










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.15 no.44 Murcia oct. 2016
CLÍNICA
Education effectiveness in diabetes mellitus type 1 management made by children's caregivers
Eficácia da educação no manejo do diabetes mellitus tipo 1 realizado por cuidadores de crianças
Eficacia de la educación en el tratamiento de la diabetes mellitus tipo 1 realizado por cuidadores de niños
Pedrosa, Karilena Karlla de Amorim*; Pinto, Juliana Teixeira Jales Menescal**; Arrais, Ricardo Fernando***; Machado, Regimar Carla**** and Mororó, Deborah Dinorah de Sá*****
*Nurse. Master in Nursing by the Graduate Program in Nursing of the Federal University of Rio Grande do Norte (UFRN). E-mail: karilena pedrosa@hotmail.com
**Nurse. Master in Nursing by the Graduate Program in Nursing of the Federal University of Rio Grande do Norte (UFRN). Professor at the Nursing School of Natal at UFRN. Natal/RN.
***Ph.D. in Medicine from the Federal University of São Paulo (UNIFESP). Professor at the Pediatric Department of the Federal University of Rio Grande do Norte (UFRN). Coordinator of the Diabetes Mellitus Program of UFRN Pediatric Hospital. Natal/RN.
****Nurse. Ph.D. in Science by the Program of Cardiovascular Surgery of the Federal University of São Paulo (UNIFESP). Professor at the Graduate Program in Nursing of the UFRN, Natal/RN.
*****Nurse. Master in Nursing by the Graduate Program in Nursing of the Federal University of Rio Grande do Norte (UFRN). Residence Coordinator Multidisciplinary Integrated Health, Pediatric Nursing practice area, Pediatric Hospital of UFRN. Natal/RN, Brazil.
ABSTRACT
Objective: To analyze the effectiveness of health education in the management of type 1 diabetes mellitus provided by caregivers of children.
Methods: This is a descriptive study with cross-cut and quantitative approach. We used the instruments: Knowledge Quiz Diabetes Mellitus and Self-efficacy Scale in Diabetes Management, adapted and validated in Brazil.
Results: About knowledge of caregivers, 72% had a satisfactory score. Most of them can perform the treatment (80%), and 24% do not trust the skill; 72% of respondents can recognize hyperglycemia and 96% can recognize hypoglycemia; 80% apply the correct technique of insulin administration; 80% manage to keep the recommended diet. However, 16% said they did not know to replace correctly.
Conclusion: The majority of caregivers of children with type 1 diabetes mellitus have good knowledge about the disease, and disease management performed by these caregivers is satisfactory in general. However, there is a need to intervene in some ways, changing attitudes to cope more adequately with the disease, as well as improving the effectiveness of diabetes education.
Keywords: Diabetes Mellitus; Type 1; Health Education; Child; Nursing; Caregivers.
RESUMO
Objetivo: Analisar a eficácia da educação em saúde no manejo do Diabetes Mellitus tipo 1 realizado por cuidadores de crianças.
Métodos: Trata-se de um estudo descritivo com recorte transversal e abordagem quantitativa. Utilizaram-se os instrumentos: Questionário de Conhecimento do Diabetes Mellitus e Escala de Autoeficácia no Manejo do Diabetes, adaptados e validados no Brasil.
Resultados: Em relação ao conhecimento dos cuidadores, 72% obtiveram escore satisfatório. A maioria consegue realizar o tratamento (80%) e 24% não confia na sua habilidade; 72% dos entrevistados conseguem reconhecer a hiperglicemia e 96%, a hipoglicemia; 80% aplicam a técnica correta de administração da insulina; 80% conseguem manter a dieta recomendada, no entanto 16% afirmaram que não sabiam substituir corretamente.
