










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.16 no.47 Murcia jul. 2017 Epub 01-Jul-2017
https://dx.doi.org/10.6018/eglobal.16.3.259541
Originales
Engagement and commitment in nurses: associated sociodemographic and labour variables
1Diplomada in Nursing. Master in Gerontology. Zaragoza's University. Spain.
2Licenciada in Social and Cultural Anthropology. PhD in Sociology. Zaragoza's University. Spain.
3Licenciada in History of Art. PhD in Sociology. University of Zaragoza. Spain.
Objectives
To determine the level of engagement and its relation with six areas of work life in nursing professionals in the city of Huesca, Spain and its association with socio-demographic and labour variables.
Materials and Methods
A descriptive, cross-sectional study with a quantitative approach, which involved 305 nurses. Descriptive analysis, bivariate correlations and parametric tests, ANOVA and T-Student.
Results
Most participants were women, with children and a partner, with a mean age of 44.98 years (SD 10.86). 35.4% of the sample had high levels of engagement (high levels of energy, involvement and effectiveness). Civil status, employment status of the partner and chronic diseases were related to levels of effectiveness; leisure activities were related to energy levels and involvement. The assessment of the labour climate is related to allthree areas of engagement; age, time in the work unit, years working as a nurse and time in a management position are related to involvement.
Conclusions
The study population has high levels of work engagement and consistency between the subscales of working life and the organization, with the exception of the subscale of fairness, since individuals surveyed believe that the organization treats them unfairly.
Keywords Nurses Clinics; Nursing staff; Nursing; Occupational Health; Job Satisfaction
INTRODUCTION
Nursing has developed over the years in parallel with the evolution of care in society, and because nursing has developed along side the evolution of care in society, its profesional development has met with many obstacles. It was not until the emergence of Florence Nightingale in 1859 1 that nursing emerged as a profession, and the basis of formal trainingwas established in this field.
Hildergard Peplau, Callista Roy, Martha Rogers, Virginia Henderson and Dorothea Orem 1 among others have since developed theories and models that delimit the conceptual framework of nursing, agreeing to establish that the essential characteristicof nursing is "care", defined by Vera Regina Waldow as "the phenomenon resulting from the caring process, which in turn represents the way in which, or should occur, the encounter between the being who cares and the being that is cared for". This same author states that "care is relational, that is, it is always in function of the other (be a thing, object, animal, any living being). In nursing, the other is the patient and his family, those who need his care" 2.
The characteristics of nursing, such as its complex development as a profession 3, since it was based on the assumption that nursing is an innate art to any woman and not a particular profession4, the fact that care is a relational act 2 and the continuous contact with people/clients, promote the experience of burnout syndrome inthis profession. This syndrome was defined in 1961 by Grahan Greene in a novel entitled "A burnout case", and later in 1974 was defined by the American psychologist Herbert Freudenberger 4)(5. A few years later, Maslach and Jackson 6 defined this syndrome as: "A syndrome of emotional exhaustion and cynicism that often occurs in individuals who work for people, and who devote a lot of time to personal relationships of a confidential nature with those people under chronic conditions of stress and tension."
In contrast, the term of engagement emerges, defined by Leiter and Maslach in 1998, as "an energetic state of involvement with the activities with which they personally ful fill and improve the sense of professional efficiency" 7. These authors define engagement as an opposite concept to burnout, where energy becomes exhaustion, involvement turns to cynicism and efficacy to inefficacy 8. The psychological relationships of people with their jobs have been conceptualized as a continuum betweenthe negative experience of burnout andthe positive experience of engagement. In 2002, Scaufeli et al. 9 argue that the concept of engagement is a concept with its own entity, not just the opposite form of burnout. These authors findthat the concept of engagement is the antithesis of burnout 8.
Engaged employees are individuals who take personal initiative in their work and generate their own feedback on performance 10, look for new challenges and are committed to achieving excellence in their performance, which leads them to develop positive feedback with their supervisors and customers. These employees also experience fatigue but associate it with something positive such as accomplishment of a job well done and achievement of a goal 11).
Given the increasing interest that this term presents for the business world, several evaluation questionnaires have been developed, not all publicly available, as companies do not want to share this data with their competitors. Among these questionnaires are the Gallup Q12 12, Personal Engagement questionnaire developed by May et al. 13, the UWHE developed by Schaufeli et al. 14, and the Six Areas of Work Questionnaire (AWS) developed by Michael P. Leiter and Christina Maslach in 2004 15, and validated in Spanish by Gascón and Leiter 16.
