










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.12 no.29 Murcia ene. 2013
CLÍNICA
Influence of clinical practice in trapezius muscle myofascial trigger points in nursing students: longitudinal descriptive study
Influencia de la práctica clínica en la presencia de puntos gatillo miofasciales en el músculo trapecio de estudiantes de enfermería. Estudio longitudinal descriptivo
Martín Tuda, Cristina*; Soto Vidal, Concepción**
*Graduate in Physiotherapy. Salamanca University. E-mail: crismartu@gmail.com
**Graduate in Physiotherapy. Professor of Physiotherapy Department. Alcalá de Henares University. Spain
ABSTRACT
Aim: To observe whether the tasks performed by nursing students during their third year of nursing degrees have an influence on the state of MTP of their trapezius muscle.
Participants and Methods: 30 third-year students from Alcalá de Henares University College of Nursing were evaluated. Exclusion criteria: to suffer any sense or trophic muscular disorder, to have begun or be receiving any influential treatment. A questionnaire about the types of tasks they carry out and other sociodemographic and academical work factors were done. Students were assessed to check the presence of some MTP in their trapezius, describing its active or dormant state through diagnostic criteria, their pressure pain threshold (measured with an algometer) and active ranges of cervical movements were also recorded. All measurements were taken before and after one month of the experiment. Through the statistical analysis the data collected in the questionnaire was compared with the state of the MTP in both moments, with a p<0.05 and a 95% confidence interval.
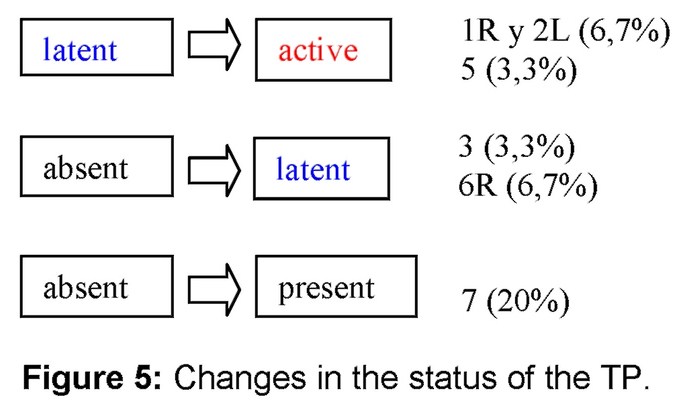
Results: all the subjects were women who over the course of the experiment recorded a 1.8- upper scoring on the visual analogue scale, they showed an average increase of 1.55o in the cervical ranges of motion, except flexion; and the pressure pain threshold rose an average 0.139 kg/cm2. Trigger points (TP) 1 and 2 changed from dormant to active state on 6,7% of the subjects, and the TP5 on 3,3%. At the end of the experiment the TP6 appeared as 6,7% of them.
Conclusions: tendencies have been observed among the analyzed variables which allow the proposition of more specific studies about biological and socio-labour factors linked to MTPs in order to establish physio-therapeutic efficient strategies for incorporation into the professional world.
Key words: myofascial trigger point; nursing; student; prospective study; internship; pain.
RESUMEN
Objetivo: Observar si la práctica clínica de estudiantes de enfermería influye en el estado de PGM en el trapecio.
Participantes y métodos: Estudio longitudinal descriptivo en el que se evaluaron 30 estudiantes de tercero de la Escuela Universitaria de Enfermería de Alcalá de Henares. Criterios de inclusión: iniciar su primer período de prácticas tras la primera sesión de valoración. Criterios de exclusión: presentar alteración muscular sensitiva o trófica, estar realizando o iniciar algún tratamiento influyente. Se pasó un cuestionario sobre tareas desempeñadas en sus prácticas clínicas y otros factores sociodemográficos y del entorno académico-laboral. Se valoraron: la presencia de puntos gatillo miofasciales (activos y latentes) en el trapecio según criterios diagnósticos, el umbral de dolor a la presión (con algómetro), y los rangos de movimiento cervical activo. Todas las medidas se tomaron antes y después de un mes de prácticas. En el análisis estadístico se compararon los datos recopilados en el cuestionario con el estado de los PGM en los dos momentos, considerando una p<0.05 y el intervalo de confianza del 95%.
Resultados: Todos los participantes fueron mujeres, que tras el período de prácticas clínicas, registraron una puntuación 1.8 superior en la escala analógica visual, mostraron un incremento medio de 1,55o en los rangos de movimiento cervical, salvo en la flexión; y el umbral de dolor a la presión aumentó de media 0.139 kg/cm2. Los PG 1 y 2 cambiaron de estado latente a activo en un 6,7% de sujetos, y el PG 5 en un 3,3%. Al final del período el PG6 apareció en el 6,7%.
Conclusiones: Se han observado tendencias en las variables analizadas que permiten plantear el estudio más específico de factores biológicos y sociolaborales influyentes en la presencia de PGM, para establecer estrategias fisioterápicas eficientes antes de la incorporación al ámbito profesional.