Conclusão: a maioria dos cuidadores de crianças com Diabetes Mellitus tipo 1 possuem bom conhecimento sobre a doença, e o manejo da doença realizado por esses cuidadores é satisfatório de um modo geral, no entanto há a necessidade de intervenção em alguns aspectos, modificação de atitudes para enfrentamento mais adequado da doença, como também a melhoria da eficácia da educação em diabetes.
Palavras-chave: Diabetes Mellitus Tipo 1; Educação em Saúde; Enfermagem; Criança; Cuidadores.
RESUMEN
Objetivo: Analizar la eficacia de la educación para la salud en el tratamiento de diabetes mellitus tipo 1 proporcionado por los cuidadores de niños.
Métodos: Se trata de un estudio descriptivo con corte transversal y un enfoque cuantitativo. Utilizamos los instrumentos: Examen de Conocimiento Diabetes Mellitus y escala de autoeficacia en Gestión de la Diabetes, adaptado y validado en Brasil.
Resultados: En relación con el conocimiento de los cuidadores, el 72% tenía una puntuación satisfactoria. La mayoría consigue realizar el tratamiento (80 %) y el 24% no confía en su habilidad; 72% de los encuestados pueden reconocer la hiperglucemia y el 96%, la hipoglucemia; 80% aplica la técnica correcta de la administración de insulina; 80% logran mantener la dieta recomendada, sin embargo, el 16% dijo que no sabía reemplazarla correctamente.
Conclusión: La mayoría de los cuidadores de niños con diabetes mellitus tipo 1 tiene buen conocimiento sobre la enfermedad, y la gestión de la enfermedad realizada por estos cuidadores es satisfactoria en general, sin embargo, hay una necesidad de intervenir de alguna manera, cambiar actitudes para hacer frente de manera más adecuada a la enfermedad , así como también la mejora de la eficacia de la educación en diabetes.
Palabras clave: Diabetes Mellitus Tipo 1; Educación en Salud; Niño; Enfermería; Cuidadores.
Introduction
Diabetes Mellitus (DM) type 1 is a chronic metabolism disorder, characterized by a partial or complete deficiency of the hormone insulin production, resulting from the destruction of pancreatic beta cells, usually caused by the autoimmune or idiopathic process. It can occur in a quick and progressive way in children and adolescents(1-4).
Currently, the DM is considered a global epidemic, being a big challenge for health systems worldwide(1,2,5). However, it affects more than 90% of children and adolescents, it is the second most common chronic childhood disease, with a life expectancy on average of 15 years old(1-4).
The proper management of the disease in children and adolescents has been a challenge, because of the presence of behaviors, skills and inadequate knowledge that contribute to non-adherence to treatment and the significant increase in long-term complications(3-4,6-7).
In this regard, the Pediatric Hospital, reference in pediatric endocrinology in the Unified Health System (SUS), has created a multidisciplinary program of monitoring the family and children with type 1 DM in the ambulatory care unit called Assistance Program Bearer Patient Diabetes Type 1, linked to the Endocrinology and Metabolism Unit, composed of endocrinologists, a nurse, nutritionist, a psychologist, a social worker and a resident endocrinology and nursing and nutrition multi"professional residence.
Before or after the medical consultation, in first or subsequent consultations, health education activity performed by nurses addresses issues related to medicine, monitoring of blood glucose, the resolution of acute complications and monitoring of chronic complications as well as the assessment of knowledge and skills of the caregivers in the management of blood sugar monitoring and insulin application. Thus, education through a multidisciplinary team is a key element for the successful implementation of this complex treatment(3-4,6-10).
The treatment of diabetes is predominantly behavioral, being the key to self" management. However, there is a big gap between knowing what to do and how the individual evaluates his ability to achieve an appropriate behavior. However, there are many variables that influence adherence to treatment, such as age, disease control, knowledge and skills, cost, social support, quality of life, communication between patient and staff, and self-efficacy(11).
Therefore, it is necessary to know these variables to prepare the planning of care and family monitoring of children with type 1 DM and to evaluate their Results(12).
