










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.17 no.52 Murcia oct. 2018 Epub 01-Oct-2018
https://dx.doi.org/10.6018/eglobal.17.4.304901
Originals
Effectiveness of the implementation of community IMCI strategy in Montería, Colombia
1Enfermera. Magister en Salud Pública. Docente Universidad del Sinú Elías Bechara Zainúm. Montería. Córdoba. Colombia. caipachope@gmail.com
2Enfermera. Magister en Enfermería. Docente Titular Universidad de Córdoba, área investigación. Córdoba. Colombia.
3Enfermera. Magister en Desarrollo Social. Docente Asociado Universidad de Córdoba área Salud Colectiva. Córdoba. Colombia.
Objective
Describe the scope that has been the strategy Integrated management in childhood Illness (IMCI) on morbidity and mortality in children under five years living in the South of the municipality of Monteria (Cordoba, Colombia).
Methodology
Descriptive study, social, quantitative approach. It was interview with 145 caregivers of children to assess knowledge, applicability of the 18 key practices, and felt morbidity of diseases subject of strategy in 87 families with homes in strata 1 and 2. The official information on the rates of infant mortality (2005-2015) of the municipality was used to analyze the trend of this indicator.
Results
The most used practices are those relating to competences for disease control subject of the strategy (80% to 99.3%), however, a high percentage (66.9%) does not recognize the warning signs; lesser used practices related to the promotion of health and prevention of diseases prevalent (23%-57, 9%). Social mobilization with ethno-cultural approach has an intermediate level of frequency of use (60% to 79%). Diarrhea and pneumonia predominate, more permanent learning relate to key practices 11, 12 and 17; the less applied are key practices 3, 7, 8, 9 and 10. Lower sustained mortality was observed after the implementation of the strategy IMCI.
Conclusions
The parents and caregivers of children give more importance and differential applicability for the control of diseases than for their prevention.
Keywords: children; mortality; morbidity; caregivers
INTRODUCTION
During Millennium Summit of the United Nations in 2000, the global goals in development were defined, the global goals were defined, among these it can be mentioned that by 2015 the mortality of children under 5 years must be reduced by two thirds; the signature of this commitment, is raised among other causes because it is estimated that in the world 37% of deaths in this age group occur within the first month of life, it is interesting to note that 97% of these cases are of unknown cause.(1
Some International organizations have considered that a percentage close to 26% of neonatal deaths have an apparent origin in intrapartum problems that lead to perinatal asphyxia, which point into 10% of deaths in children under 5 years. This situation has influenced the Pan American Health Organization in partnership with the World Health Organization (PAHO / WHO), with the support of the United Nations Children's Fund (UNICEF), to develop the strategy called Integrated Management of Childhood Illness (IMCI) as an effective tactic, which presents a unique way to address the child's care, both in health services, as well as in the family and in the community. 2
Considering these elements, in 2005, on the occasion of World Health Day, the Pan American Health Organization and the World Health Organization - PAHO / WHO launched an initiative called "Make every mother and child count", a significant fact that represented the health sector a call for the integration of care to the mother-baby binomial in favor of child and maternal health; This initiative was subsequently approved at the 47th Directing Council of the World Health Organization in 2006, and its foundation served as a basis to support the creation of regional alliances and plans, which resulted in the elaboration of a strategy called “ Integrated Management of Childhood Illness” and is internationally recognized as the IMCI strategy; which allows not only the comprehensive approach to the health of children in early childhood, but also provides tools for the detection and management of risks that may occur in women during pregnancy and labor, as well as risks in the newborn; This strategy has its main support in the capacity to empower individuals, families and communities for the health care of the maternal and child population. 3
The strategy is structured by three components, all of them aimed at diminishing morbidity and mortality in children under five years of age. Its implementation demands political, social, technical and financial commitment of all the actors of the System; but besides requires that primary and secondary prevention measures be applied in cases of disease subject to the strategy, due to which it is necessary and unavoidable to meet the goal of informing and educating parents about prevention and promotion of health childish. The components of the strategy are the following:
Management: this component is designed to improve the organization and functioning of the health systems required in order to offer efficient and quality care, by increasing the resolution capacity of primary health care services.
