










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.17 no.52 Murcia oct. 2018 Epub 01-Oct-2018
https://dx.doi.org/10.6018/eglobal.17.4.299971
Originals
Body mass index of pregnant women in the family health care unit
1 Enfermera, Egresada del Curso de Graduación en Enfermería de la Facultad de Medicina de São José do Rio Preto - FAMERP.Brasil. bbarco@famerp.br
2 Enfermera obstétrica, Profesora Doctora del Departamento de Enfermería Especializada de la Facultad de Medicina de São José do Rio Preto - FAMERP. Brasil.
Objectives:
To analyze the body mass index in the gestation of women attended at the Basic Health Unit; To identify the prevalence of overweight and obesity in pregnant women; To verify the gestational weight gain and to associate with the variables: age, marital status, gestational number, parity, pre-gestational weight and prenatal.
Methodology:
Quantitative, retrospective and descriptive study. Comprising 241 women who had gone under prenatal care, from 2013 to 2015. The Prevalence Coefficient (total number of overweight and obese pregnant women x 103/total number of pregnant women) was considered.
Results:
The prevalence rate of overweight and obesity was 34.54% in 2013; in 2014, of 43.61% and in 2015, of 41.34%. In the obstetric characteristics, they had a strong correlation with the total gestational weight gain at prenatal consultations and at gestational age, with a significance of P <0.0001. It was identified that the BMI of pregnant women ranged from 15.80 to 46.80 kg / m². Overweight was detected in 39.84% of pregnant women; 34.44% gained more weight than expected during gestation. While overweight 55.00% gained more weight than recommended and of those with obesity 54.77%. The correlation of pre-gestational BMI with the variables of the previous weight, the weight at the last visit and the total weight gain during pregnancy was strong with the BMI, P <0.0001.
Conclusion:
Inadequate nutritional status has been increasing over the years, strengthening the importance of a more comprehensive approach on the subject with pregnant women.
Keywords: Obesity; Pregnant women; Obstetric Nursing; Body mass index; Overweight
INTRODUCTION
Obesity should be treated as a public health problem, since its prevalence and comorbidities lead to a global epidemic condition. 1)(2)(3)(4)(5 Considered until recently as a disorder of little clinical relevance, even the scientific community related this disorder to bad habits and lack of personal determination that would affect individuals without will power, responsible for their own clinical condition.
However, it is already described as multicausal etiology, involving biological, historical, ecological, political, socioeconomic and cultural aspects, defined as a multifactorial chronic metabolic syndrome characterized by an unbalance between alimentation and caloric expenditure. 1)(5)(6) Increasing the number and size of adipose cells in the body.2)(7)
Epidemiological studies of the Brazilian Ministry of Health, "Vigilância de Fatores de Risco e Proteção para Doenças Crônicas por Inquérito Telefônico" (VIGITEL), is a system developed to monitor risk or protection behaviors for chronic diseases in the Brazilian population. 8 In order to diagnose the nutritional status of adults, the Body Mass Index (BMI) was calculated by dividing weight in kilograms / by squared height, measured in meters (kg / m²). 8 Classifying as overweight the BMI with a value equal to or greater than 25 kg / m² and obesity equal to or greater than 30 kg / m². 8)(9 Vigitel identified, in the city of São Paulo, overweight in 53.9% of the population over 18 years old, and among women the rate was 50.5%. Obesity affects 18.9% of the population and 19.6% of women. 8
Data from the World Health Organization (WHO) show an increase in the number of obese people in the world, it is estimated that in 2025, more than 700 million people will be affected by this condition.