In this context, this study aimed to analyze the health education effectiveness in the management of Type 1 Diabetes Mellitus performed by children's caregivers.
Material and Method
The study is delineated field as descriptive with the cross-cut and quantitative approach, performed in an outpatient clinic of a State Pediatric Hospital of Rio Grande do Norte, Brazil, from June to August 2013. Of the 151 participants eligible for the study, through the number of children and adolescents enrolled in the child care program with diabetes mellitus, 95 were excluded not meeting the inclusion criteria. The total participants included in the study were 56 patients with type 1 DM, of which 36 had appointments scheduled in 2013; and of them, 25 attended the consultations in the study period.
The following eligibility criteria for the study were adopted: children diagnosed with diabetes mellitus type 1, using insulin and aged 0 to 9 years and 11 months old, classified in this range as Children(13) and caregivers of these children enrolled in the children and adolescents patients with DM type 1 program of the Hospital, who had performed at least one nursing consultation, and agreed to participate in the study by signing the Informed Consent Form (TCLE), according to Resolution 466/12(14). Caregivers of children diagnosed with type 2 diabetes mellitus were excluded.
Having the list of children and having sought, information regarding the date and time of appointment in the consultation service system, the researcher carried out the data collection, which occurred on the day and shift of each appointment. First, the children were identified with their caregiver, then, the reason for the approach was presented and explained, clarifying the objectives and purposes of the study, and then the read and completion of the Informed Consent Form (TCLE) was requested.
At first, a questionnaire with closed questions related to socio-demographic, clinical and characterization of children and caregivers was used as a tool for data collection. In the second phase, two adapted and validated instrument in Brazil were used, for the evaluation of patients with diabetes: the Diabetes Mellitus Knowledge Questionnaire (DKN-A)(16) and Self-efficacy Scale in Diabetes Management (IMDSES)(7). These instruments are used to measure and assess the effects of educational interventions in health education programs(15-16).
For the descriptive analysis, the support of the Statistical Package for Social Sciences (SPSS) version 15.0 for Windows was used to provide an organized, summarized and understandable view. In the descriptive analysis of quantitative variables, there is a mean and standard deviation, while categorical data are presented in tables by absolute and relative frequencies.
For the analysis of the variables of the Diabetes Mellitus Knowledge instrument (DKN-A), the Pearson correlation was used as a way to analyze the behavior between two quantitative variables. Then, the analysis of variance (ANOVA) was used to compare the means of variables related to knowledge (DKN-A instrument) and categorical variables.
As for Self-efficacy Scale in Diabetes Management (IMDSES), the variables were analyzed for differences between the responses and the association Pearson Chi-square test was used. Throughout the analysis, a standard p-value of 0.05 and confidence interval (CI) of 95% was considered.
The research started after approval by the Ethics Committee on Research of the UFRN under Certificate Presentation Ethics (CAAE) No 16151013.6.0000.5292 and authorization of the Research Committee of the institution, location of data collection, followed by the legal requirements of Resolution No 466/2012 of the National Health Council which deals with research involving human beings.
Results
Characterization of children with type 1 diabetes and their caregivers
For the characterization of the 25 children with Type 1 Diabetes Mellitus and their caregivers investigated, aspects related to their socio-demographic data, and clinical data of children accompanied by Assistance Program Diabetes Patient Carrier Type 1 were described.
Regarding the children's characterization, the average age was approximately 7.4 (±2.1) years old, with 76% of children in the age group of 6 to 10 years old. The average onset age was 3 and a half years old (±2.0) with a female predominance (60%). Most of them were brown race/skin color (52%), up to 4 years of study (92%); and from the state of Rio Grande do Norte (RN) (56%).
As for the characterization of caregivers of children with type 1 DM, the average age was 35 years old (±7.64), with 44% (n = 11) in the age group of 30 to 39 years old and predominantly female (96%). Most of the caregivers were married/common-law marriage (68%), between 5 to 9 years of education (54%) and 33% had 12 years of study. Caregivers were from the interior of Rio Grande do Norte state (60%), unemployed (71%), but some of them had some occupation (29%) as self-employed, day laborer, a farm worker in agriculture and dressmaker.
