










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.17 no.52 Murcia oct. 2018 Epub 01-Oct-2018
https://dx.doi.org/10.6018/eglobal.17.4.310741
Originals
Evaluation of patient safety climate in an ophthalmic surgical hospital
1Enfermera, Maestra en Salud y Tecnología en el Espacio Hospitalario de la Escuela de Enfermería Alfredo Pinto, miembro del Sector de la Seguridad del Paciente de la Secretaría de Salud del estado de Río de Janeiro/SES. Río de Janeiro. Brasil. isabelleamorim2016@gmail.com
2Enfermera, Doctora y Maestra en Neuroinmunología. Profesora del Departamento de Enfermería de la Escuela Alfredo Pinto. Programa de postgrado en Salud y Tecnología en el Espacio Hospitalario/ Universidad Federal de Río de Janeiro UNIRIO. Brasil.
Objective:
Evaluate the security climate in an ophthalmic surgical hospital through the perception of its professionals.
Method
Exploratory, descriptive and transversal study of quantitative nature. Developed from October to January 2016 through the application of the Safety Attitudes Questionnaire (SAQ) to 61 different categories of health professionals being only considered for 27 of the questionnaires applied analysis
Results:
The average score obtained through the six domains of SAQ-climate of teamwork, safety Climate, job satisfaction, stress Recognition, perception of management and working conditions-showed concordance index below 75 points from the range of Likert, indicating a negative perception of safety climate.
Conclusions:
The study pointed out weaknesses in six areas, suggesting the development of actions focusing on improving security climate as a priority measure in ensuring the safety of the surgical patient.
Keywords: Organizational culture; Patient safety; Perioperative Nursing
INTRODUCTION
Public policy and patient safety practices have been widely discussed all over the world. The evidence points the occurrence of avoidable damage caused to the patients against risks related to health care.
Became a priority for the World Health Organization (who) reduce the adverse consequences of unsafe acts in health care and in this way, directing efforts focused on developing standards and safe practices in patient care. Created in 2004, the World Alliance for patient safety aligned its guidelines in the campaign development termed as: "global challenges for security the patient " (1 .
Safety in surgical assistance stands out among the challenges posed to health by setting itself as the second global challenge in 2007-2008 since the events (EAs) surgical adverse occupy a role of paramount importance in the health setting front frequency with that occur, the considerable impact brought to patients ' health, the economic impact in the social and health spending and because in part are attribuTable to the shortcomings in attention to health 2 .
The surgical environment is defined as a risk scenario, involving a range of critical and interdisciplinary actions steps, where work processes are considered complex, exerting strong dependence on individual and team performance in environmental conditions, dominated by pressure and stress (3
As well as these factors, others are also determining factors and contribute to the occurrence of serious incidents on surgical assistance and are related to organizational structure and human: inexperience of the surgeon, hospital surgery volume, low load excessive work and fatigue, inadequate technology or unfamiliarity with equipment, deficiency in the supervision of interns, miscommunication between the professionals, the rush, the time of completion of the procedure and faults administrative provisions (4)(5 .
The quest for quality assurance of healthcare and patient safety permeates the need for health services managers disseminate an evaluative culture of the Organization; This aspect, considered the national patient safety Program in 2013 when considered within their specific objectives, the development of strategies for the promotion of safety culture with emphasis on learning and organizational improvement, involvement of professionals and patients in preventing incidents 6 .
Monitor and evaluate the safety culture in healthcare organizations enables the identification and management of patient safety in the surgical environment, providing a subsidy to a situational diagnosis, continuing education programs, implementation of assistance protocols and monitoring of adverse events (7 .
Strengthen patient safety culture as factor in deployment strategy guidelines and Clinical-surgical protocols in order to secure assistance is determining factor. (5 .
The reference literature "safety climate" as the measurable component of safety culture being evaluated through individual perceptions and attitudes of professionals, being referred to as temporal measurement of the State of the safety culture of an institution ((8, 9.10)). It is worth mentioning that some opinion leaders, organizations and newspapers use the terms interchangeably culture and climate 9 .
Different scales have been used to measure the security climate since the beginning of the years 1980, being considered important tools in evaluating the quality of health care. Among the employed, the SAQ-Safety Attitudes Questionnaire, constitutes the instrument more sensitive to assess individual attitudes related to patient safety, having already been applied on Chinese version in Taiwan hospitals, in Denmark and in hospitals in Sweden (7)(8)(11 .