Palabras clave: punto gatillo miofascial; enfermería; estudiante; estudio prospectivo; prácticas; dolor.
Introduction
The pain caused by the presence of myofascial trigger points (MTP), responsible for the Myofascial Pain Syndrome (MPS), is very common, particularly after a trauma or sustained muscle fatigue. The prevalence of MTP has been increasing in recent years, being more frequent location the trapezius muscle (1).
The signs and symptoms related to MPS (head and neck pain, muscle stiffness, restriction of movement, dizziness, sweating, insomnia...) limit daily activities, with a very high recurrence rate, and they may persist for long periods. Moreover, the MPS never disappear completely if it is not treated effectively (2).
Epidemiological data about MPS indicate that it is the most common diagnosis in both genders. Cervical pain is more common in women, and its prevalence increases gradually with age. It can be associated with a lower socio-economic status and occupational factors (static or repetitive tasks, uncomfortable positions, heavy loads, or physically demanding work) (3). Some biological aspects such as hormonal differences, size and muscle composition also influence the presence of stiffness associated with MTP in trapezius muscle and the preponderance of traumatic injuries among women (2). It is also believed that there are significant associations among co-morbidities, old neck injury and gradual cervical pain. On the other hand, psychosocial differences (labour demand, physical and mental stress at work and at home, social support... ) related to musculoskeletal pain, determine a higher absenteeism among women (3).
Within the occupational groups, nurses state as one of the most commonly affected groups by musculoskeletal disorders (4-6). The physical hard work added for consecutive days, psychosocial factors (premenstrual tension (7) and high mental pressure), and to have children act as risk factors to suffer from severe neck pain and to increase the prevalence of MPS. (8,9)
The nursing student collective, subject of study of the present work, can also be affected by MTP at reasonably high rates. (10)
Despite the extensive research about MPS, its cause and intrinsic nature are still not well understood in young subjects, but are common reason of musculoskeletal pain. It is possible that the MTP that they developed in pre-university schooling years can persist for years and become a serious problem in old age(11). Lucas et al(1) examined asymptomatic subjects belonging to university staff and voluntary students, and detected that, among the muscles of shoulder blade positioning, upper trapezius is the first location in order of prevalence of latent MTP. Taking into account that postural disorders, acute traumas, muscular and/or psychological stress (2)(12) are the most common causes of MTP related to neck pain, it is suggested that a high occupational exposure to both physical and psychological factors, from the role of student to active professional, may be the primary cause of the increase in back pain (13), which is a health condition of high prevalence that largely afflicts University undergraduates (14).
In this way, the concept of selecting changeable personal characteristics in nursing students can be regarded as an alternative to occupational prevention strategies in working professionals. (12)
Physiotherapy treatment aimed at the MPS should address simultaneously the symptomatic MTP and its underlying causes. This should be carried out by a variety of effective techniques, including the new physiotherapeutic approaches described in the literature, i.e., manual techniques (myofascial release and articular methods), therapeutic education to the patient- through information about contributing factors in cervical pain and its related disability (3)-, postural hygiene, -which appears to be effective at reducing the prevalence of symptoms (15)-, and attenuation techniques developed since the new etiological concepts (16). Specifically the therapies with exercise appear to be more beneficial for neck disorders with or without headache to improve pain and satisfaction of the patient (17, 18).
This work is devoted to the study of musculoskeletal and physical demands playing an important role in the appearance and perpetuation of MTP (17, 19-21). This will prompt the development of effective (preventive and therapeutic) physiotherapy treatments (22), readily to be implanted at the nursing academic field as a model of health care profession.
Main objective: to observe if there is relationship between the professional activities developed by third-year nursing students during their clinical practice and socio-demographic and academic-labor context characteristics, respect to the presence and/or the state of MTP in their trapezius muscle.
Participants and methods
Subjects of study
In this prospective longitudinal descriptive study we evaluated 30 third-year students belonging to the College of nursing of Alcalá de Henares in the 2010-11 academic year, during their first period of clinical practice November-January.
We used a non-probability of convenience technique of sampling, all subjects fulfilled the condition of being a third-year student of Nursing going to begin their period of clinical practice, and they could be in the age range 18-65 years (inclusion criteria).
We established as exclusion criteria: the presence of some kind of alteration of sensation or muscle trophism, isolated or due to Fibromyalgia, degenerative or neurological disease (multiple sclerosis, amyotrophic lateral sclerosis, myopathies, medullary syndromes, ...); be conducting or having intention to start, during the period of study, some kind of treatment (pharmacological, physiotherapist, or other) which affected direct and/or indirectly symptoms triggered by the trapezius muscle MTP.
The sample of the study was formed by women, right-handed with respect to dominant hand, and who carried out 35 weekly hours of clinical practice during the period of study. Although most of the subjects were aged between 19 and 25, there were three participants aged 41, 46 and 50.
Procedure
From previous studies (1, 11), by comparison of proportions and stockings, we have obtained a sample size of 319 subjects. This is a pilot study in which 30 students attended.