The caregivers' knowledge of children with diabetes mellitus type 1
The scores obtained in the knowledge of caregivers, and general understanding of the disease are shown in Table 1, with the application of the Knowledge Questionnaire (DKN-A). Thus, 72% of participants had higher scores than eight, considered as a high score.
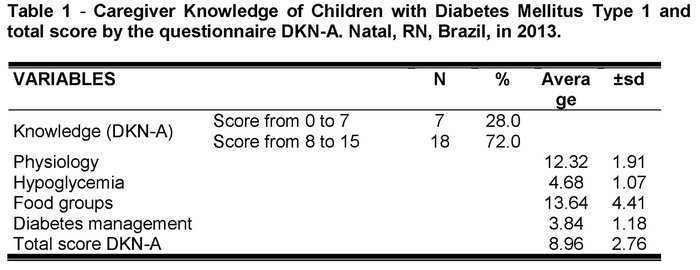
Three correlations were performed with the total score of the DKN-A questionnaire (knowledge). The first correlation was the age of the children, showing a positive correlation, moderate (r=0.44) and significant (p=0.02). The second correlation was between the years of study of the caregiver showing a positive correlation and regular (r=0.32) but not significant (p=0.11), and the third correlation was between disease duration and total score DKN-A, with positive and moderate correlation (r=0.43), and statistical significance (p=0.03).
Analyzing the dimensions of knowledge in the DKN-A, according to the occurrence of hypoglycemia, hyperglycemia and the total score of the questionnaire, there were no significant differences in average (p>0.17, 0.40 and 0.59, respectively).
The effectiveness in the management of type 1 DM performed by caregivers of children with this disease
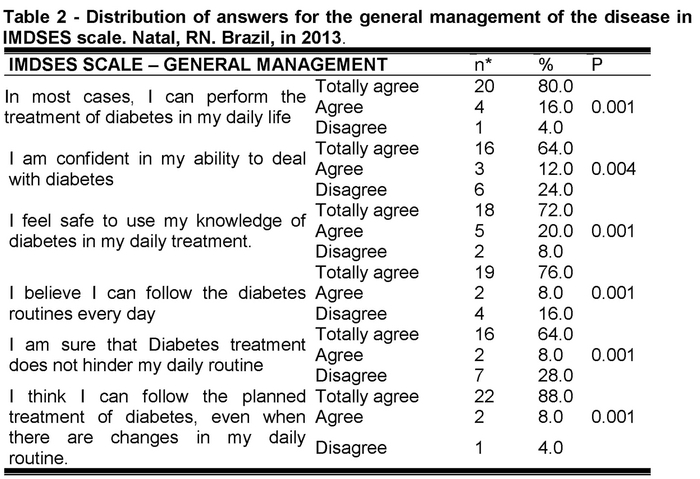
Table 2 shows the distribution of responses for the general management of the disease, considering valid cases.
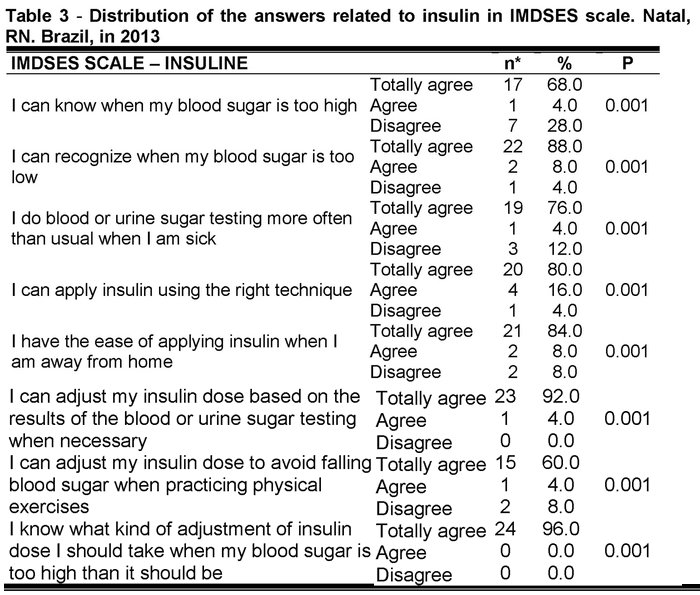
As for the aspect of insulin in the IMDSES scale, Table 3 shows the distribution of responses for the management of insulin. It means that most caregivers trust on their ability to perform the treatment of insulin in the child.