Thus, the present study aims to assess the climate of security in an ophthalmic surgical hospital through the perception of its professionals by assessing the domains of the SAQ and identify aspects related to patient safety that may interfere with the quality and safety of surgical care.
MATERIALS AND METHOD
Exploratory, descriptive and transversal study of quantitative nature developed in a private hospital, specializing in ophthalmic surgery, located in the municipality of Niterói-Rio de Janeiro, being developed in the period from October to January 2016.
The present study was extracted from the master thesis titled: "Safe Surgical Care in Ophthalmology: Adaptation and Operationalization of the surgical safety checklist" presented at Programa de Pós-Graduação em health and hospital space technology as requirement for obtaining a Masters degree in nursing at the Federal University of Rio de Janeirobeing respected the ethical aspects of research with humans having approval issued by the ethics on Research Committee of the UNIRIO, under paragraph CAAE: 48307515.90000.5285, in accordance with the guidelines contained in resolution 466/2012 of the National Health Council.
The team of health professionals who have agreed to participate in the survey received and signed an informed consent (TFCC) in two ways.
Were considered as a criterion for inclusion, health professionals of the frame of the institution involved directly or indirectly in the process of caring for patients undergoing ophthalmologic procedures having expertise in this area in at least six months. As a criterion for deletion, it was decided to not include the professionals who were out of work in the period of data collection, on grounds of license for health treatment, pregnancy or vacation.
As a research tool has been used the safety Attitudes questionnaire (SAQ) -Safety Attitudes Questionnaire-Short Form, 2006 autoaplicável instrument, intended to evaluate the perception of professionals in relation to security issues; allowing to evaluate the safety culture in hospitals by analyzing the security climate. Chosen for the development of the study allowed to be applied to any hospital area with the objective of measuring the perception of safety climate (9)(12 .
The questionnaire is composed of 41 total items, divided into two parts, where the first part is composed of 36 items distributed in six areas: climate of teamwork (items 1 to 6); Climate of security (items 7 to 13); Job satisfaction (items 15 to 19); Perception of stress (items 20 to 23); Perception of the management unit and of the hospital (items 24 to 29) and working conditions (items 30 to 32) and five items are not correlated to any domain, namely, item 14, It refers to the perception of the professional when you bring suggestions relating to patient safety and the items of between 33 to 36 directed the existing collaboration between the team and the failures in communication (12 .
The second part of the questionnaire is reserved for professional data and contains the padding information regarding position data, gender, acting principal and long experience in the specialty.
The answers to each of the questions follow the Likert scale, a scale of five points; for the purpose of assigning a numerical value to each of the responses issued by study subjects with five modes of answers: strongly disagree (A) equals 0 points; I disagree in part (B) equals 25 points; neutral (C) equals 50 points; I agree in part (D) is equal to 75 points; totally agree (and) is equal to 100 points and not apply identified with the letter "X" (9)(12)(13 .
Thus, the higher the score, the more positive the attitude, with the exception of items that feature reverse score (2, 11 and 36) where the lowest score indicates a more positive attitude (9)(12)(13 .
For descriptive analysis of responses to questionnaires completed two calculations were carried out: the first, the conversion of the answers as score set on Likert scale after inversion of the reverse items ("R"), and the second calculation intended to determine the average domains being held the sum of the scores assigned to each question in each of the corresponding domains.
From these values, the answers of each domain were summed and divided by the number of questions, resulting in a range of zero to 100, being considered a positive attitude when the result set was greater than or equal to 75 points demonstrating strong the professionals on the issues of security.
Thus, the questions were grouped by areas and finally calculated the sum of the answers to the questions in each domain and divided the result by the number of questions in each area.
Data were analyzed through simple statistical analysis, statistical treatment suffered software Microsoft ® Office Excel 2007 version being used a simple descriptive statistical analysis, with calculation of relative frequency, absolute and average frequency being built as a result of the aggregate indicators and stratification of the answers collected organized in tabbed Tables and charts in Excel.
RESULTS
Analysis of the envelopes returned in number corresponding to the amount reported for each functional area coordinator (14 envelopes for professionals in the hospital hygiene team, 17 envelopes for nursing professionals, 30 to reception/Administration), totaling the participation of 61 professionals.