Clinical: by means of this component it is intended to develop in health professionals, the ability for early identification and timely treatment for children under five years of age; for this purpose, it uses the teaching, supervision and provision of guides adapted to local scenarios on the needs for comprehensive and integrated care of childhood diseases as well as the set of activities to promote its use.
Community: this component of the strategy incorporates a series of key family and community practices related to the care and attention of children in the home, aimed at improving child survival rates, maintaining appropriate healthy growth and development; It is based on the need to empower parents and caregivers of children in the most appropriate ways to maintain the health in the home.
In summary, these three components, when integrating their development, seek to ensure timely detection and effective treatment in health services, in the same way, that at home and the community, the knowledge is reached to achieve the prevention of diseases; and the early and timely identification of complications during the care of children bearing from the diseases subject of the strategy.
So the IMCI strategy is an effective instrument based on the right of every child to be treated with quality and warmth, which adopts a risk identification and total integration approach, which involves the broad coverage of knowledge by the family and the community on diseases that lead to infant mortality. 4
Among these diseases are pneumonia, diarrhea and neonatal problems, considered the "big murderers" of children, that in the company of malnutrition are the root cause of more than half of all deaths in this age group, reaching figures of almost six million deaths in children under five years of age due to causes that can be prevented with available and feasible interventions. 5)(6
In this group of pathologies is community-acquired pneumonia, which is an acute inflammatory process of pulmonary parenchyma of infectious origin, the causative agents of extra institutional childhood pneumonia are mostly of bacterial origin, although they may also be of fungal origin or viral infections that are more frequent in children older than 5 years; as such it is not a unique process, but a group of infections caused by different microorganisms, which conditions an epidemiology, a pathogenesis, a clinical picture and a different prognosis in each population group, being the treatment of bacterial pneumonias more expensive than viral pneumonias; pneumonia is responsible for 15% of all deaths of children under 5 years of age and is estimated that killed some 922,000 children in 2015. (7)(8)(9)
Considering the evidentness of these statistics, it is considered that the prevention of childhood pneumonia is an essential aspect to reduce infant mortality. Other forms of prevention contemplated in the strategy are immunization against Hemofilus Influenza type B (Hib), pneumococci, measles and whooping cough, accompanied by home practices such as balanced nutrition, which is undoubtedly essential to improve the child's natural defenses, this begins with exclusive breastfeeding during the first six months of life. Other family practices that can contribute to reduce the incidence of pneumonia in children are intervening environmental risk factors such as air pollution by particles. 10
In the less developed municipalities of Colombia, Acute Diarrheic Disease (ADD) is the most frequent cause of morbidity and mortality in the population under five years of age, clinical complications and death are due in general to dehydration (76.7%) and anorexia (70.5%) that occurs in these cases, which justifies the inclusion of ADD in the strategy that involves both prevention programs and activities for the identification and control of their associated complications. 11
Concerning to neonatal morbidity related to mortality, a cohort study conducted between 2002 and 2003 was analyzed, this prospective study had women as subjects between 20 and 26 weeks of pregnancy; in the follow-up to this group, a neonatal mortality rate of 47.3 per 1,000 live births was identified. Being found that among the main causes that led to these deaths were premature births (34%); among those born by cesarean section of emergency was due to complications of labor, the main cause of neonatal mortality was intrapartum hypoxia / anoxia (26%). In detail, neonatal mortality registered 45% during the first 48 hours after birth, and 73% during the first week of life. It is relevant to highlight that the result that shows as the professional assistance of the childbirth, or that the labor was made inside a health center was not associated as expected with a lower incidence of mortality in the neonatal period. 12
Regarding to the mortality rate of children under 5, the target set for 2015 is 4-5 per 1,000 live births for developed countries and 35 per 1,000 live births for underdeveloped countries. In this respect for the year 2007 countries like Colombia, Brazil, the United States, Norway and Sweden reached that goal. 13
Due to this, within the IMCI strategy, it is understood as an impact on health a short-term decrease in mortality due to these causes, based on the precept that educating mothers and caregivers about how to prevent prevalent diseases of the childhood; promotes and reinforces protective factors such as breastfeeding, nutrition, immunization and affection, on the potential positive effect that teaching parents to recognize the signs of danger consulting on time decreases long-term mortality.