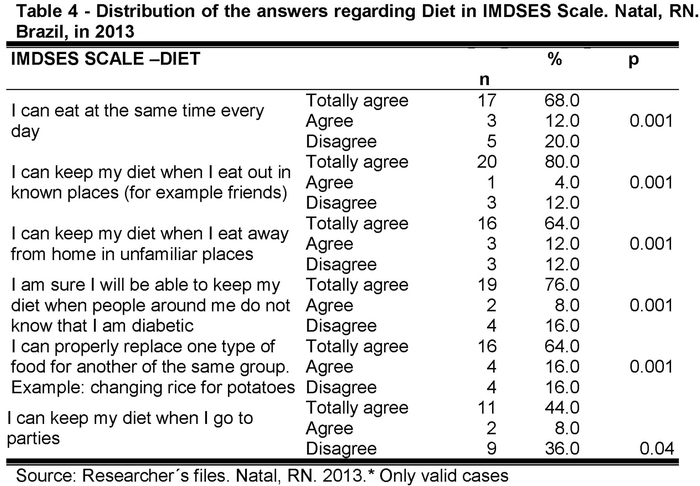
Regarding the replacement of one type of food for another of the same group, 16% said they did not know to replace them correctly; 16% found difficulties in replacing some food and the majority (64%) ensured that could perform the correct replacement (Table 4).
Discussion
Characterization of children with type 1 diabetes and their caregivers
The life of children with chronic disease, especially children with diabetes, has associated stressors related to having diabetes, care for the disease, food control, the explanation of the disease to people who are not from the family, overprotection of friends and family, the concern of the caregiver when the child is away from home and the lack of adequate knowledge about the disease by the child(6).
Analyzing the characteristics of the children with type 1 DM, it was observed that the most of them were on the school stage. The disease has appeared abruptly in early childhood, with solid symptoms indicating the presence of the disease(2,4).
Regarding caregivers of children with type 1 diabetes, it was found that the vast majority were adults, with a good level of cognitive understanding(17). Education interferes significantly in adherence to treatment of DM, as they may have difficulty to understand treatment recommendations and can interfere with adherence to treatment of caregivers too(18). However, this study revealed adherence of caregivers to treatment by the responses and comments, the commitment and the understanding of the importance of treatment and the severity of the disease.
Children show a dependency relationship with their caregivers for the treatment and follow-up of type 1 DM, especially in the age group of the study (under ten years old). Thus, it is necessary to have a right responsible(6,19), justified by the fact that caregivers mostly do not work.
Some mothers reported difficulties in finding support from other family members, especially the father. This is highlighted in studies when children reveal in their statements, an absent father or, in most cases, performing the improper management of the disease as a way to reward their absence in care(6).
It was also noted that grandmothers, aunts, and brothers were cited in research as collaborators in the treatment. In the extended family analysis, some it was identified in some testimonies of children that family members had behaviors that interfered with the good management of the disease, especially the grandmothers, who bought foods not allowed for the children. There are reports in the literature that this attitude may indicate a lack of knowledge about the disease and non-adherence to treatment(6).