To obtain professionals with a high level of "engagement" is the objective of labour organizations, to know what are the personal, socio-demographic and labour variables that are associated with it allows to develop strategies that promote their development among professionals and avoid all those that promote the development of burnout syndrome 17)(18. Therefore, the objective of this study is to know the engagement situation in health professionals of health centres in a northeastern area of Spain, as well as the personal variables, socio-demographic and labour conditions associated with it.
METHOD
A cross-sectional descriptive study was carried out amongnurses who work in health centres in Huesca, Spain. Huesca is a city in the northeast of the Iberian peninsula with 52,418 inhabitants in 2013 according to the National Institute of Statistics 19. It is the capital of the province of the same name, which forms, together with the provinces of Zaragoza and Teruel, the Autonomous Community of Aragon, and in turn falls within one of the health sectors that make up the Aragonese Health Service, the Health Sector of Huesca, which serves a population of 107,197 inhabitants according to the health map of the Autonomous Community of Aragon 20. The survey was conducted in all public and private health centres in the city that had nurses ontheir staff, except a private clinic that declinedto participate. In the present study, all public health centres of the city participated, including hospital centres, geriatric residences, primary care centres and specialized care centres. Private centres that participated in the study are geriatric centres, mutual labour, specialized medical centres and specialized care centres. Overall, 20 public and private health centres participated in this study. 92.1% of the respondents performed their care practice in centres with a capacity of 500 beds or less, this type of health centre being representative of 90% of Spanish hospitals according to the National Catalogue of Hospitals of 2015 carried out by the Ministry of Health, Social Services and Equality 21.
Two types of instruments were used for the collection of information. Firstly, an instrument of our own elaboration that collected socio-demographic variables and labour variables. This questionnaire also included an assessment of the working environment using a Likert scale (0 very poor / 5 excellent). The second tool used was aquestionnaire developed by Michael P. Leiter and Christina Maslach in 2004, validated in Spanish by Gascón and Leiter (16), which comprises 45 items divided into two questionnaires. The first one consists of 16 items that are scored according to a Likert scale that includes values from 0 (never) to 6 (daily), and evaluates three states opposed to burnout syndrome, energy (as opposed to emotional exhaustion) is evaluated through 5 items, efficacy (contrary to depersonalization or inefficiency) is evaluated by 6 items and involvement (opposite to cynicism) is evaluated by 5 items. This scale in turn allows to evaluatethe three dimensions that make up the burnout syndrome (professional efficacy, cynicism and exhaustion).
The second questionnaire consists of 29 items that evaluate the congruence or incongruity of the individual toeach of Six Areas of Work Life (risk factors shown as apositive) using a Likert scale that ranges from 1 (strongly disagree) to 5 (strongly agree), it has 6 subscales: workload or overload (6 items), control (3 items), reward (4 items), community (5 items), fairness (6 items) and values (5 items). The alpha coefficient of the scales meets the criterion of 0.70, with the highest value in Control with 0.832, and the lowest in Community with 0.757, which guarantees the reliability of the subscales.
Data analysis was performed using the statistical package SPSS Statistics V17.0. A descriptive and analytical statistical study was performed, with a significance level chosen ofp <0.05.
A descriptive analysis ofthe sample as well as bivariate parametric correlations and tests, ANOVA and T-test were carried out, in order to analyse how socio-demographic and labour factors affect engagement prevalence and its relation with Six Areas of Work Life in the study population.
RESULTS
The actual reference population was 527 nursing professionals and a response rate of 57.87% was obtained. 91.1% of the respondents were women, 83.3% had a partner and 67.9% had children. The mean number of children was 1.23 children (SD= 0.990) and the average age of the respondents was 44.98 years (SD = 10.86). 92.1% of the respondents performed their care in health centres with a capacity ranging from 200-500 beds or less.
Table 1 shows the mean and standard deviations of the different subscales, where it is observed that in five of the six areas of work the individuals present a satisfactory congruence with the organization (Maslach and Leiter, 2008): workload, control, reward, community and values. Only the fairness sub-scale presents inconsistency between the individuals surveyed and the organization.