In Colombia, notwithstanding the efforts made, mortality among children under five years of age seems to be an uncontrolled problem. It is known from reports from the Epidemiological Surveillance System (SIVIGILA) that persistently high rates and marked regional differences in infant mortality occur. For Colombia, the commitment to reduce infant mortality means reducing the mortality rate in children under 5 years to 17 deaths per 1000 live births and reducing mortality in children under 1 year old to 14 deahs per 1000 live births. 14)(15)(16
The mortality rate is a very useful indicator of health to measure the result of the interaction of social determinants of health, such as the mother’s knowledge about health care, the security of food disposition, the level of household income, access to health services, quality of care, access to potable water and basic sanitation facilities. 17
The third component of this strategy empowers families and communities in terms of the responsibility to provide care for children and provide conditions and spaces that allow for optimal growth and development through the implementation of educational programs aimed at preserving the health of children. This component is reflected in policy line number 1, about the promotion of health and quality of life that in its paragraphs "b", "c", "d", "g" and "h" defines a series of aspects that must be fulfilled at home, by parents and caregivers:
Development of community-based initiatives to improve the skills of individuals, families and the community in the prevention and control of prevalent childhood diseases, Integrated Management of childhood Illness - IMCI.
Development of community-based initiatives to improve the skills of individuals, families and the community for the promotion of good treatment of children and the peaceful resolution of conflicts.
Develop and evaluate education, information, communication and social mobilization strategies with an ethno-cultural focus, to promote rights in childhood health and healthy lifestyles.
Promote at home and in institutional settings such as nurseries and family welfare homes, hygienic habits of oral health routine of daily care from birth, early childhood and school age.
Promote protective factors for oral health among parents and caregivers, such as not using baby pacifiers and bottles, establishing oral hygiene habits and emphasizing the importance of the care of the sixth molar and the control by a dentist.
In the report of the Ministry of Social Protection in Colombia, related to the situation of the IMCI strategy in 2010, an analysis is made from the territorial management, which reports that of 37 Territorial Health Directions (DTS by its initials in Spanish), 56.8% claimed to have counted their community agents, 54.1% said that he monitored them and had instruments for the execution of said monitoring. Regarding the conditions to carry out the activities within the strategy, it is identified that 51.4% showed that community agents have supplies for their work, which come mainly from the DTS themselves and the Non-Governmental Organizations (NGOs) that work in the territories. (18
Regarding the prioritization of the key practices, all the DTS report to the Ministry of Social Protection of Colombia that have completed the gathering of the information for the baseline and have carried out the prioritization of the same. For this procedure he referred to the use of methods such as the use of focus groups, groups of experts, and the analysis of the surveys applied in the realization of the baseline. 18
With all this information, it is reasoned that the community IMCI since 2010 has trained the agents and members of the communities in the national territory, which motivates the interest of "comparing morbidity and infant mortality rates in the municipalities at the beginning and the end of the strategy implementation "study in which we analyzed the ways in which adult caregivers of children in the southern sector of the capital city of the Department of Córdoba (Colombia, South America) perform the 18 key practices included in the IMCI strategy in order to keep children healthy; whose results are presented in this article.
The official launch of the strategy in the Department of Córdoba was made on September 10, 2009; However, the aforementioned report reports that Córdoba is classified in the intermediate range within the DTS functionality when a combination of problems is identified with the management of the work teams, absence of groups, responsibility of the strategy in charge of the referent , or teams overloaded because they simultaneously participated as active members in various programs with different responsibilities; in addition to the ignorance of some normative and theoretical elements of the strategy and difficulties in the consolidation of internal and external alliances to the Territorial Health Directorate (DTS). 19
MATERIALS AND METHOD
Type of study
The research is classified as descriptive, transversal, with a social focus, as it describes the reach of the IMCI strategy on the morbidity and mortality event in the population subject of the strategy; depending on the level of measurement selected corresponds to a quantitative design, the results are reported using measures of central tendency and epidemiological measurements.