Even with caregivers performing the treatment and monitoring the evolution of the disease, it was observed that hyperglycemia episodes happen more often in the sample studied. Prevention of these changes should be carried out through daily monitoring of blood glucose levels, which is essential in the management of type 1 DM, for the children, depending on age, varying in their feeding pattern that hinder the proper adjustment of dose and insulin scheme(2,4).
The caregivers' knowledge of children with diabetes mellitus type 1
Analyzing the scores obtained in knowledge, it was found that most respondents showed satisfactory Results in the knowledge of the DM type 1. This study identified a positive correlation between the longer disease duration (mean of 4 years) and highest children's age, with the greatest knowledge of the disease by caregivers. These data corroborate another study(15), by demonstrating that they may be related to the greater number of consultations and guidance received.
Since the DKN-A is used to measure and assess the effects of educational interventions in education programs in diabetes, it was observed in the total score that the education program has a satisfactory effect. Therefore, it is noteworthy the relevance of the multi-monitoring program for children with chronic diseases.
Although the participants have a good score for knowledge of diabetes, there are still some attitudes needed to change for proper treatment of the disease. It reinforces the continued need for evaluation of diabetes education programs for educational strategies to be redirected, improving learning and encouraging a positive attitude in fighting the disease(6,20).
These recommendations should be strengthened in Hypoglycemia dimensions and Diabetes Management, as shown by the Results of the DKN-A questionnaire in which caregivers showed poor Results in knowledge, adherence, and performance(6). If there is a failure of knowledge, therefore there are practical consequences in the treatment and management of the disease.
Education to the diabetic patient is a critical element in the care of all patients and requires a multidisciplinary team involved, as a fundamental part of the educational process(6,21). This result allows us to identify the need to be strengthened and even modified in educational strategies to provide the foundation for self-management of the disease.
From the knowledge dimensions of the DKN-A according to the occurrence of hypoglycemia, hyperglycemia, and the total score of the questionnaire, it was observed that the occurrence of complications is not related to having or not knowledge but a great adherence and participation of the diabetic patient and the entire family(2,22).
Above all, besides the educational process, the treatment has the regular physical activity, dietary guidelines and the full replacement of insulin(6). Thus, diabetes education is considered very important for the management of the disease, which for years it was seen as a way to transmit knowledge, teaching skills for self-care and requirement of the therapeutic recommendations. However, this passive process and centered on the educator has been considered inadequate for the practice of diabetic patient education. Thus, an education not only is recommended for self-care but also to change behavior(9-11).
The effectiveness in the management of type 1 DM performed by caregivers of children with the disease
Analyzing the General Management of the disease from the Results of IMDSES scale, it was observed that caregivers could lead the management of the treatment, although some of them showed that these factors need to improve so that confidence in their ability to make decisions on the plan of self-care control is more effective.
As the more effective treatments are scientifically proven and as the more effective as behavioral interventions, it is necessary to place the incorporation properly in the patient's life. For these reasons, the biggest challenge for health professionals regarding people with diabetes is to teach them how to live and manage the disease. Thus, educating for behavioral changes occurred and sustained over the course of the disease and life(3,23).
It is observed that there are many difficulties in education for the effective behavior change, in which the skills and knowledge are insufficient. It is essential to know how a diabetic person perceives his situation, what his attitudes are and for what extent he believes it can influence the course of the disease(3).
An important aspect shown by this study is related to diabetes routines and their influence in the child's life, showing the change in the family routine is inevitable and radical. Diabetes mellitus type 1 entails individual implications that relate to acceptance of the disease and treatment, which make the difference in the context of the life of these individuals and interfering with their quality of life and survival(19).
This study found that the physical exercise is not considered as part of the treatment of children with type 1 DM. Caregivers reported that the children were playing, and the majority did not perform a specific physical activity, either by family and financial conditions/or because the school did not offer this activity.
The daily monitoring of blood glucose levels is an essential aspect in the management of type 1 DM(1). The literature emphasized lower adherence and a certain difficulty of diabetics to incorporate this important tool for achieving metabolic control, as it allows the identification of episodes of hypoglycemia, hyperglycemia control, adjust the medication and preventing complications(17).