Table 1 Mean and Standard Deviation of sub-scales
| VARIABLE | MEAN | SD |
|---|---|---|
| Energy | 4.52 | 0.92 |
| Involvement | 4.89 | 0.96 |
| Efficacy | 4.08 | 1.00 |
| Workload | 3.37 | 0.73 |
| Control | 3.08 | 0.85 |
| Reward | 3.30 | 0.69 |
| Community | 3.61 | 0.63 |
| Fairness | 2.62 | 0.73 |
| Values | 3.09 | 0.70 |
If we analyse the results obtained according to a percentiles division (as done by Maslachand Jackson (1986) with the MBI-GS scale) that divides them into low, medium and high levels, we observe that 79.5% reported high scores in the energy sub-scale, 56.3% scored high on the efficacy sub-scale and 85.3% scored high on the involvementsub-scale.
Engagement, understood as a syndrome composed of high energy, involvementand efficacy, appears in 35.4% of the sample studied. Of those individuals with engagement,86.1%have a partner, and for 76.5%their partner is active. 67.2% of those with engagement have children while72.4% do not have dependents. 75% are non-smokers, 92.6% do not drink alcohol on a regular basis, 68.5% do regular exercise and 81.5% do leisure activities, 61.1% do not have post-graduate training and 58.5% have a permanent contract. In addition, 1.9% hold a management position and 12% a supervisory position.
Table 2 shows the significant relationships between the sub-scales of engagement and the six areas of work life with the socio-demographic variables, with the efficiency sub-scale being the one with the most significant relationships (civil status, situation and the variable of chronic diseases), compared to energy and involvement that only present significant relationships with the performance of leisure activities. In addition to this, according to Bonferroni’s Post Hoc there is a significant relationship between those whose partneris unemployed and those who do not have a partner(p <0.05).
Table 2 Significant relationships between engagement sub-scales and the sub-scales of the six areas of work life with socio-demographic and labour variables (T-test)
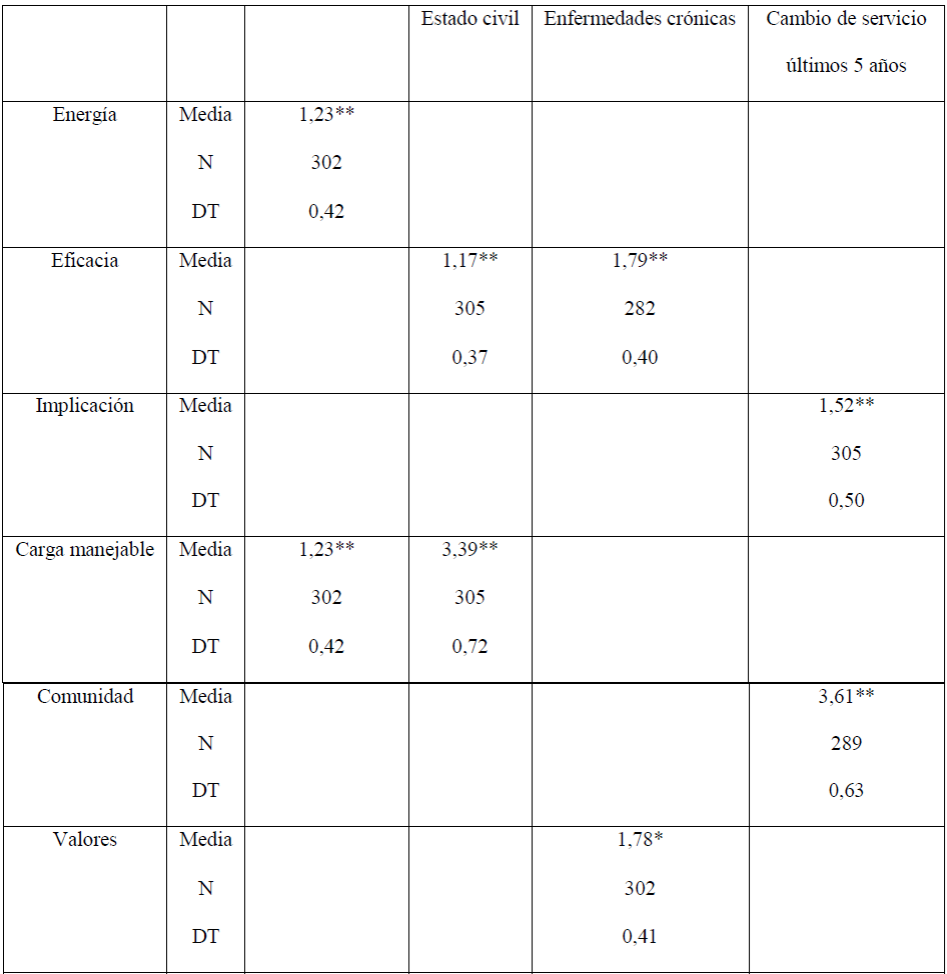
* p<0.05 **p<0.01
The scores on the reward sub-scale also show significant relationships with the partner’semployment situation according to the Bonferroni Post Hoc, with a significant relationship between those whose partneris active and those whosepartneris unemployed (p <0.05). The scores obtained in the community sub-scale show, according to Bonferroni Post Hoc, that there are significant relationships between those whose partnerisunemployed and with those whose partneris active (p <0.05) and those who do not have a partner(p<0.05).