Unit of Analysis
The child care practices were applied after the implementation of the Community IMCI strategy in the families living in 7 of the 23 neighborhoods that make up the southern sector of the city of Monteria, capital city of the Cordoba State (Colombia) these neighborhoods were La Candelaria, La Esperanza, Cantaclaro, Mogambito, Ranchos del Inat, San Martin and Edmundo Lopez.
Sample
The sample consisted of 145 study subjects constituted by 87 mothers and 58 caregiver grandmothers of children, located among 107 families living in the southern sector of the municipality of Monteria, who constituted the reference population.
Sampling at the community-family level was not probabilistic or intentional, only families that had at least one child of less than five years among its members were included and that the family members responsible for their care had been intervened for educational activities of the strategy IMCI.
To measure the impact of infant mortality in the municipality, the sources were the official records of mortality in children under five years of age in a previous period constituted by statistics from 2005 to 2009 and statistics after the implementation of the 2010 strategy to 2015 to carry out the evaluation of the impact of the strategy on the general rate of infant mortality in children under five years of age. The results obtained were analyzed comparing what was expected with the goals of the strategy and with the national statistics to interpret the impact result.
The primary source was used, with the main informants being the parents and caregivers of children under five years of age in regards to the 18 key practices contained in the IMCI strategy.
For the purpose of studying the aspects related to the measurement of care that family members, parents and caregivers offer their children, a series of questions were designed to obtain the information required to evaluate the knowledge and applicability of the 18 key practices of the Community IMCI Strategy; The semi structured interview was designed consisting of 20 open and closed questions aimed at identifying the knowledge of the interviewees on the subject. To this interview, facial validity was carried out, pilot test and after adjustments were applied to an equivalent to 10% of the estimated sample to verify suitability.
RESULTS
The neighborhoods in which the measurements were made correspond to 30.4% of the southern sectors of the municipality, which is characterized as the most populated in the city, also by the precarious condition of its inhabitants according to which 67% of families have income lower than current legal monthly minimum wage in Colombia, 25% earn a salary and 8% a minimum and a half wage.
About 8% of families in the sector have children under 5 years of age among their members; A total of 158 children under five years old were identified in the 87 families surveyed; On average there are 2 children per family; the age range of the children in the targeted families was thus distributed 46% for ages between 3 to 5 years old; 36% in ages of 1 to 2 years old and 4% of children under 1 year old.
The care of children in 59% of the surveyed households is provided directly by their mothers, while 41% of this care is in the hands or under the responsibility of the grandmothers (21% maternal grandmother, 7% paternal grandmothers, 13% of them alternate care) for those cases in which both parents work outside the house.
Among the 18 Key Practices three (33.3%) are accomplish in percentages that exceed 80% of parents and caregivers of children under 5 years old; these are related to the control of the diseases subject of the strategy (in this group of competencies, key practice 16 is excepted, relative to "recognizing the signs of danger in the disease and recognizes when it is necessary to seek timely help".
In the competences related to the fulfillment of social mobilization with an ethno-cultural focus, to promote the rights in childhood health and healthy lifestyles, it is identified that these recommendations are followed and put into practice by a range between 60% and 79% of parents / caregivers.
While the key practices 3, 7, 8, 9 and 10 that contribute to the members of the families the competition for the promotion of health and for the prevention of the prevalent childhood diseases are only fulfilled by a range between 23 % and 57.9% of parents and caregivers; of them the least used is the key practice number 9 about the care of the oral cavity.