It is worth mentioning that the doctors surgeons institution participated in this phase of the research, although included as participants for the implementation of the SAQ. Impossibilities portrayed by coordination of area, such as unwillingness to respond to the questionnaire items in front of the time to be discharged and incongruous items considered SAQ related area, it is not possible to deal with the surgeons, by setting a important limitation to the development of the study.
It is considered that doctor involvement; a critical part of change of culture in the operating room, where the absence of your active participation in daily life is characterized by insufficient decision-making, especially because this type of partnership can determine the promotion of adherence to this plan essentially Interdisciplinary care and safety (14 .
A total of 61 questionnaires which were delivered to health professionals FICS and SAQ in different areas of the institution 34 of them were excluded after return, because evidence of affirmative response rate less than 65% or even those who were fully "in White ".
It was only considered for analysis a total of 27 questionnaires answered, representing 55.7% of the total number of questionnaires with possibility of evaluation; composing a final sample of the study: (1) Auxiliary Nurse/nursing technicians (11); pharmacist (1), (4), environmental/sanitation service support (6), other (4) for the professional category doesn't discriminated against in the questionnaire.
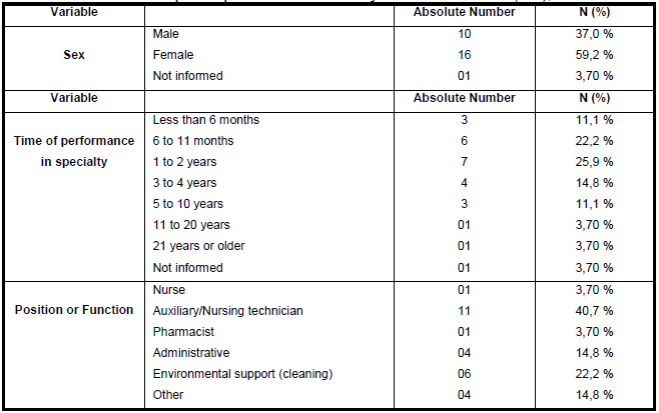
Table I Distributionof variables: Gender, Time of performance in specialty and title or function of the participants of the survey. Rio de Janeiro (RJ), 2017.
Source: results of own research. (Ribeiro, 2017)
Table I shows the socio demographic characteristics and functional study participants. From the analysis of the 27 questionnaires was evidenced higher prevalence of female professionals (59.2%); average time of performance of the professionals in the specialty configured within 6 months to 2 years (48.1%), 22.2% of 6 fence where the 11 months and 25.9% 1 to 2 years. In relation to the position or function performed, greater representation in the population group represented by assistants/nursing technicians (40.7%), followed by the employees of the environmental support service (Hospital cleaners) with 18.5%, administrative (14.8%) and other professionals categorized as "Other" (14.8%) corresponding to any category not entered in the questionnaire, for example: the pharmacy service helper.
Table II descriptive analysis of SAQ-Safety Attitudes Questionnaire

Source: results of own research. (Ribeiro, 2017)
In Table II , the descriptive analysis of the SAQ for your domains overall average 53.6 total valued pointed SAQ demonstrating concordance index less than 75 points.
As already mentioned in this study, it was considered only positive safety culture when the absolute number is represented by value equal to or greater than 75 points from the Likert scale.
The average scores of the SAQ, as well as the mean and median total for the score of the questionnaire for each domain and related items were evaluated separately according to Table II for better understanding of the scores for each item.
It can be observed that the attitude with highest average was represented in the field "job satisfaction" (74) followed by the "climate of teamwork" (68.9) and "security Climate" (67.8); obeying a descending order of value. There is no significant difference of value between these last two.
Smaller scores assigned to "Perception Management" related to the unit and to the hospital (41.1) followed by the domain on "Perception of stress" (53.3) and "working conditions" (57.6).
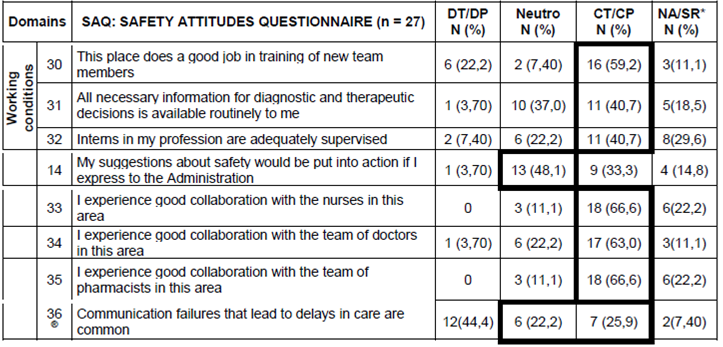
As author of the SAQ, items 14 and 33 to 36 do not belong to any specific domain, where the "14" item refers to the perception of the employee concerning the safety of the patient and the "the 33 35 items" related to collaboration between the health care team members and finally the "i has 36 " directed perception on the failures in communication (12 .