Prior to the start of the period of clinical practice (October 2010) the principal investigator held a joint meeting to recruit the participants, and to make an appointment with them to the first individual session. At this joint meeting, they signed their informed consent and they completed a general questionnaire about sociodemographic aspects and academic-labour environment, and we explained them how to fill out the International Physical Activity Questionaire (IPAQ) and the card of clinical practice that they would receive and forward by e-mail.
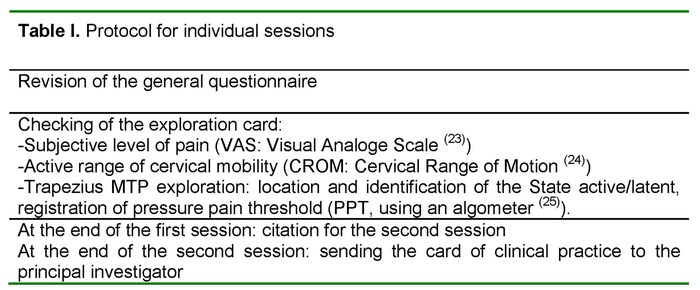
In each individual session, before and after a month of practice, we proceeded according to the above in table I, indicating also the instruments used in the measurements. We applied the recognized diagnostic criteria described by Travell and Simons (17, 19) to explore the MTP.
Ethical aspects
This study was approved by the Committee on ethics of the "Príncipe of Asturias" University Hospital (Alcalá de Henares).
Response variables
With regard to the main objective, the independent variable was the task carried out by the student in their clinical practice, and the main dependent variables were the presence of any MTP in the trapezius muscle and its status, active or latent. The subjective level of pain, range of motion of the cervical spine and the PPT (pressure pain threshold, associated with the MTP) were also dependent variables. Values were compared before and after the internship.
Regarding the secondary objectives, the rest of variables, were independent: smoking, phase of the ovarian cycle, additional work, level of physical activity, previous episodes of neck pain, pretreatment.
Analysis of data
A database was edited with the gathered information using Microsoft Excel 2003 (©2004 Copyright Microsoft Corporation), and its analysis was made with the statistical programmes Graphpad InStat 3.10 (Copyright 1992-2009 by Graphpad Software, Inc.) and PASW Statistics 18.
The t test for related samples was applied for quantitative variables and the Wilcoxon test when the assumption of normality was not met. A value P < 0,05 was considered significant.
The 95% confidence interval (95% I.C) is expressed in cases of normal distribution. Pearson Chi-square and Fisher exact test were used to check the possible association between categorical variables: smoking, phase of the ovarian cycle, level of physical activity, work, previous episode, previous treatment, with respect to presence or status of MTP.
Results
We started from a non-normal distribution.
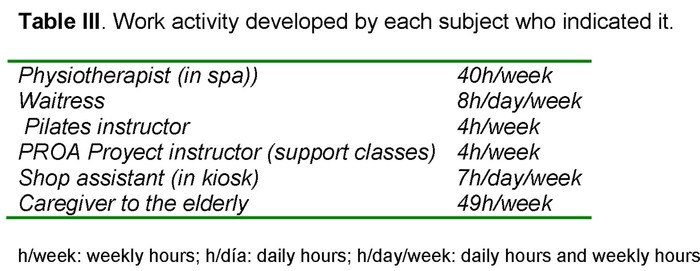
The descriptive analysis of the sample is exposed through absolute and relative frequencies in Tables II and III.
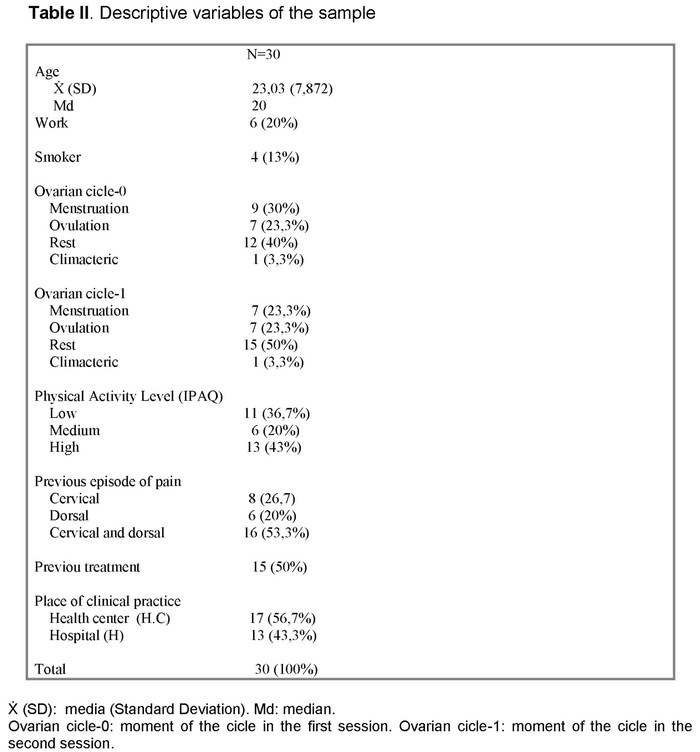
A 26.70% of subjects showed some current or persistent musculoskeletal diagnostic: osteoporosis, migraines, cervical discal crushing, recurrent contractions, painful shoulder, low back pain, malformation of the femur (flat trochlear angle).