Furthermore, it is also important in pediatric patients, to monitor the incidence of hypoglycemia. Depending on the age, the child, may vary in their feeding pattern which makes the proper adjustment of the dose and insulin regimen. Therefore, it should be noted the importance of persisting in glycemic control, so they do not have early complications of type 1 DM, such as micro-angiopathy(4).
A problematic aspect observed in this study is the insulin administration technique. Although the vast majority knew performing step by step properly, the concern should be with the failures and those who did not use the technique correctly. Therefore, it is necessary to strengthen the guidance and the continuous repetition. Some aspects should be considered, such as the preparation of insulin (combined or not), the graduation of the syringe doses, ways of administration, local and application technique, the rotation of places; insulin storage and disposal of the material used(4,10,23).
Analyzing the diet from the Results of IMDSES scale, it was observed that their maintenance and compliance with mealtimes were held by the majority of the children interviewed. The food monitoring, as well as the management of food changes, are an essential part of the treatment of diabetes(15). In this context, there is the participation of the nutritionist in diabetes education because it is up to him further deepening this issue(17).
Therefore, considering the criteria for evaluating the effectiveness of the education program: Regular physical activity practice; Change in eating habits; Good psychosocial adaptation; Adherence to the dosage of the medication regimen; Adequate self-monitoring of blood glucose; Reduction of the risk of chronic complications (improvement in glycemic control); Individual's ability to properly correct hypoglycemia and hyperglycemia(9) and the Results of this study, it was observed that the education program in diabetes has good efficacy. However, it is necessary to consider and strengthen some important aspects of the management of diabetes to be adequate and provide a better quality of life of affected children.
Conclusion
It is understood that the caregivers have adequate knowledge about the disease and the factors surrounding it, such as treatment and diet. However, they demonstrated the need to strengthen some aspects such as control of hypoglycemia, the type 1 DM management and better development of the criteria considered important in assessing a diabetes program, especially ability to properly correct the hypoglycemia and hyperglycemia, adherence the regimen of medication and regular physical activity, improving the effectiveness of diabetes education, as well as answering to the health needs of this population, providing quality of life for children with diabetes and their families.
Received: April 10
Accepted: June 24, 2015
References
1. World Health Organization. What are the risks of diabetes in children?. 2012. [ Links ]
2. Hockenberry MJ, Wilson D. Wong-Fundamentos de Enfermagem Pediátrica. 8 ed. Rio de Janeiro: Elsevier; 2011. [ Links ]
3. Sociedade Brasileira de Diabetes (SBD). Diretrizes da Sociedade Brasileira deDiabetes: 2013-2014. São Paulo: AC Farmacêutica; 2014. [ Links ]
4. Sociedade Brasileira de Diabetes. Diretrizes da Sociedade Brasileira de Diabetes. AC Farmacêutica. 3 ed. 2009a. p. 400. [ Links ]
5. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Cadernos de Atenção Básica, n. 16. Diabetes Mellitus. Brasília (DF): Ministério da Saúde; 2006. p. 64. [ Links ]