Adequate weight gain during pregnancy for obese women is up to 6.8 kg. For those who initiate pregnancy with excess weight, a gain is estimated to range from 6.8 to 11.2 kg, while for women who are pregnant with a suitable weight, the recommended gain is 11.2 to 15.9 kg. 1
The gestational period may aggravate or trigger obesity, especially in women who are predisposed to this disorder and in those with a history of infertility. 10 Obesity leads to gestation an increase in the risk of maternal and perinatal complications such as gestational diabetes, arterial hypertension developed by pregnancy, pre-eclampsia, eclampsia, thromboembolic phenomena, urinary tract infections, preterm delivery, dystocia deliveries that increase the incidence of cesarean sections, fetal malformations, fetal macrosomia, fetal death, postpartum heavy hemorrhage, puerperal infection, maternal death, among others. 1)(4)(10)(11
Obese or overweight women who wish to become pregnant should be instructed and encouraged to lose weight previously, reinforcing the importance of preconception consultations and family planning. 9 Preventive care during pregnancy and postpartum results in the best maternal and fetal outcome. 10
In view of this problem, and with the purpose of improving care for women in the puerperal pregnancy cycle, this research had the following objectives.
OBJECTIVES
-To analyze the body mass index in the gestation of women attended at the Basic Health Unit;
-To identify the prevalence of overweight and obesity in pregnant women;
-To verify the gestational weight gain and to associate with the variables: age, marital status, gestational number, parity, pre-gestational weight and prenatal weight.
MATERIALS AND METHODS
A quantitative, retrospective, descriptive study, approved by the Research Ethics Committee of the Faculdade de Medicina de São José do Rio Preto (FAMERP), with opinion no. 1,448,790. Developed in a Basic Health Family Unit (BHFU) of Health District IV, which had a total of 169 births in 2013, 163 in 2014 and 142 in 2015, according to the Monitoring Panel of the municipality of São José do Rio Preto, located in the Northwest of the State of São Paulo, Brazil. 12
The data were collected between March and April 2016, of women's records that met the following criteria: having performed prenatal care in this BHFU from 2013 to 2015 and the one completed by the birth until December 2015. As a criterion of exclusion: the medical records that did not include the height of the pregnant woman, making it impossible to calculate the body mass index.
In the first stage of the data collection, the number of the medical records recorded in the unit's pregnant book was identified. After the collection of these medical records, the respective information was collected on social and obstetric data, personal characteristics and previous gestational history. The independent variables were: maternal age, initial nutritional status, marital status, schooling, number of pregnancies, abortion, stillbirth, complication (Gestational Diabetes/Hypertensive Pregnancy Syndrome) and underlying disease; presence of anemia and fasting glycemia.
From the height and weight data before gestation, the BMI was calculated to evaluate the weight gain and the weight was considered from the second trimester of gestation (14th week). 13
For the classification of BMI and weight gain during pregnancy, the WHO recommendation was considered: low weight <18.5 kg/m2 can gain from 12.5 to 18 kg; suitable 18.5- 24.9 kg/m² can gain 11.5 to 16 kg; overweight 25.0- 29.9 kg/m² should gain from 7.0 to 11.5 kg; obesity> = 30 kg/m² should gain from 5.0 to 9.0 kg. 13
The prevalence of overweight/pre-gestational obese women was obtained with the Prevalence Coefficient=total number of overweight and obese pregnant women x 103 / total number of pregnant women.
Statistical analysis of the data was done through the software GraphPadInstat 3.0 and Prism 6.01, and considered the level of significance of α=0.05.
RESULTS
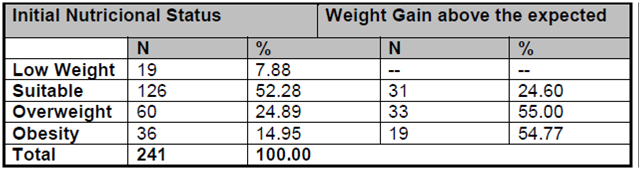
It was selected 241 (100.0%) medical records that met the inclusion criteria. In the evaluation of the nutritional status of pregnant women, the pre-gravid BMI was detected from 15.80 to 46.80 kg/m2, an average of 24.83 kg and a standard deviation of 5.48 kg/m2. Overweight was detected in 39.84% of the pregnant women, of these, 24.89% were overweight and 14.95% were obese, they gained weight above the expected 34.44% of the pregnant women.