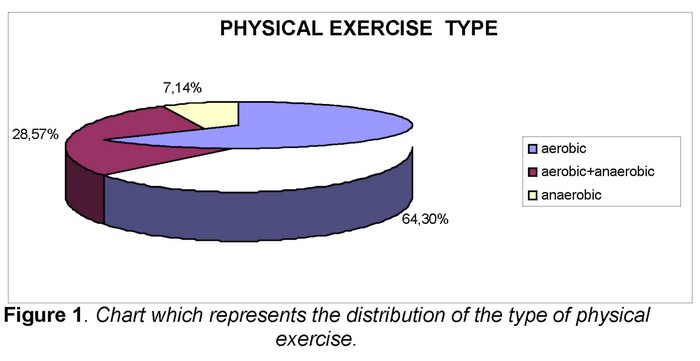
The 46,6% of the total of subjects has acknowledged doing some type of physical exercise represented in Figure 1.
During the last year all the participants had experienced some episode of cervical or dorsal pain associated with inadequate and maintained positions, prolonged sitting position during classes, the study and the use of the computer, muscular strain, tension and stress associated with exam time, load weight (backpack, bag,...), soft mattress, lack of physical activity... in short, physical and positional factors.
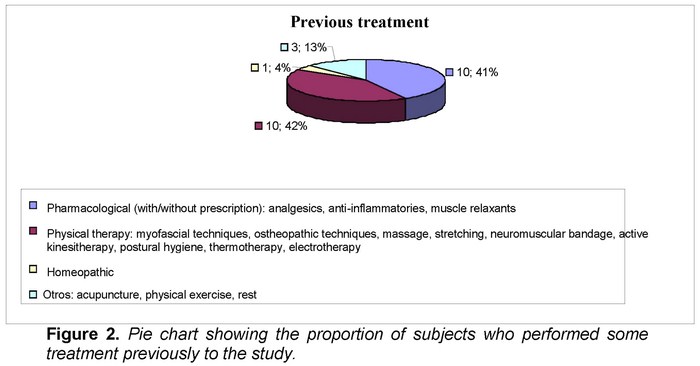
But only half of the subjects had made, previously this study, some type of treatment (Figure 2) due to cervical or dorsal pain.
At the beginning of this study, the 63,3% of students indicated cervical or dorsal pain (according to the prevalence of the different regions, showed in Table I), and among them, the 21,1 % expressed to feel any limitation in their cervical movement. The duration of this episode is reflected in Figure 3.
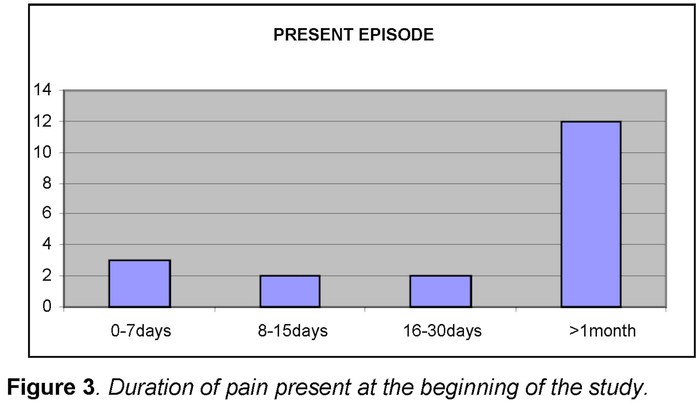
The limitation in any movement was described by subjects with duration of pain more than 16 days.
Clinical practice-related activities:
The following data have been got from the information provided about the tasks as future professionals in nursing:
The tasks associated to cervical or dorsal pain were:
- mobilization of patients: it involves load weight, pull of sheets in bedridden patients, to perform transfers and postural changes;
- channelling of peripheral roads (removal of blood, serum therapy ,...), record of vital signs (blood pressure with stethoscope or pressure gauge,...): they carry maintain a posture of trunk and cervical flexion to apply the technique using the upper limbs;
- healing of ulcers, bandages: they pose adopt a flexed posture or semiflexion of trunk to access the corporal area of the patient, or support the weight of the limb to be treated, together with maintaining visual contact with the patient, which produces sustained flexion or extension of the cervical spine;
- hold weights: material (infusion pumps,...) during the move of patients; some body region (head, limbs) during grooming, a baby during daily intakes;
- make beds: demand to adopt a forward-flexion position of trunk and at the same time move the cervical spine and upper limbs beyond the neutral zone;
- record data in computer without maintaining a suitable posture of discharge due to deficits of furniture (height table-chair, absence of back and armsrest);
- sustained surgery hours in unsuitable posture owed to deficits of furniture (sitting position on backless stools).
The described symptomatology includes: pain, overload and tension muscle, neck stiffness, sensation of cramp or stitch; and it is classified as acute, constant or which appears during the activity, if this is lengthy, and the symptom is kept later if the cervical and dorsal area is still using; either it reappears performing another task involving these regions. If the pain starts at the lumbar level sometimes it radiates to the dorsal and cervical area. In some cases it can be accompanied even by throbbing headache, dizziness, loss of concentration.
