chkirbene, M. Kamel Souguir
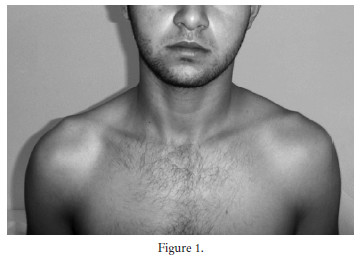
In the case that we present, we have been designated as experts to examine a 21 year old young man, who claims to be victim of physical violence perpetrated by police officers in the police station where he was on custody. Indeed, the concerned told the prison doctor during the medical visit of entry, about a complete impotence secondary to a right shoulder aggression by stick blows. The medical examination in prison highlighted painful limitation of motion of the shoulder strain with a right shoulder protruding without visible impact point. A widening of the acromioclavicular (AC) joint space was noted at the radiograph of the right shoulder. The patient was referred to the emergency of a University Hospital for specialist examination and the diagnosis of AC dislocation was confirmed by the clavicle deformation in "piano key" and the radiological appearance. No current injury was noted in this examination. In this torture allegation context, the prosecutor was notified and a judicial investigation was opened. A medical expertise was ordered.
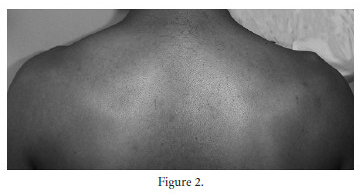
Our medical assessment, carried out 17 days after the first examination of the detainee, highlighted a distortion of the AC joint on the right with a protruding collarbone under the skin and a mobility of the distal clavicle ("piano key" sign). This deformation was associated with atrophy of the muscles of the right shoulder and right arm with a slight limitation of movement of the right shoulder. In our evaluation, we carried out a comparative examination of both upper limbs and noticed the same strain of the AC joint on the left, which is more marked on the right with a significant bump (See figure 1 and 2).
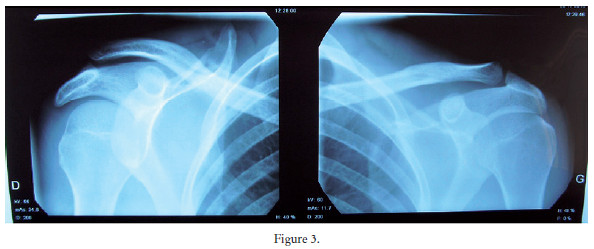
Moreover, we found no traces of violence on the skin and the neurological examination was uneventful. The radiographs of both shoulders by the Railhac incidence showed bilateral widening of the AC joint without other recent or former bone lesion (See figure 3).
We were, thus, able after expertise, to demonstrate that there is an AC dislocation of both shoulders and that it was a chronic ancient dislocation, this taking into account the bilateral nature of the dislocation, the muscle atrophy, the absence of traumatic lesions such as bruises or hematomas on the skin and the absence of traumatic lesions in the radiography. Regarding all these arguments, we concluded that patient's abuse allegations were not concordant with our findings. Seen these medical expertise data, the judge decided a dismissal and the investigation stopping.
AC dislocation represents 8% of all dislocations of the upper limbs and 12% of the shoulder joints1. It is particularly known among athletes especially in contact sports but also in road and fall accidents, the direct impact on the stump of the shoulder in adducted position is the primary traumatic mechanism2, 3 What we call chronic AC dislocation is an acute joint injury not initially operated and which can be well tolerated, particularly among the low-active individuals, little using their shoulders in their professional or sports activities4. However, in such situations, subsequent effects can occur such as a limited range of motion and pain related to the instability of the clavicle and its projection under the skin especially in thin patients4, 5. In addition, reduced strain of the injured limb can cause muscle wasting4. All of these have been taken into account in our approach and allowed to confirm the chronic nature of the dislocation and exclusion of the possibility of torture.
Finally, we emphasize the importance of the comparative clinical and radiological examination, which in this case would have directed the prison doctor to chronic and bilateral dislocation and excluded the possibility of torture in this prisoner.
References
1. Solovyova O, Judson CH, Ziegler CG, Edgar CM, Imhoff AB. Current Concepts in the Treatment of Acromioclavicular Joint Dislocations. Arthrosc J Arthrosc Relat Surg. 2013;29(2):387-97. [ Links ]
2. Brenn S, Farron A. Lésions acromio-claviculaires: Diagnostic et traitement. Rev Med Suisse. 2008;4(166):1706-11. [ Links ]
3. Fraschini G, Ciampi P, Scotti C, Ballis R, Peretti GM. Surgical treatment of chronic acromioclavicular dislocation: Comparison between two surgical procedures for anatomic reconstruction. Injury. 2010;41(11):1103-6. [ Links ]
4. Gumina S, Carbone S, Postacchini F. Scapular Dyskinesis and SICK Scapula Syndrome in Patients With Chronic Type III Acromioclavicular Dislocation. Arthrosc-J Arthrosc Relat Surg. 2009;25(1):40-5. [ Links ]
5. Babhulkar A, Pawaskar A. Acromioclavicular joint dislocations. Curr Rev Musculoskelet Med. 2014;7(1):33-9. [ Links ]
![]() Correspondence:
Correspondence:
Mohamed Yassine Braham
Email: brahammedyassine@gmail.com
Text received: 19/01/2017
Text accepted: 07/02/2017