If the obtained scores are established in relation to the average obtained in the sample, it is observed that they present a greater efficiency than the average of those who have a partner (p <0.05) and those whose partneris in active employment (p < 0.01). On the other hand, those who perform leisure activities usually have high energy (p <0.01).
The significant relationships between engagement sub-scales and labour variables are shown in Table 3, where it can be seen that the labour climate valuation variable is significantly related to all sub-scales of engagement, whereas the sub-scale of involvement is related to a greater number of labour variables (type of contract, time in a management position, time in the work unit, years as a nurse and change of service in the last five years). Regarding the relationship between involvementand type of contract, after Bonferroni Post Hoc, it is observed that there is a significant relationship between those who have a fixed contract and a replacement contract (p <0.05).
Table 3 Correlations between engagement sub-scales and socio-demographic and labour variables
| Age | How do you rate the work climate | Time in the work unit in years | Years in a management position | Years as a nurse | |
|---|---|---|---|---|---|
| ENERGY | .309** | ||||
| EFFICACY | .218** | ||||
| INVOLVEMENT | -.142* | .305** | -.154* | .995** | -.144* |
* p<0.05 **p<0.01
If the obtained scores are established in relation to the mean obtained in the sample, it can be observed that the majority of those working in management positions (p <0.05) have a high involvement, and these also have high efficacy (p<0.01).
The significant relationships established between the subsectors of the Six Areas of Work Life and the socio-demographic variables can be seen in Table 2. In addition, we can see the workload subscale has a greater number of significant relationships, and that the control and fairness subscales do not present significant relationships with any of the socio-demographic variables analysed.
As expected, labour variables present a greater number of significant relationships with the sub-scales of the six areas of work life, as can be seen in Table 4. In addition to the relationships observed in the table, those that are established between the variables of "Holds a management position" with the control sub-scale (p <0.01), with the fairness sub-scale (p <0.01) and with the values sub-scale (p <0.05). Also, exercising a management position is significantly related to the control sub-scale (p <0.01).
Table 4 Correlations between the sub-scales of the Six Areas of Work Life and labour variables
| How do you rate the work climate | Years as a nurse | Years in a management position | Time in the work unit in years | |
|---|---|---|---|---|
| Workload | .193** | .131* | .127* | |
| Control | .241** | |||
| Reward | .322** | |||
| Community | .418** | |||
| Fairness | .189** | -.125* | .952* | |
| Values | .248** | -.161** | .821* |
* p<0.05 **p<0.01
According to the Bonferroni Post Hoc analysis in the relationship between the manageable workloadand the work centre, significant relationships are established between those belonging to health centres with those of emergency centres (p <0.05). In the relationship between the control sub-scale and the work shift, significant relationships are established between those in rotating shifts with those who work day shifts (p <0.05), and those who work rotating shifts with those who work inshifts categorizedas "Others" (p<0.05); in the relationship between the fairness sub-scale and age measured in intervals (p <0.01), significant relationships are established between those found in the age group 24-34 years old with those between 35-44 years old (p <0.01) and those aged 45-54 years (p <0.05); between the values sub-scale and the work shift (p <0.05), significant relationships are established between those who work according to a rotating shift and those who follow a day shift (p <0.05), and the age measured in intervals (p <0.01) establishing significant relationships between those belonging to the age group 24-34 years with those of the rest of the groups (p <0.05 for the group of 35-45 years and p <0.01 for the rest of the groups); between the community sub-scale and the time spent working on the unit measured in intervals (p <0.01), significant relationships are established between those who have been working for more than 5 years and less than 10 years in the same unit with those whohave been in the same unit for more than 20 years (p <0.05).