Stress and tiredness during the day favour to symptoms appear or be maintained. Mental stress before the execution of a task for the first time, contributes to the presence of muscle tension. Hospital practices involve a greater sense of stress due to the inherent rhythm of care required by the patients-users of emergency services.
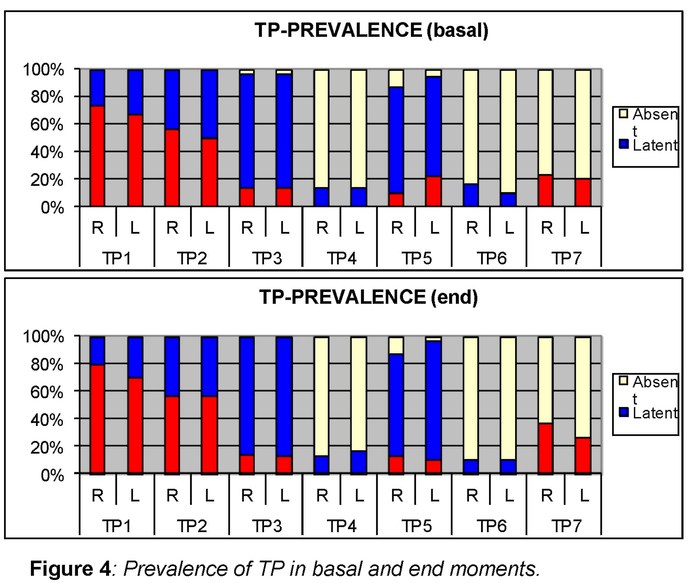
Trapezius Muscle myofascial trigger point (TP) (figures 4 and 5).
We observed that the order of higher to lower prevalence of the different MTP before and after the study period differs only in late positions:
TP1 and TP2-TP3-TP5- Right (R) TP6-TP7-TP4- Left (L) TP6 in the basal moment; TP1 and TP2-TP3-TP5-TP7-TP4-TP6 in the final moment.
Regarding the TP7, the described sensations (chills, tingling, tickling) and its location do not adhere rigorously to what is stated in the Manual of Travell and Simons (4).
Although they were registered as "Present TP7", to distinguish those subjects who did not manifest any sensation, we take into account that they could be included in the "absent" category and therefore it would be the lowest prevalent TP (4).
The results on changes in quantitative variables were:
> Subjective level of pain (VAS: Visual Analogue Scale):
An increase of 1.8 points in the EVA at the end of the period. Statistically significant difference (P<0.001) with a 95% I.C (1,143-2.531)
> Active Cervical Range of Motion:
Except in flexion, in the rest of neck movements, we observed a slight increase in articular range after the period of study, not being statistically significant (P>0.05), except in extension and lateral right flexion where we observed significance (P<0.05) (see table IV).
> Pressure pain threshold (see table IV):
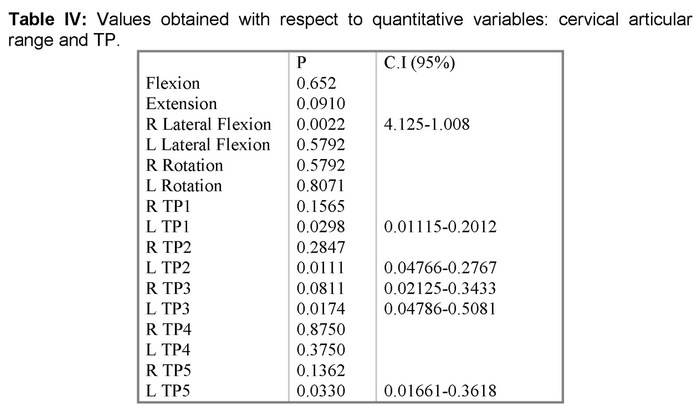
It was high in all TP, except in the LTP4, at the end of the study period. The differences were found statistically significant in the case of the left 1, 2, 3 and 5 TP.
We could not analyze TP6 by lack of subjects (we only assessed its prevalence before and after).
Ovarian cycle-TP
In this study we detected most frequently active TP during menstruation and latent TP during ovulation.
The only student rated "climacteric" presented TPs according to the majority of subjects studied (tables II and III), except the basal LTP6 and the final R Tp6 and LTP6, that were found in a latent state.
Tobacco-TP
In the present sample we did not observe significant differences in the existence of any TP in the trapezius muscle with regard to be smoking or not (P>0.05).
Previous diagnostic-TP
The results have not showed statistical significance (P>0.05) about the possible association between medical diagnosis of a musculoskeletal problem and the presence of TP in the trapezius muscle.