Table I Key practices used by parents and caregivers for the prevention and control of diseases prevalent in childhood
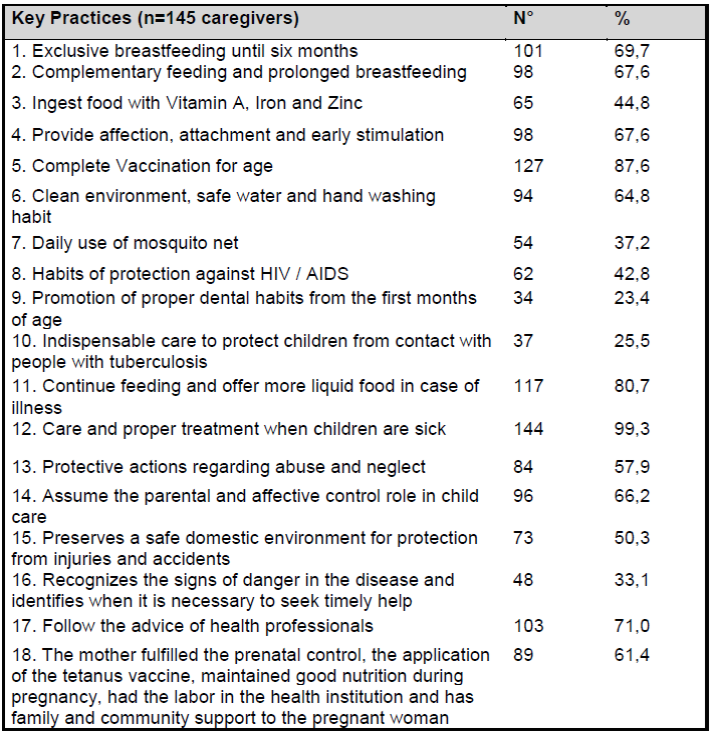
Primary source: Information obtained by direct interview
This differential behavior between groups of educational information in favor of prevention of health alterations, shows that families give greater importance to special aspects, detracting from interest in preventive practices in the family daily life, perhaps neglecting these aspects of health promotion, considering them "excessive" or "inoperative" as a safe home environment, oral cavity care, promotion of dental habits from an early age, consumption of certain foods rich in vitamins and minerals; all this group of recommendations obtained a low percentage in both knowledge and practices. In the key practice group with a small percentage, only the key practice 16 that deals with the "ability to recognize the warning signs and when to seek help" is excluded from the set of recommendations for health promotion, since its intrinsic content is part of the competition control of the diseases subject of the strategy.
In these families with children under five, is identified a low frequency of diseases of interest in public health in the last year, parents / caregivers report that the event with the greatest presentation in this town sector of the city is the group of the ADD, followed in order of frequencies by pneumonias. The cases received medical attention in the primary care agencies and none required hospitalization.
Table II Felt morbidity of prevalent childhood diseases

Primary source: Information from the direct interview
The cases of neonatal problems required specialized attention, among them 5/8 (62.5%) neonates were assisted and monitored ambulatory and 3/8 (37.5%) required institutionalization. The malnutrition identified corresponded in the eight cases to acute protein-calorie malnutrition and was reversed within three months.
The main care offered by the caregivers to children's illnesses are those recommended within the strategy in key practices 11, 12 and 17, which seem to have been the most permanent learning of the interviewees, which is reflected in the group of care practices performed by sick children.
However, it is alarming that 66.9% do not recognize the signs of danger in the disease and are unable to recognize when it is necessary to seek timely help; this aspect should be highlighted in the group and individual educational sessions that take place within the community IMCI strategy.
To identify the impact of the IMCI strategy on child mortality in the municipality, the official databases were consulted at local, national and international levels in order to analyze the behavior of under-five mortality in the period before and after the strategy.
The infant mortality rate is an indicator that accounts for the number of deaths of children under one year old in a given year, calculated from the base of every 1,000 children born alive in that same year. At the municipal level there is a notable decrease in the infant mortality rate in the two years following the implementation of the IMCI Strategy at the departmental level, which may be due to the fact that Monteria was the first municipality to initiate the implementation of the Community IMCI Strategy. 14-15
The trend in mortality, however, shows a slight increase in infant mortality between 2011 and 2012; the difficulties of this period have apparently been controlled and a progressive and sustained decline in infant mortality was established in 2014 and 2015.