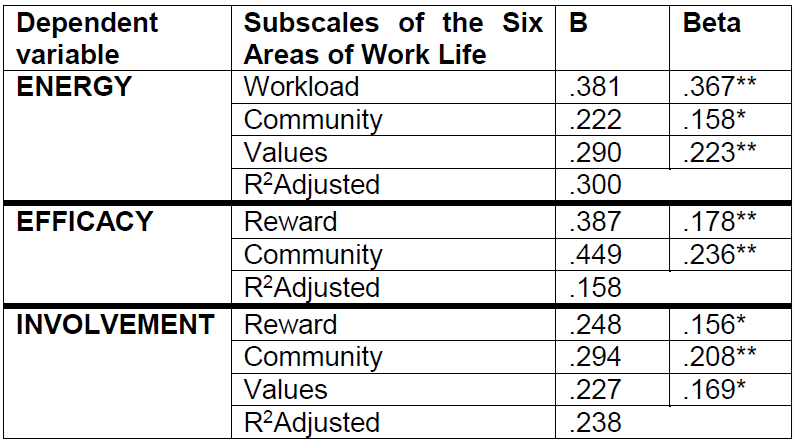
By linear regression analysis we tried to find outwhich variables predicted or contributed to the dimensions of energy, efficiency and involvementas shown in Table 5, establishing that the variables contributing to the energy sub-scale are the workload ( p<0.01), the sense of community (p<0.05) and values (0.01); those contributing to the sub-scale of efficacy or performance inwork are the feelings of reward (p <0.01) and the sense of community (p <0.01), being similar in the group of women,whereas in men only the sense of community contributes (p <0.01);the variables that contribute significantly to the sub-scale of involvement are the feelings of reward (p<0.05), community (p <0.01) and values (p <0.05), and this also applies in the group of women, but not in that of men, in which the feelings of community do not contribute significantly to obtain good levels of involvement.
DISCUSSION
The engagement results obtained by the present study are similar to those obtained by previous studies conducted amongnursing professionals in Italy 22, with the exception of the scores obtained in the energy sub-scale, whose figures are higher in the present sample. Similarly, in astudy carried out in southern Switzerland 23 the scores obtained in the energy sub-scale are lower than those obtained in the sample studied. The difference between the data obtained in the present study and those obtained by other authors may be due to the difference between the mean ages of the population as indicated by Mahboubi 24, or to the fact that the sample of this study is larger. In addition, it should be noted that the presence of higher scores in the energy sub-scale indicates, on the contrary, lower scores on the exhaustion sub-scale, a central dimension of burnout syndrome, indicating that the professionals surveyed have less of a need to distance themselves emotionally from work, a fact that may be due to the size of the centres where the surveys have been carried out with a capacity of less than 500 beds, as well as 90% of Spanish health centres, and the smaller size of health centres isrelated to a lower level of burnout 25.
As for the results obtained in the sub-scales that measure the six areas of work life, it is observed that in the present study only the fairness sub-scale presents incongruence between the individuals and the organization, just as in the study carried out by Fiabane 22, but not in other studies where there is inconsistency between individuals and organization in the scales of manageable workload and fairness23)(26)(27. The fact that the fairness sub-scale always appears as incongruent between individuals and the organization emphasizes that health professionals feel that the organizations they work for treat them unfairly, or not as justly as they would like, sodeveloping models that improve these feelings of fairness would directly improve the engagement of individuals with the organization. Measures aimed at developing this sense of fairnesswould be the implementation of leadership models 28 or goal orientation 29.
As in previous studies 18)(30, it is observed that the age of professionals, physical symptoms or chronic diseases, and civilstatus influence the engagement and burnout syndrome in the present study. Relationships of the sub-scales that make up engagement with the partner’s work situation have not been analysed in the consulted studies, but their association seems logical due to the psychosocial stress that this situation can generate.
Work climate is considered as a predictor of engagement and the six areas of work life according tothe results of the present study, as well as the results obtained in previous studies 17)(18, and this phenomenon also occurs in the opposite sense, since engagement influences the perspective of work climate, results and quality of care 17.
As for the subscales that measure the six areas of work life, it should be noted that although the fairness sub-scale is the only one that generally obtains a score that shows incongruence between the individuals and the organization, this sub-scale presents significant relationships with the variable of time in a management position, which may be related to the fact that in these positions there is greater social recognition, a variable that has been shown to be a predictor of engagement together with job gratitude 29. Likewise, the fact of being in a management position is associated with a high involvement, related to the fact that satisfaction with the work position improves the quality of working life, reduces social dysfunction and stress 31.