Previous treatment-TP
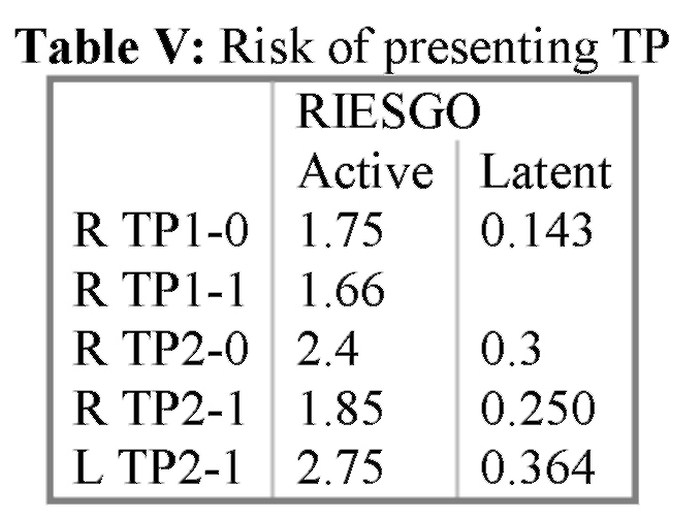
The estimate of risk was only possible in cases with statistical significance: RTP1, RTP2 and L-0 (basal) TP2.
The subjects that made treatment at some time, seem to have some probability of present active or latent TP. Estimated risk values are presented in table V.
Job-TP
For none of the registered TP we observed statistically significant relationship in terms of the performance of an occupation combined with the academic activity (P>0.05).
Physics activity level (PA)-trigger points (TP)
The Table VI complements the results exposed below, in the basal (0) and end (1) moments.
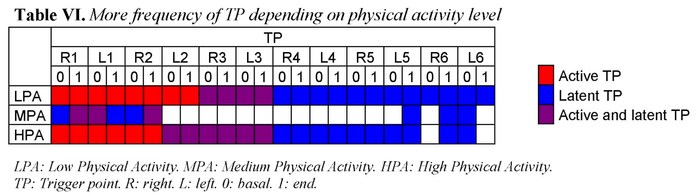
RTP1-1, LTP1-0 and RTP2-1: we observed that the students with medium level of PA have the same proportion of TP to dormant assets.
RTP3-0, RTP3-1, LTP3-0 and LTP3-1 were observed most frequently as latent TP in all levels of PA.
TP4 left and right in the basal and final moments: were only detected in a latent state. RTP5-0: At all levels of PA was more frequent to find it latent than active (considering what was observed in table II).
As latent it is more present in low and high level of PA. We detected a more case of active TP in medium PA than in the high level. None at low level.
RTP5-1 and LTP5-0 were found in greater proportion in a latent state than in active. We observed them as active, to the same extend, in middle and high levels. And none at low level.
LTP5-1: For all levels of PA, we observed it more often in latent state than active. But we did not identified any active TP in mid-level PA. It was most presente as active in low and high level of PA.
We registrated TP6 (left and right) in the basal and final moments only in latent state, at all levels of PA.
RTP7-0 and LTP7-0 were observed more frequently in the following order with respect to the level of PA: mid-low-high.
RTP7-1: Its presence is similar at all levels of PA, although in order: mid-low-high.
LTP7-1 was present from highest to lowest frequency in low-mid-high PA.
We obtained statistical significance (P<0.05) on: RTP1 and LTP2-1.
Centre for clinical practice-TP
We found statistical significance (P<0.05) in: RTP3-1, LTP3-1, RTP4. According to the data, it seems that the internships in Health Center involved more likely (risk 1.44) to submit latent TP in the dorsal region (indicated TP3) PG. We found absent the 4RTP in subjects located in centre of health at a rate of 1.44 regarding students with internship in hospital.
Discussion
The present work aims to explain the importance of the knowledge of socio-labour factors influencing the cervico-dorsal pain linked to trapezius muscle TP of the future professionals of nursing, with the purpose of contributing to the development of strategies for prevention (21.26).
According to the obtained results, performing tasks that involve no neutral postures for the column, and a maintained muscle activation to stabilize the column while a manual technique, seems to increase the subjective pain sensation in the cervical-dorsal region. Although pain may be related to limitation of the articular movement(11) in this study we did not observe affectation about the mobility of the cervical spine (P>0.05). The basal measurement, carried out during the period of theoretical classes for the first semester, which involve hours in sitting position in the classroom (paying attention to the professor and to audiovisual media), might explain that the range of motion detected at the end of the day in the classroom, was lower than after a period of clinical practice, in which the student is often physically more active, affecting in this way the flexibility of the tissues of the cervical spine, and showing thus greater articular extent, though not in a meaningful way, as we observed in this study sample.
According to the results, we saw a tendency to tolerate more pressure in the TP at the end of the internship period. The perception of this type of stimulus after a stressful day and continuous activity, might easing through mechanisms of descending modulation, by prevailing feeling of general tiredness or mental tension accumulated. Having found a highest pressure pain threshold in the left TP, considering that the right hand was dominant in all the subjects of the study, seems coherent if muscle solicitation is less when they perform manual techniques that involve awkward postures (25).
Data about the moment of the ovarian cycle do not allow to glimpse a clear relationship in all TP due to the small sample size, since there are not enough subjects to include in all categories of the classification.