It is noteworthy that 7.88% were underweight, and until the end of gestation did not gain excess weight. Among the overweight women, 55.00% of the pregnant women and 54.77% of those with obesity gained more than the recommended weight at gestation. (Table 1 )
Table 1 Distribution of pregnant women according to pre-gravid nutritional status and gestational weight gain. São José do Rio Preto / SP, Brazil, 2016
The prevalence rate of overweight and obesity was 34.54% in 2013, 43.61% in 2014, rising to 41.34% in 2015.
When assessing the correlation of pre-gestational BMI with the variables of the previous weight, the weight at the last visit and the total weight gain during pregnancy, there was a strong correlation with the BMI in all variables and significance with P <0.0001, according to Table 2 .
Table 2 Correlation of pre-pregnancy BMI with pre-gestational weight, weight at the last visit and total weight gain at gestation. São José do Rio Preto/SP, Brazil, 2016.

Concerning the social characteristics of pregnant women, the age range varied from 13 to 41 years, with 57.26% of pregnant women aged 20 to 29 years, and the mean of 24.53, SD = 14.10. Having a companion was 72.20% of pregnant women. Schooling varied from 1 to 9 years or more, with a mean of 5.50, SD = 1.80, women with elementary education represented 67.22%, that is, from 5 to 8 years of schooling. (Table 3 )
Table 3 Distribution of pregnant women according to social characteristics. São José do Rio Preto / SP, Brazil, 2016.
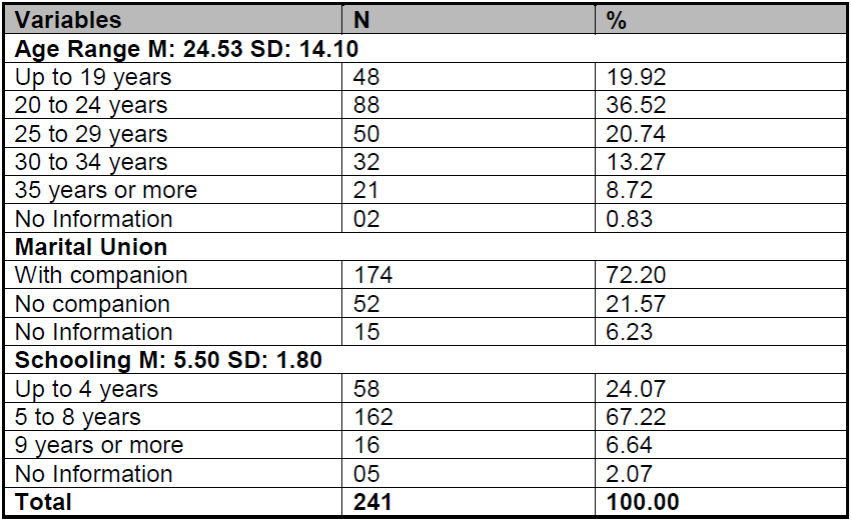
Table 4 shows the obstetric characteristics and found that 36.52% were primigravida and 17.02% had abortion in previous pregnancies. The onset of prenatal care in the first trimester was true for 71.37% of the pregnant women, with a mean of 7.34 visits, SD = 2.85, attending from 7 to 9 prenatal visits, 42.32%, followed by 34.85% who attended in up to 06 consultations. The gestational age of the last prenatal visit of 51.04% of the pregnant women was from 26 to 37 weeks.
The total weight gain during pregnancy had a strong correlation with prenatal consultation and gestational age, with an equal significance of P <0.0001. Women with high BMI reached the highest number of prenatal consultations and with the evolution of gestational age accumulated more weight than recommended.
Table 4 Distribution of women according to obstetric characteristics. São José do Rio Preto/SP, 2016.