The fact of working in the different healthcare units has been studied as a determinant variable forsuffering burnout syndrome, with health emergency services being the ones that obtain the worse scores in the measurement scales for burnout syndrome, that is to say, low scores in engagement 32, contrary to the results obtained in the present study. These results may be due to the small size of this service in this community and consequently tothe lower pressure of care that it supports. The association between different sub-scales of the six areas of work life and work shift has already been described in studies that conclude that nursing management, professional practice, relationships with physicians, organizational resources and shift work influence engagement factors 33.
As previously stated, age of the respondents establishes significant differences in sub-scales that make up engagement and those of the six areas of work life, so that younger professionals present significant differences compared to olderprofessionals. Similar data were obtained in several studies where it is concluded that in newly graduated professionals, modifying labour factors exert an important influence on job satisfaction and the intention to leave work, and consequently on engagement and burnout 34 or in studies which conclude that those students who finish their nursing studies with low levels of engagement have low levels of preparation at the end of their studies 35. Therefore, preventive measures are essential to avoid development of burnout syndrome in nursing students, and consequently in the potential new labour forthis profession.
Subsequently, by analysing by linear regression the contribution of the sub-scales of six areas of work life to feelings of energy, efficacy and involvement, the results are similar to those obtained by several authors previously, so that manageable workload predicts energy 36 as in the present study, that is, that dealing with a manageable (quantitative and / or qualitative) workload makes individuals more efficient in performing tasks 37. The same occursin several studies 22)(23 where manageable workload contributes to good energy levels and to good levels of involvement. In the present study, community and values contribute to feelings of energy, feelings of values are also reflected in previous studies 23, since a good fit between the individual values and those of the organization is associated with energy and involvement 23, while in other studies it would also contribute to good levels of efficacy 22. Feelings of adequate reward for the work done contribute to levels of efficacy and involvement as in previous studies 23 but not to energy levels 22, results that are in line withprevious studies where appropriate reward predicts levels of engagement 29).
Although in the previous literature feelings of control are related to engagement 23)(29, in the present study, and in those of different authors 22)(38, this does not happen, a fact that may be because high feelings of control are not necessarily advantages for the well-being of workers 38.
Results obtained in the present study show high levels of engagement amongthe professionals surveyed, and engagement has been associated with fewer health problems, particularly social dysfunctions 23.
The main limitations of the study are that it has been developed in a specific area of northeastern Spain, so its results maynot be representative of nursing professionals throughout the country, but the fact that the study was carried out in a centre with a capacity lower than 500 beds is representative of 90% of Spanish health centres.
CONCLUSIONS
The studied population presents high levels of labour engagement and congruence between the sub-scales of work life and the organization, with the exception of the fairness sub-scale where there is inconsistency, that is, individuals surveyed do not believe that the organization is treating them fairly. On the other hand, the valuation of the working environment is shown to be the variable that presents more significant relationships with engagement and six areas of the working life, and the sub-scale of involvementis one that presents more significant relations with labour variables, so that implementing strategies that achieve a high level of involvement of individuals will have important repercussions in the workplace.
Contrary to the data obtained by several previous authors,the sample analysed presents a high level of professional engagement, and consequently, will present low levels of burnout, which should be studied in future to know the variables associated with these findings.
Improving and implementing work engagement in nursing professionals reducesthe risk of occupational stress and burnout, and consequently leads toa higher quality of care for users of their services. Knowing the situation of engagement between professionals and the socio-demographic and labour factors with which it relates is fundamental to be able to establish measures that encourage their appearance in order to improve the care offered and achieve a higher level of health of the different professionals reducing work abandonment. Our results show that there are several socio-demographic and labour variables that are associated with the emergence of labour engagement, which could be used to promote a healthy working environment and greater job satisfaction, so the findings of this study could be developed with preventive measures to improvethe well-being of health professionals. Likewise, these results would allow the later development of qualitative studies in order to find out thedeeper realities of these relations.