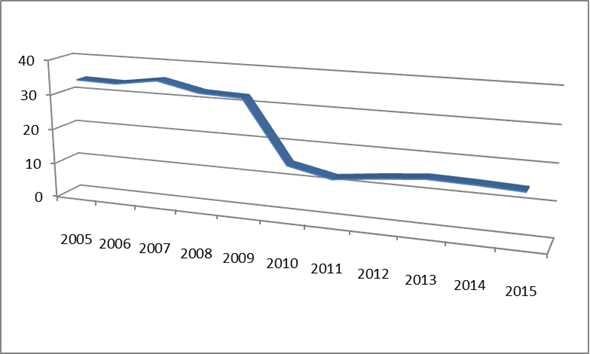
This behavior demonstrates the real effectiveness of the IMCI strategy in reducing infant mortality; As can be seen, the impact of the strategy is social, economic and statistical in terms of improving the living conditions of children in the territory where it has been implemented; This demonstrates the validity and potential of the Community IMCI strategy to achieve the desired goal of reducing the mortality rate in infants.
It should be remembered that these important results and impacts of the community IMCI strategy on infant mortality are given even under conditions in which the educational and family counseling issues to the caregivers can improve in the aspects identified as weaknesses in education for families that are presented in table I .
When comparing municipal and national infant mortality rates, we observe the wide gap that existed at the beginning of the analyzed period, which has been closing in the period after the implementation of the IMCI Strategy, it can be seen that since the implementation the municipality of Monteria has maintained infant mortality rates even below national rates, even with the slight increase in the mortality rate in 2013. 17
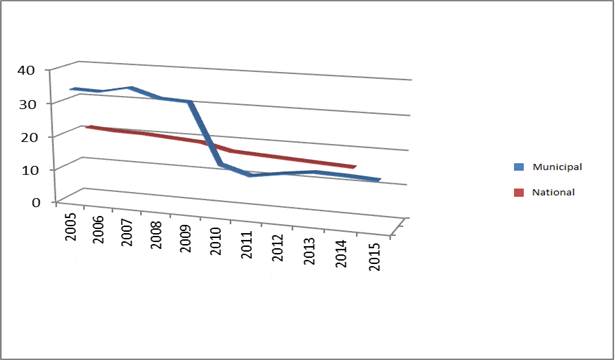
The effectiveness of the strategy is evident as a positive indicator of health for the children living in the municipality of Monteria (Cordoba, Colombia). It also demonstrates the importance of education and the empowerment of families on the basic aspects that are required to conserve children's health. It is important to highlight that even in a field of shortcomings in educational results and deficiencies in the 18 key practices, the strategy has a high potential to demonstrate its validity and to be able to comply with the fourth Millennium Development Goal (MDG 4) that contains the commitment of the territorial entities to reduce by two thirds the mortality rate in children under 5 years by 2015, likewise, the IMCI strategy, is also valid in light of the Sustainable Development Goals, as it contributes to the achievement of objectives 3 and 4, to uphold actions to promote health, promote the achievement of well-being among all ages, ensure inclusive education and promote lifelong learning opportunities. 20
DISCUSSION
Regarding specific perinatal mortality, the diagnosis of maternal and perinatal health, which contains the statistics from the Cordoba State, reports that 85% of the neonates died in a health institution independent of their level of complexity, detailing the complexity, the high prevalence complexity and intensive care service, 10% die at home; Likewise, the source in question describes the causes of neonatal mortality among which those associated with the respiratory system stand out, among them, respiratory insufficiency of the newborn, bacterial sepsis of the newborn, unspecified and newborn respiratory distress. In this group of deaths neonatal deaths predominate over fetal deaths (60 Vs 80) with the early neonatal period being the most frequent. 21
The same report from the Ministry of Health and Social Security of the Town Hall of Monteria cited that "the time when the event is most present is the postpartum Hospital pre-discharge with 45% of cases, which reflects deficiencies in the quality of neonatal care and / or the result of the complications of prematurity; followed by the antepartum with 21% this moment corresponds to intrauterine deaths and reflects problems related to maternal health that complicate the normal development of pregnancy; 15% postpartum hospital post-discharge "these conditions seem to reflect operational problems or other order associated with the service offered by the providers, which should alert the training institutions and providers to control these deficiencies identified by the competent body. 21