Descriptive analyses carried out for the sake of the domains of the SAQ, considering the options of answers: strongly disagree (DT) and partially disagree (DP) and the partially agree (CP) and totally agree (CT) grouped in order to obtain greater clarity on the statistics descriptive.
In the field for the "climate of teamwork", corresponding to the six items of the questionnaire, where correlates the quality of the relationship and collaboration between team members, can be showing average of 68.9 score as the level participants (Table II ). This made the second highest score among all other domains evaluated.
Table III Descriptive analysis by issue of SAQ - domain climate of teamwork, of health professionals operating in the municipality of ophthalmic hospital, Niterói, Rio de Janeiro, Brazil, 2017.

Source: results of own research. (Ribeiro, 2017)
In individualised analysis to items belonging to this domain (Table III ) can evaluate that 66.6% of the professionals agree completely and/or partially that the suggestions of the nurses are well accepted and in the work environment of mutual collaboration between the professionals team members in the care of the patient (81.4%) being easy dialogue and carry out questions on the desktop (81.4%). This aspect is highlighted in Table II showing the highest percentage index of all items represented in this field.
In the field "safety Climate", the average obtained does not show statistical significance with the previous domain where the result obtained an average score of 67.8 points (Table II ). Involves the evaluation of seven items on the perception of professionals about the commitment to patient safety.
The fact that both domains "climate of teamwork" and "security Climate present almost similar results can be explained when we perceive a certain convergence in some responses pointed out in both.
It can be observed that the participants have proven difficult to talk openly about issues that could involve the care, which in some ways, reveals some difficulty in creating a climate of security.
In descriptive analysis to the "safety Climate" (Table IV ) item 11 brings questionning "in this area, it is difficult to discuss about mistakes" and leads us to an important reflection when noted that more than half of the participants (51.8%) agree completely and/or partially be difficult to talk about mistakes though, 74% say being encouraged by colleagues to report any concerns related to patient safety.
Table IV Descriptive analysis by issue of SAQ: domain security Climate team of health professionals operating in the municipality of ophthalmic Hospital, Niterói, Rio de Janeiro, Brazil, 2017.

Source: Resultados da própria pesquisa. (Ribeiro, 2017).
However, in this same area, there is a counterpoint where participants report that they feel safe being treated in that institution as patients, demonstrating safety in the service provided to clients assisted, showing an index of agreement between the participants of 77.7%.
With respect to notification of adverse events, in item 9; "I know the appropriate means to address the issues related to patient safety in this area" showed that 70.3% of professionals recognize the internal means of notification of occurrences related to patient safety, where 77.7% believe that errors are treated in an appropriate manner.
The "job satisfaction" domain that depicts the positive view of the workplace under the perception of professionals presented the highest average score correlated to other domains.
Table V Descriptive analysis by issue of SAQ from the domain: Job satisfaction and Perception of stress, health professionals active in ophthalmologic hospital municipality of Niterói, Rio de Janeiro, Brazil, 2017.

Source: results of own research. (Ribeiro, 2017)
In the field "job satisfaction" you can analyze from the items that compose (Table V ), that most professionals replied "I agree completely (CT)" and/or "Partially Agree (CP)" featured issues; where the item "I like my job," presented the highest score (92.5%) followed by the item "I pride myself on working in this area" (70.3%).
Other items belonging to the domain could also reflect a positive view of the workplace where the issues concerning items 16 and 17 obtained 66.6% average score depicting the perception of professional satisfaction in working on site.
In respect of questions relating to the perception of professionals about the factors that can influence the job stressors, the responses indicated that 66.6% believe that the performance at work suffers when you feel tired, 40.7% opine that reflects tasks on decrease of efficiency in work and 44.4% cite agree completely and/or partially there is more likely to make mistakes in tense and hostile situations.