6. Nascimento L C, Amaral M J, Sparapani V C, Fonseca L M M, Nunes M D R, Dupas G. Diabetes mellitus tipo 1: evidências da literatura para seu manejo adequado, na perspectiva de crianças. Rev Esc Enferm USP. 2011;45(3):764-9. [ Links ]
7. Brito TB, Sadala MLA. Diabetes mellitus juvenil: a experiência de familiares de adolescentes e pré-adolescentes. Ciênc Saúde Coletiva. 2009;14(3):947-60. [ Links ]
8. Associação Americana de Educadores em Diabetes-AADE. AADE Position Statement: Individualization of Diabetes Self-management Education. In: The Diabetes Educator. 2007; 33:45. [ Links ]
9. Leite SAO, Zanim LM, Granzotto PCD, Heupa S, Lamounier RN. Pontos básicos de um programa de educação ao paciente com diabetes melito tipo 1. Arq Bras Endocrinol Metab. 2008;52 (2):233-42. [ Links ]
10. Torres HC, Pereira FRL, Alexandre LR. Avaliação das ações educativas na promoção do autogerenciamento dos cuidados em diabetes mellitus tipo 2. Rev Esc Enferm USP. 2011; 45 (5):1077-82. [ Links ]
11. Marshall M, Carter B, Rose K, Brotherton A. Living with diabetes: perceptions of children and their parents. J Clin Nurs. 2009;18(12):1703-10. [ Links ]
12. International Diabetes Federation/ International Society for Pediatric and Adolescent Diabetes (IDF/ISPAD). Global Guideline for Diabetes in Childhood and Adolescence. 2011. [ Links ]
13. Ministério da Saúde (BR). Coordenação Nacional de hipertensão e diabetes. Hipertensão arterial e diabetes mellitus: morbidade auto referida segundo o VIGTEL, 2009 e cadastro de portadores do SIS-Hiperdia 2010. Brasília (DF): Ministério da Saúde; 2011. [ Links ]
14. Ministério da Saúde (BR). Comissão Nacional de Ética em Pesquisa. Normas para pesquisa envolvendo seres humanos (Res. CNS 466/2012 e outras). Brasília (DF): Ministério da saúde; 2012. [ Links ]
15. Oliveira KCS, Zanetti ML. Conhecimento e atitude de usuários com diabetes mellitus em um serviço de atenção básica à saúde. Rev Esc Enferm USP. 2011;45(4):862-8. [ Links ]
16. Torres HC, Hortale VA, Schall VT.Validação dos questionários de conhecimento (DKN-A) e atitude (ATT-19) de Diabetes Mellitus. Rev Saúde Pública. 2005; 39(6): 906-11. [ Links ]
17. Pélicand J, Gagnayre R, Sandrin-Berthon B, Aujoulat I. A therapeutic education programme for diabetic children: recreational, creative methods, and use of puppets. Patient Educ Couns. 2006; 60(2):152-63. [ Links ]
18. Villas-boas LCG, Foss MC, Foss-Freitas MC, Torres HC, Monteiro LZ, Pace AE. Adesão à dieta e ao exercício físico das pessoas com diabetes mellitus. Texto Contexto Enferm. 2011; 20(2): 272-9. [ Links ]
19. Sales CA, Tironi NM, Artibale D, Ferreira E, Silva MAP, Violin MR, et al. Cuidar de uma criança com diabetes mellitus tipo 1: concepções dos cuidadores informais. Rev Eletr Enf (Internet). 2009 (citado 2012 out 20);11(3):563-72. Disponível em: http://www.fen.ufg.br/fen_revista/v11/n3/pdf/v11n3a13.pdf. [ Links ]
20. Rodrigues FFL, Zanetti ML, Santos MA, Martins TA, Sousa VD, Teixeira CRS. Conhecimento e atitudes: componentes para a educação em diabetes. Rev Latino-am Enfermagem. 2009;17(4):468-73. [ Links ]
21. Pennafort VPS, Silva ANS, Queiroz MVO. Percepções de enfermeiras acerca da prática educativa no cuidado hospitalar a crianças com diabetes. Rev Gaúcha Enferm. 2014; 35(3):130-6. [ Links ]
22. Almeida J. Paulo, Pereira M. Graça, Fontoura M. Variáveis individuais e familiares na adesão ao tratamento, controle metabólico e qualidade de vida em adolescentes com diabetes tipo 1. Rev SBPH. 2012; 15(1): 59-82. [ Links ]
23. International Society for Pediatric and Adolescent Diabetes (IS PAD). Clinical Practice Consensus Guidelines 2006-2007. Swift PGF. Diabetes education. Pediatr Diabetes. 2007; 8:103-9. [ Links ]