Regarding other factors that have a negative effect, limiting the positive impact of the strategy, the same report has described that according to the BABIES matrix, the main problems related to the occurrence of the event on infant mortality are those related to maternal health, followed by problems arising from newborn care at the level of health institutions and thirdly, prenatal care; which reflects apparent deficiencies in the implementation of clinical IMCI, considering that the report defines possible “deficiencies in preconceptional care - family planning and mothers without the clinical conditions suitable to initiate or attend a pregnancy process which translates into new Preterm infants, also show deficiency in the institutional care provided to these”, therefore, it is recommended that the process of prenatal care be analyzed, to control the failures of procedures that may be affecting the quality of care in pre-natal health agencies, intrapartum and postpartum including care provided in the neonatal period by the health team. 18)(19)(20)(21)(22)(23
Ostensible failures that still maintain inadequate levels of infant mortality rates do not seem to be related to the community IMCI strategy, nor to the family structure despite the fact that the educational aspects barely reach the third quartile in the measurement of the indicators of educational success in health; but with inherent aspects of clinical IMCI that apparently has not been disseminated and implemented in its entirety in the second and third level municipal care organizations. 3)(4)(5)(6
In effect, families have incorporated 45% of key practices as part of their cohesive social system through the creation of healthy common cultures and routines, even in the context studied, in which the existence of children living in poverty prevails, in families in which both parents must achieve job placement to be able to satisfy minimum basic family needs. 16
CONCLUSIONS
The impact of the IMCI Strategy on infant mortality in Monteria (Córdoba, Colombia) is unmistakable in accordance with the reports and official information of the municipality, mortality rates have remained below the national rate since the implementation of the strategy.
Parents and caregivers give different levels of importance and applicability to the 18 key practices, the most used are related to the competences for the control of prevalent diseases; with the only exception of the identification of the warning signs.
REFERENCIAS
1. Organización de las Naciones Unidas. Objetivos de desarrollo del milenio. Cumbre de la ONU. 20 al 22 de septiembre de 2010 Nueva York. Documento pdf. Pág. 26-28 [ Links ]
2. Scucces, M. Restricción del crecimiento fetal: factores de riesgo. Rev. Obstet. Ginecol. Venezuela, 2011. 71(4), 231-239. [ Links ]
3. Díaz Lemus, M. Introducción del manual de enfermedades prevalentes de la infancia en la enseñanza de enfermería en cuba. 2012. Revista cubana de enfermería, 28(2), 118-124. [ Links ]
4. Chia-gil A., Pariona R., Soto V., Cuipal J., Romaní D., Díaz, et al. Lactancia materna exclusiva y enfermedades prevalentes de la infancia en menores de seis meses. 2013. Revista peruana de epidemiología [internet], 17(2), 1-8. [ Links ]
5. Rincón M.V.B., López Dd. F. Atención integrada a las enfermedades prevalentes de la infancia-aiepi-para ferropenia en niños manizaleños. 2011. Revista de salud pública, 13(1). [ Links ]
6. Benguigui Y. (2012). La estrategia aiepi y su contribución a la salud infantil nuevos paradigmas en la enseñanza de la pediatria. 2012. Cuadernos esp, 1(1), pág-23. [ Links ]