REFERENCIAS
1. Alligood MR, Merriner Tomey A. Modelos y teorías en enfermería. 7ª ed. Barcelona: Elsevier; 2011. [ Links ]
2. Waldow VR, Borges RF. El proceso de cuidar según la perspectiva de la vulnerabilidad. Rev Latino-am Enfermagem. 2008 julho-agosto; 16(4). [ Links ]
3. Burgos Moreno M, Paravic Klijn T. Enfermería como profesión. Rev Cubana Enfermería [internet]. 2009; 25(1-2) [consultado 23 Mar 2016]. Disponible en: http://bit.ly/11LW4sh [ Links ]
4. Mingote Adán JC. Síndrome de burnout o síndrome de desgaste profesional. Formación Médica Continuada. 1998; 5(8): 493-508. [ Links ]
5. Moreno B, González JL, Garrosa E. Desgaste profesional (burnout), personalidad y salud percibida. En J. Buendía y F. Ramos (Eds.). Empleo, Estrés y Salud. Madrid: Pirámide; 2001. p. 59-83. [ Links ]
6. Maslach C, Jackson SE. Burned-out cops and their families. Psychology Today. 1979; 12 (12): 59-62. [ Links ]
7. Leiter MP, Maslach C. Burnout. En H. Friedman (Ed.). Encyclopedia of Mental Health. San Diego, CA: Academic Press; 1998. P. 347-357. [ Links ]
8. Rodriguez-Muñoz A, Bakker AB. El engagement en el trabajo. En B. Moreno-Jimenez E. Garrosa Hernandez (Eds.). Salud laboral: Riesgos laborales psicosociales y bienestar laboral. Madrid: Pirámide; 2013. p. 437-452. [ Links ]
9. Schaufeli WB, Salanova M, Gonzalez-Roma V, Bakker AB. The measurement of burnout and engagement: A confirmatory factor analytic approach. Journal of Happiness Studies. 2002; 3:71-92. [ Links ]
10. Schaufeli WB, Taris T, Le Blanc P, Peeters M, Bakker AB, De Jonge J. Maakt arbeid gezond? Op weg naar een positieve Arbeids- en Gezondheidspsychologie. De Psycholoog. 2001; 36:422-428. [ Links ]
11. Schaufeli WB, Salanova M. Work engagement. Managing social and ethical issues in organizations. 2007: 135-177. [ Links ]
12. Harter JK, Agrawal S. Cross-cultural analysis of Gallup's Q12 employee engagement instrument. Omaha, NE: Gallup. 2011. [ Links ]
13. May DR, Gilson RL, Harter LM. The psychological conditions of meaningfulness, safety and availability and the engagement of the human spirit at work. Journal of Occupational and Organizational Psychology. 2004; 77: 11-37. [ Links ]
14. Schaufeli WB, Salanova M, González-Romá V, Bakker AB. The measurement of Engagement and burnout: A confirmative analytic approach. Journal of Happiness Studies. 2002; 3: 71-92. [ Links ]
15. Leiter MP, Maslach C. Areas of worklife: A structured approach to organizational predictors of job burnout. En P. L. Perrewe & D. C. Ganster (Eds.). Research in Occupational Stress and Well-Being. Oxford: Elsevier; 2004). P. 91-134. [ Links ]
16. Gascón S, Leiter MP, Srtight N, Santed MA, Montero-Marín J, Andrés E, et al. A factor confirmation and convergent validity of the "areas of worklife scale" (AWS) to Spanish translation. Health and Quality of Life Outcomes. 2013; 11:63. [ Links ]
17. Van Bogaert P, van Heusden D, Timmermans O, Franck E. Nurse work engagement impacts job outcome and nurse-assessed quality of care: model testing with nurse practice environment and nurse work characteristics as predictors. Frontiers in Psychology. 2014; 5. [ Links ]
18. Lee HF, Yen M, Fetzer S, Chien TW. Predictors of Burnout Among Nurses in Taiwan. Community Ment Health J. 2015;51(6):733-7. [ Links ]
19. Instituto Nacional de Estadística [sitio web]. Madrid: INE [actualizada 1 de enero 2013; consultado 29 de diciembre de 2015]. Disponible en: http://www.ine.es/inebmenu/indice.htm [ Links ]
20. García Encabo M, De la Bárcena Guallar J. Mapa sanitario de la comunidad autónoma de Aragón. Sector Huesca [monografía en internet]. Zaragoza: Gobierno de Aragón. Departamento de Salud y Consumo; 2008 [acceso 29 de diciembre de 2015]. Disponible en: http://www.aragon.es/estaticos/ImportFiles/09/docs/Ciudadano/GuiaCentrosServiciosSanitarios/OrdenacionSanitaria/MapaSanitario/MS_HUESCA.PDF [ Links ]