According to the literature, PPT can vary during the menstrual cycle, by which should carry out all measurements of PTT in the second week of the menstrual cycle, to achieve homogeneous conditions and so, to ensure that any symptom of premenstrual pain or during the menstruación does not affect the PPT (27, 28). The study of the possible association between the state of the TP in the trapezius muscle and the time of the ovarian cycle, would require a specific inquiry controlling the influence of other factors of diverse nature.
With respect to the variable "smoking", the analysis did not provide conclusive results. From the published studies, which captured this variable, only one brings that evaluated smokers had 1.97 times more probability of experiencing back pain than non-smokers (3). In other references, either they did not associate the tobacco with musculoskeletal disorders among Australian rural students of nursing, or they did not conclude anything about it (5, 9 10).
On the other hand, the low percentage of students with a diagnosis of musculoskeletal problem and occupational activity coupled with their academic day, do not make possible to establish any trend about their possible association with the presence of TP in the trapezius muscle. We could propose the study of subjects with a common diagnosis and to observe them about the presence of TP, given the existence of musculoskeletal risk factors among nurses (5,10). And we would need a larger sample to analyze, from a more homogeneous classification, with regard to its type of occupation and its working day; however, according to several publications, to carry out a professional activity either sedentary or involving physical exertion, repetitive tasks, stress,... favours the presence of back pain, both acute episodes and with tendency to chronicity (1, 2 4 13). Hence the importance of knowing influential factors which would allow to prevent the occurrence and chronicity of musculoskeletal pain according to the type of work activity.
With reference to the level of physical activity, we have detected in this sample that students with a medium level of physical activity are less likely to experience TP. This trend could lead to study thoroughly the most favourable physical activity level depending on the work activity, on the basis of previous publications, that hypoactivity time (category of low level of physical activity) is among the factors associated with back pain in university students of health areas (29). In addition, to think that intense physical exercise increases the "risk" of TP may not be inconsistent, considering the fact of working certain muscle fibers in a repetitive manner and without tissue recovery period (16, 30).
Taking into account the center of clinical practice, the tasks performed by students in health centres mostly involve spending time in sitting position, (surgery times with patients, procedure tasks assisting the function of the doctor), besides common tasks with certain services in the hospital-extractions, cures, record of vital signs,...-which involve no neutral positions for the column. We suggest that the limited space of a surgery allows less physical shifts which could relieve muscular tensions accumulated by the maintenance of a posture in prolonged sitting position. Hours opposite the computer, on not ergonomic furniture, and handling the keyboard without support, could suggest that the dorsal area, was exposed to the development of PG since it include partipating muscles in the movements of the upper limbs (1). We propose to extend the period of continued exposure of subjects to activities that they develop during their clinical practice, and to focus on a specific context (hospital service or health center), to see what happens with the variables expouned in this paper.
Conclusions, limitations and usefulness
Although the results do not show statistical significance, we have been observed trends regarding the analyzed variables that allow to focus on research into influential factors in the emergence or perpetuation of MTP in the trapezius muscle.
Despite the limitations of the present study in terms of the reduced sample size and composition only by female subjects with variability of biological and occupational conditions, we consider that an exhaustive and specific knowledge of biological and socio-labour aspects would help to see their role in the emergence and state of trapezius muscle MTP, as frequent musculoskeletal problem also in young subjects in process of incorporation into a professional activity in the field of health, as nursing is.
Acknowledgements
I would like to thank the collaboration during the development of this study: Carlos Gutiérrez Ortega, participating students of nursing, fellows of Manual Physiotherapy Master, friends and family, who contributed with their presence and encouragement to reach the final of this work of research.