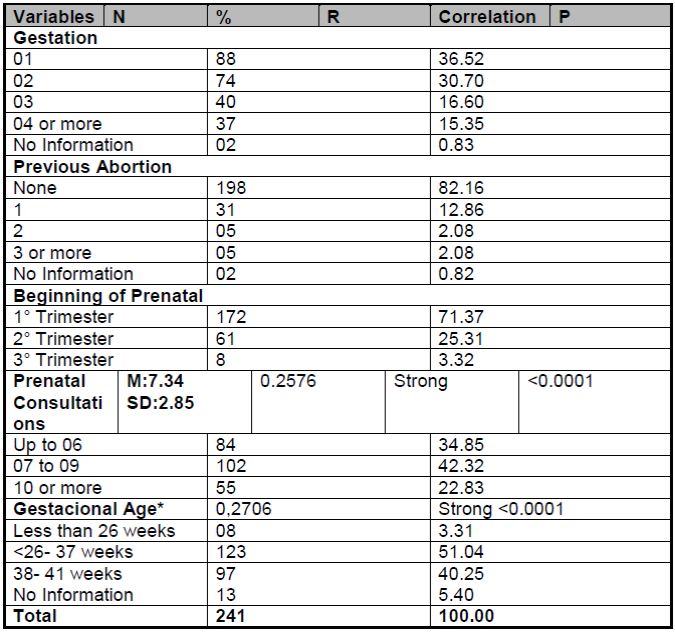
*last prenatal consultation.
At the first prenatal visit, the hemogram showed that in 9.54% of the pregnant women the hemoglobin value was up to 11g/dl, followed by 20.75% with values between 11.1 and 12g/dl and 60.59% of 12.1g/dl or more. Still, as to the hematocrit of this first hemogram, in 31.54% of the pregnant women the result was less than 36%. In relation to the fasting blood glucose values, a reliable evaluation was not possible due to the lack of information on the results of the examination in the records of pregnant women.
DISCUSSION
The nutritional status has repercussions on gestational and perinatal outcomes, hence the importance of maintaining adequate BMI during the pregnancy period and maintaining weight gain from the onset of pregnancy. 4)(14
Comparable to the described prevalence, overweight rates are described from 22.00% to 24.00% of the pregnant women in the studies, and 18.00% to 25.00% with obesity. 15)(16)(17 In contrast to the results, it was found in pregnant women in Rio Grande do Sul that 66.7% were underweight and continued until the end of gestation. 18 It is noteworthy that high BMI reflects in the lower satisfaction of the pregnant woman with her body image. 15)
It was identified women in the age group considered as a risk factor for gestation, which are those younger than 15 years and those with 35 years or more, despite the increase in the average age of pregnant women in Brazil, which has been portrayed for approximately 30 years.13)(15
The conjugal union confers emotional support to the pregnant woman, the presence and participation of a partner is fundamental for the maintenance of balanced mental health for gestational development, influence on the experienced gestation, delivery and the process of motherhood. 16 In Recife, Pernambuco, having a partner represented 74.5% of the pregnant women, equally found in Imperatriz in Maranhão. 19) (20
Low schooling is considered an obstetric risk factor that makes it difficult to understand the body's changes in this period and the decision to self-care. 16) (21 Often, schooling is linked to socioeconomic status, which, in addition to conferring a low level of schooling, it is associated with lower purchasing power, reducing access to food in qualitative terms and opting to consume more caloric ones that are generally cheaper.