21. Castrodeza Sanz JJ, Alfaro Latorre M, Gogorcena Aoiz MA, Alonso Villar C, de Bustos Guadaño M, Jimenez Rosado P, et al. Catálogo Nacional de Hospitales 2015 [monografía en internet]*. Madrid: Ministerio de Sanidad, Servicio Sociales e Igualdad; 2014 [acceso 4 de enero de 2016].Disponible en: http://www.msssi.gob.es/ciudadanos/prestaciones/centrosServiciosSNS/hospitales/docs/CNH2015.pdf [ Links ]
22. Fiabane E, Giorgi I, Sguazzin C, Argentero P. Work engagement and occupational stress in nurses and other healthcare workers: the role of organisational and personal factors. J Clin Nurs. 2013 Sep; 22(17-18):2614-24. [ Links ]
23. Setti I, Argentero P. Organizational features of workplace and job engagement among Swiss healthcare workers. Nurs Health Sci. 2011 Dec;13(4):425-32. [ Links ]
24. Mahboubi M, Ghahramani F , Mohammadi M, Amani N, Mousavi SH, Moradi F. Evaluation of Work Engagement and Its Determinants in Kermanshah Hospitals Staff in 2013. Global Journal of Health Science. 2015; 7(2):170-176. [ Links ]
25. Fuentelsaz Gallego C, Moreno Casbas T, López Zorraquino D, Gómez García T, González María E, Consorcio RN4CAST-España. Perception of work environment of nurses in hospitals of the Spanish national health system. RN4CAST-Spain Project. Enferm Clin. 2012; 22(5):261-268. [ Links ]
26. Cho J, Laschinger HK, Wong C. Workplace empowerment, work engagement and organizational commitment of new graduate nurses. Nurs Leadersh (Tor Ont).2006;19(3):43-60. [ Links ]
27. Greco P, Laschinger HK, Wong C. Leader empowering behaviours, staff nurse empowerment and work engagement/burnout. Nurs Leadersh (Tor Ont).2006;19(4):41-56. [ Links ]
28. Hayati D, Charkhabi M, Naami A. The relationship between transformational leadership and work engagement in governmental hospitals nurses: a survey study. Springerplus. 2014 Jan 14;3:25. [ Links ]
29. Adriaenssens J, De Gucht V, Maes S. Association of goal orientation with work engagement and burnout in emergency nurses. J Occup Health.2015;57(2):151-60. [ Links ]
30. Berger J, Polivka B, Smoot EA, Owens H. Compassion Fatigue in Pediatric Nurses. J Pediatr Nurs.2015;30(6). [ Links ]
31. Jenaro C, Flores N, Orgaz MB, Cruz M. Vigour and dedication in nursing professionals: towards a better understanding of work engagement. J Adv Nurs. 2011;67(4):865-75. [ Links ]
32. Adriaenssens J, De Gucht V, Van Der Doef M, Maes S. Exploring the burden of emergency care: predictors of stress-health outcomes in emergency nurses. J Adv Nurs.2011;67(6):1317-28. [ Links ]
33. Sawatzky JA, Enns CL J. Exploring the key predictors of retention in emergency nurses. Nurs Manag.2012;20(5):696-707. [ Links ]
34. Laschinger HK. Job and career satisfaction and turnover intentions of newly graduated nurses. J Nurs Manag. 2012;20(4):472-84. [ Links ]
35. Rudman A, Gustavsson JP. Burnout during nursing education predicts lower occupational preparedness and future clinical performance: a longitudinal study. Int J Nurs Stud. 2012 Aug;49(8):988-1001. [ Links ]
36. Schulz M, Damkröger A, Heins C, Wehlitz L, Löhr M, Driessen M, et al. Effort-reward imbalance and burnout among German nurses in medical compared with psychiatric hospital settings. J Psychiatr Ment Health Nurs.2009;16(3):225-33. [ Links ]
37. Landsbergis PA. Interventions to reduce job stress and improve work organization and worker health. En: Schnall P, Dobson M, Rosskam E (Eds.). Unhealthy Work: Causes, Consequences, cures. Amityville, NY: Baywood Publishing Co. 2009; 193-209. [ Links ]
38. Kubicek B, Korunka C, Tement S. Too much job control? Two studies on curvilinear relations between job control and eldercare workers' well-being. Int J Nurs Stud. 2014;51(12):1644-53. [ Links ]
Received: May 23, 2016; Accepted: August 23, 2016
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