References
1. Lucas KR, Rich PA, Polus BI. How common are Latent Myofascial Trigger Points in the scapular positioning muscles? J Muscoskel Pain. 2008; 16(4): 279-86. [ Links ]
2. Gerwin RD. Classification, Epidemiology, and Natural History of Myofascial Pain Syndrome. Curr Pain and Headache Rep. 2001; 5(5): 412-20. [ Links ]
3. Côté P, Cassidy JD, Carroll L. The Factors Associated With Neck Pain and Its Related Disability in the Saskatchewan Population. Spine. 2000; 25(9): 1109-17. [ Links ]
4. Simona M, Tackenberga P, Nienhausb A, Estryn-Beharc M, Conwayd PM, Hasselhorn H-M. Back or neck-pain-related disability of nursing staff in hospitals, nursing homes and home care in seven countries- results from the European NEXT-Study. Int J Nurs Stud. 2008; 45: 24-34. [ Links ]
5. Smith DR, Mihashi M, Adachi Y, Koga H, Ishitake T. A detailed analysis of musculoskeletal disorder risk factors among Japanese nurses. J Safety Res. 2006; 37: 195-200. [ Links ]
6. Lin TY, Teixeira MJ, Fischer AA. Work-related musculoskeletal disorders. In: Fischer, editor. Myofascial Pain: Update in Diagnosis and Treatment: AA. Philadelphia: W.B. Saunders Company; 1997. p. 113-8. [ Links ]
7. Chesterton LS, Sim J, Wright CC, Foster NE. Interrater Reliability of Algometry in Measuring Pressure Pain Thresholds in Healthy Humans, Using Multiple Raters. Clin J Pain. 2007; 23: 760-66. [ Links ]
8. Warming S, Precht DH, Suadicani P, Ebbehøj NE. Musculoskeletal complaints among nurses related to patient handling tasks and psychosocial factors-Based on logbook registrations. Appl Ergon. 2009; 40: 569-76. [ Links ]
9. Smitha DR, Satob M, Miyajimab T, Mizutania T, Yamagata Z. Musculoskeletal disorders self-reported by female nursing students in central Japan: a complete cross-sectional survey. Int J Nurs Stud. 2003; 40: 725-9. [ Links ]
10. Smith DR, Leggat PA. Musculoskeletal disorders among rural Australian nursing students. Aust J Rural Health 2004; 12: 241-5. [ Links ]
11. Cimbiz A, Beydemir F, Manisaligil U. Evaluation of Trigger Points in young subjects. J Muscoskel Pain. 2006; 14(4): 27-35. [ Links ]
12. Hou C-R, Tsai L-C, Cheng K-F, Chung K-C, Hong C-Z. Immediate Effects of Various Physical Therapeutic Modalities on Cervical Myofascial Pain and Trigger-Point Sensitivity. Arch Phys Med Rehabil. 2002; 83: 1406-14. [ Links ]
13. Mitchell T, O'Sullivan PB, Burnett AF, Straker L, Rudd C. Low back pain characteristics from undergraduate student to working nurse in Australia: A cross-sectional survey. Int J Nurs Stud. 2008; 45: 1636-44. [ Links ]
14. Stock C, Mikolajczyk RT, Bilir N, Petkeviciene J, Naydenova V, Dudziak U, et al. Gender differences in students' health complaints: a survey in seven countries. J Public Health. 2008; 16: 353-60. [ Links ]
15. Tezel A. Musculoskeletal complaints among a group of Turkish nurses. Int J Neurosci. 2005; 115: 871-80. [ Links ]
16. McPartland JM, Simons DG. Myofascial trigger points: translating molecular theory into manual therapy. J Man Manipulative Ther. 2006; 14(4): 232-9. [ Links ]
17. Simons DG. Review of enigmatic MTrPs as a common cause of enigmatic musculoskeletal pain and dysfunction. J Electromyogr Kinesiol. 2004; 14(1): 95-107. [ Links ]
18. Gross A, Kay T, Hondras M, Goldsmith C, Haines T, Peloso P, et al. Manual therapies for mechanical neck disorders: a systematic review. Man Ther 2002; 7(3): 131-49. [ Links ]
19. Simons DG, Travell JG, Simons LS. Dolor y disfunción miofascial. 2a ed. Madrid: Médica Panamericana; 2001. [ Links ]
20. Fernández-de-las-Peñas C, Cuadrado M, Pareja J. Myofascial trigger points, neck mobility and forward head posture in episodic tension type. Headache 2006; 47(5): 662-72. [ Links ]
21. Friedrich M, Hahne J, Wepner F. A controlled examination of medical and psychosocial factors associated with low back pain in combination with widespread musculoskeletal pain. Phys Ther. 2009 Aug; 89(8): 786-803. [ Links ]
22. Mitchell T, O'Sullivan PB, Burnett A, Straker L, Smith A, Thornton J, et al. Identification of modifiable personal factors that predict new-onset low back pain: a prospective study of female nursing students. Clin J Pain. 2010 May; 26(4): 275-83. [ Links ]
23. Carlsson AM. Assessment of Chronic Pain. I. Aspects of the reliability and validity of the Visual Analogue Scale. Pain. 1983; 16: 87-101. [ Links ]
24. Prushansky T. Cervical motion testing: methodology and clinical implications. J Manipulative Physiol Ther. 2008 September; 31(7): 503-8. [ Links ]
25. Fischer AA. Pressure algometry over normal muscles. Standard values, validity and reproducibility of pressure threshold. Pain. 1987; 30: 115-26. [ Links ]
26. Nussbaum EL, Downes L. Reliability of Clinical Pressure-Pain Algometric Measurements Obtained on Consecutive Days. Phys Ther. 1998; 78(2): 160-9. [ Links ]
27. Rhudy JL, Bartley EJ. The effect of the menstrual cycle on affective modulation of pain and nociception in healthy women. Pain. 2010; 149: 365-72. [ Links ]
28. Martin VT. Ovarian Hormones and Pain Response: A Review of Clinical and Basic Science Studies. Gend Med. 2009; 6(Theme): 168-192. [ Links ]
29. Camargo DM, Orozco LC, Hernández J, Niño GI. Dolor de espalda crónico y actividad física en estudiantes universitarios de áreas de la salud. Rev Soc Esp Dolor. 2009; 16(8): 429-36. [ Links ]
30. Vázquez E, Cascos J, Gay C. Myofascial pain syndrome associated with trigger points: A literature review. Med Oral Patol Oral Cir Bucal. 2009 Oct; 14(10): 494-8. [ Links ]