7. Martín A. A., Moreno-Pérez D., Miguélez S. A., Gianzo J. C., García M. G., Murua J. K., et al. Etiología y diagnóstico de la neumonía adquirida en la comunidad y sus formas complicadas. In anales de pediatría 2012. (vol. 76, no. 3, pp. 162-e1). Elsevier Doyma. [ Links ]
8. Toledo Rodríguez I. D. L. M., Toledo Marrero M. D. C. Neumonía adquirida en la comunidad en niños y adolescentes. 2012. Revista cubana de medicina general integral, 28(4), 712-724. [ Links ]
9. Calderón C., Dennis R. Economic cost of streptococcus pneumoniae community-acquired pneumonia, meningitis and bacteremia in an adult population that required hospitalization in bogotá, colombia.2014. Biomedica, 34(1), 92-101. [ Links ]
10. Organización Mundial de la Salud. Neumonía. Nota descriptiva n° 331, noviembre de 2015. En: http://www.who.int/mediacentre/factsheets/fs331/es/ [ Links ]
11. Gnzales S., Bada M., Rojas G., Bernaola A., Chávez B. Guía de práctica clínica sobre el diagnóstico y tratamiento de la diarrea aguda infecciosa en pediatría perú-2011. Revista de gastroenterología del perú, 31(3), 258-277. [ Links ]
12. Mendoza l. A., Arias M., Mendoza l. I. Hijo de madre adolescente: riesgos, morbilidad y mortalidad neonatal. 2012. Revista chilena de obstetricia y ginecología,77(5), 375-382. [ Links ]
13. Perales j. A. S. Entre los objetivos de desarrollo del milenio y la cooperación sur-sur: actores y políticas de la ayuda al desarrollo en américa latina y el caribe. (2011). Pensamiento iberoamericano, (8), 195-222. [ Links ]
14. Colombia. Ministerio de salud. Instituto Nacional de Salud. Subdirección de Vigilancia Epidemiológica. Protocolo de vigilancia en salud pública. Pro-r02.024 versión 03 2016; 1 (30): 4-8 [ Links ]
15. Colombia. Ministerio de Salud. Instituto Nacional de Salud. Informe final evento mortalidad perinatal y neonatal tardía 2013. Documento pdf pág. 15 [ Links ]
16. Vázquez S. T. Más allá de 2015: objetivos de desarrollo del milenio y desafíos para la nueva agenda internacional de desarrollo. 2011. Sistema: revista de ciencias sociales, (220), 33-58. [ Links ]
17. Colombia. Ministerio de Salud. Análisis de la situación de salud: Colombia 2014. Imprenta Nacional de Colombia. Primera edición. Diciembre de 2014. Pág. 98-108 [ Links ]
18. Colombia. Ministerio de la Protección Social. Situación de la estrategia aiepi año 2010 un análisis desde la gestión territorial. Convenio cooperación técnica no. 637 de 2009 Ministerio de la Protección Social-Organización Panamericana de la Salud consultor: edinson bohórquez. Documento pdf. Pág. 50 [ Links ]
19. Córdoba. Gobernación de Córdoba. Lanzamiento de la estrategia aiepi en el departamento de córdoba. Boletín no. 288 de septiembre 11 de 2009 http://www.cordoba.gov.co/v1/boletines_2009/boletin_09-11-2009.html [ Links ]
20. Central Intelligence Agency. Cia world factbook. Cuadros de datos históricos anuales. Información actualizada a enero 1 de 2015. En: https://www.cia.gov/library/publications/the-world-factbook/ [ Links ]
21. Rendón M. T., Gonzales J., Apaza D. H., Riega R., Pinto M., Ortiz, P., et al. Mortalidad perinatal estudio colaborativo institucional hospitales del sur del Perú. 2017. Ciencia & desarrollo, (7). [ Links ]
22. Córdoba. Alcaldía de Montería, Secretaría de Salud y Seguridad Social. Situación de la mortalidad materna y perinatal - ii trimestre 2015-07-30 - salud pública en: http://salud.monteria-cordoba.gov.co/?accion=noticia&id=27. Consultado agosto de 2016 [ Links ]
23. Távara L., Sacsa D., Frisancho O., Urquizo R., Carrasco N., Tavera M. Estado actual de la mortalidad materna en los hospitales del Perú. 2015. Revista peruana de ginecología y obstetricia,45(1), 38-42. [ Links ]
Received: September 22, 2017; Accepted: October 07, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