The maternal education level influences the understanding of the educational activities developed in prenatal care, which aim to promote health maintenance and prevention of maternal fetal complications.15)(16)(17
Health professionals are expected to involve these pregnant women in educational actions, emphasizing the promotion of health and prevention of the damages associated with overweight during the pregnancy period. 22
High BMI correlated with the higher number of prenatal visits. The Brazilian Ministry of Health determines that prenatal care must be at least six consultations, and the earliest possible start, but the reality in the Brazilian regions diverges. In the first trimester, 54.20% of the pregnant women were seen, but 87.50% had less than six visits in Recife, state of Pernambuco, and in the city of Imperatriz, Maranhão, it was verified that 83.1% initiated in the first trimester, but 74.57% of the pregnant women were assisted in less than 6 visits. 13)(19)(20
The gestational period may trigger obesity, or potentiate a preexisting condition; the weight gain during pregnancy allows the woman to be more susceptible to excessive weight gain. 21)(22 Until the 32nd week of gestation, the woman can associate a diet for maintenance and / or weight loss in order to prevent immediate and future complications.23
In prenatal care, the evaluation of hemoglobin and hematocrit levels is fundamental; in a study carried out in Rio Grande do Sul, the prevalence of anemia in pregnant women was 48%, which indicates the need for continuity and intensification of supplementation programs, which is still a public health problem. The high rates of anemia are strongly related to schooling, which plays a fundamental role in adhering to the adequate nutritional health status. 18)(20
CONCLUSION
High pre-gestational BMI showed a significant relationship with total weight gain during pregnancy and in the greater number of prenatal visits. Excess weight gain during pregnancy prevailed in overweight and obese women in the pre-gestational period. Reinforcing the importance of the use of educative actions in women's health and of a broader approach on the subject with the pregnant women in prenatal consultations, focusing on the prevention of damages and reduction of the diseases caused by obesity in maternal and fetal health.
REFERENCIAS
1. Calderon ACS, Quintana SM, Marcolin AC, Berezowski AT, Brito LGO, Duarte G, Cavalli RC. Obesity and pregnancy: a transversal study from a low-risk maternity, Calderon et al. BMC Pregnancy and Child birth 2014, 14:249 [ Links ]
2. Carneiro JRI, Braga FO, Cabizuca CA, Abi-Abib RC, Cobas RA, Gomes MB. Gestação e obesidade: um problema emergente. Revista HUPE, Rio de Janeiro, 2014; 13(3): 17-24 [ Links ]
3. Ferreira RAB, Benicio MHDA. Obesidade em mulheres brasileiras: associação com paridade e nível socioeconômico. Rev Panam Salud Publica. 2015; 37(4/5): 337-42. [ Links ]
4. Fonseca MRCC, Laurenti R, Marin CR, Traldi MC. Ganho de peso gestacional e peso ao nascer do concepto: estudo transversal na região de Jundiaí, São Paulo, Brasil Ciência & Saúde Coletiva. 2014; 19(5): 1401-1407. [ Links ]
5. Stulbach TE, Benício HMD, Andreazza R, Kono S. Determinantes do ganho ponderal excessivo durante a gestação em serviço público de pré-natal de baixo risco. RevBrasEpidemiol. 2007; 10(1): 99-108. [ Links ]
6. Moreira M, Costa FP, Ferreira R e Da Silva MF. A importância do peso na gravidez: antes, durante e depois. Rev Port Endocrinol Diabetes Metab. 2015; 10(2): 147-151. [ Links ]
7. Silva JC, Amaral AR, Ferreira BS, Petry JF, Silva MR, Krelling PC. Obesidade durante a gravidez: resultados adversos da gestação e do parto. RevBrasGinecol Obstet. 2014; 36(11):509-13. [ Links ]
8. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Vigitel Brasil 2016: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico / Ministério da Saúde, Secretaria de Vigilância em Saúde. - Brasília: Ministério da Saúde, 2014. [ Links ]
9. Gutiérrez Valverde JM, Guevara Valtier MC, Enríquez Reyna MC, Paz Morales MdlÁ, Hernández del Ángel MA, Landeros Olvera EA. Estudioenfamilias: factoresambientales y culturalesasociados al sobrepeso y obesidad. Enfermería Global 2017161-10. [acesso em 16 de Maio de 2016] Disponível em:http://ww.redalyc.org/articulo.oa?id=365849076001 [ Links ]
10. Gomes E, Soares AL e Campos R. Obesidade e gravidez: conhecer para atuar precocemente? A realidade numa unidade de saúde familiar. RevPortEndocrinol Diabetes Metab. 2013; 8 (1): 16-20. [ Links ]
11. Braz L, Fonseca FA. Influência da Obesidade e Ganho Ponderal no Peso do Recém-nascido num Grupo de Grávidas com Diabetes Gestacional. RevPortEndocrinol Diabetes Metab. 2013; 8(2): 70-76. [ Links ]
12. São José do Rio Preto. Secretaria da Saúde de São José do Rio Preto. Painel de monitoramento do ano de 2014 a 2016 [internet]. 2016 [acesso em 29 de agosto de 2016]. Disponível em: http://gestao.saude.riopreto.sp.gov.br/transparência/modules/mastop_publish/?tac=Pain_Moni [ Links ]
13. Brasil. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Atenção ao pré-natal de baixo risco / Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. - Brasília : Editora do Ministério da Saúde, 2012 [ Links ]
14. Rosa RL, Molz P, Pereira CS. Perfil nutricional de gestantes atendidas em uma unidade básica de saúde. Cinergis. 2014;15(2):98-102. [ Links ]
15. Meireles JFF, Neves CM, de Carvalho PHB, Ferreira MEC. Satisfação corporal, idade gestacional e estado nutricional em gestantes. ABCS Health Sci. 2016; 41(1): 23-28. [ Links ]
16. Gomes RNS, Gomes VTS, Caldas DRC, Lago EC, Campos FKL, Gomes MS. Avaliação do estado nutricional de gestantes atendidas em unidades básicas de saúde de Caxias/Ma. R. Interd. v. 7, n. 4, p.81-90, out. nov. dez. 2014. [ Links ]
17. Alves KPS, Oliveira LML, Pedersoli AGA, Lemke GMMN. Estado Nutricional e Condições Socioeconômicas de Gestantes Atendidas em uma Unidade de Saúde da Família. Saber Científico, Porto Velho.2016; v.5, n.1, p.61-68. [ Links ]
18. Cunha LR, Pretto ADB, Bampi SR, Silva JMGC, Moreira AN. Avaliação do Estado Nutricional e do Ganho de Peso de Gestantes Atendidas em uma Unidade Básica de Saúde de Pelotas-RS. Revista Brasileira de Obesidade, Nutrição e Emagrecimento, São Paulo. v.10. n.57. p.123-132. Maio/Jun. 2016. ISSN 1981-9919. [ Links ]
19. Cardoso MD, Ribeiro CMS, Oliveira IB, Andrade PMC, Santos TMB. Perceptions of pregnant women about the organization of the service/ assistance in prenatal low risk in Recife. J. res.: fundam. care. online. out./dez.2016; 8(4): 5017-5024. [ Links ]
20. Aragão FKS, Almeida AL, Nunes SFL. Prevalência e fatores associados à anemia em gestantes atendidas em uma maternidade pública no município de Imperatriz, Maranhão. J ManagPrim Health Care. 2013; 4(3): 183-190. [ Links ]
21. Teixeira CSS e Cabral ACV. Avaliação nutricional de gestantes sob acompanhamento em serviços de pré-natal distintos: a região metropolitana e o ambiente rural. RevBrasGinecObst. 2016; 38:27-34. [ Links ]
22. Ferreira RAB, Benicio MHDA. Obesidade em mulheres brasileiras: associação com paridade e nível socioeconômico. Rev Panam Salud Publica. 2015; 37(4/5): 337-42. [ Links ]
23. Oliboni CM, Alvarenga MS. Atitudes alimentares e para com o ganho de peso e satisfação corporal de gestantes adolescentes. Rev Bras Ginecol Obstet. 2015; 37(12): 585-92. [ Links ]
Received: June 10, 2017; Accepted: September 21, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