Table VI Descriptive analysis by issue of SAQ: perception management domain and the Hospital, health professionals active in the ophthalmic Hospital city of Niterói, Rio de Janeiro, Brazil, 2017

Source: results of own research. (Ribeiro, 2017)
The "unit management and perception of the hospital" security issues showed the lowest score of the SAQ (41.1%) according to Table II .
From the descriptive analysis of the items presented as Table VI , it was observed that most of the responses did not allow the realization of a global critical analysis, under the perception of professionals regarding the management of the unit and the hospital where the answers were evenly distributed and relatively expressive of professionals responded "neutral" or "not applicable/no answer" in most items of the questionnaire.
Featured in Table VI , 44.4% index points for the items dealing with questions relating to the understanding on the part of professionals in understanding that a good job is executed by the unit and manages the hospital, and on feedback regarding events that can afe tar the your work. However, this indicator reflects the perception the half of all the participants.
Concerning "working conditions" indicated a low awareness of the professionals on this field (57.6%) as indicated in Table II .
Table VII Descriptive analysis by issue of SAQ: domain working conditions and related items to the SAQ, health professionals active in ophthalmologic hospital municipality of Niterói, Rio de Janeiro, Brazil, 2017
Source: results of own research. (Ribeiro, 2017).
The item "This hospital do a good job in training new team members" points to the common sense that there is a concern in the institution with the training of new employees, however, with the need for improvement in this area.
Under review the items not belonging to any domain (Table II /Table VII ), can be found in the "Item 14" a high percentage of neutrality (48.1%) over the perception of the participants regardless of how suggestions on safety-related matters are considered by the Organization.
This index in the report to the "perception of manages the unit and the hospital" already discussed earlier, and which also showed a relation of neutrality the questions relating to the item.
33 to 35 items already indicate that the professionals believe there is a good perception of the professional relationship between nurses, doctors and pharmacists. The "item 36" presents the lowest average score (40) of the SAQ (Table II ) indicating weakness in the communication process. Nevertheless, in Table VI, only 25.9% of professionals agree completely and/or partially that communication failures that lead to delays in care are common.
DISCUSSION
The data submitted demonstrated low perception of the security climate in the perception of health professionals as the average score obtained in six areas of the SAQ; indicating that various aspects need to be improved.
Research on the use of the SAQ, in national and international contexts suggest that scores above 80 indicate strong consensus among climate safety professionals and those below 60 means a sign of alert to the institutions because indicate the need for implementation of safety culture (3 .
A study developed in the operating room of a Hospital in southern Brazil, between July and October of 2011 also has highlighted weaknesses in six areas, being observed that the areas most valued by professionals were: ' teamwork ' Climate, ' Working conditions ' and ' job satisfaction ', following the a descending order of value; the less relevant safety weather (4 .
This result resembled some other studies, for example, an accomplished in 2015 in the Hospital Base of the Distrito Federal (HBDF) ((3)) in assessing the perception of health professionals about the safety culture where showed that the total score of the SAQ ranged between 34.4 and 74.8 for d omínio averaging 53.3 indicating low perception of the culture of safety professionals; evidencing fragility in the values, attitudes, skills and behaviors that determine the safety culture in a healthcare organization.
The result evidenced from the items in the domain ' teamwork ' Climate brings us to the understanding that there's credibility of the role of nurses in quality assurance of assistance and the importance of the coordination of joint activities between the medical staff and of nursing.
Corroborating with that thought, says that to be a working climate conducive to both professional security as the patient, you must respect, harmony, consideration to the various opinions, collective interaction 8 .
On the other hand, in the same domain, in item 2, "in this area is difficult to talk openly if I get any problems with patient care", draws attention when examining the answers issued; realize that most professionals feel difficulty to treat a patient care related issues openly within the Organization, seen that 51.8% of participants agree total and/or partial feel difficulty to speak about a problem related to care.
A study carried out in the operating room of a hospital located in the southern region of Brazil, also found similar results noting the appreciation of the work of nurses by other professionals in recognition of their skills and potential. This factor is essential for the creation of a climate of work which should be based on the harmony of interpersonal relationships, in respect to the different opinions in the development of trust and of the collective work (4 .
In the field ' security ' Climate shows that professionals feel safety in the service provided to clients assisted, but from the other items that make up this domain, it is worth mentioning that the evidence that there is difficulty are talking openly about "mistakes" Although acknowledging that the institution has a policy established for event notification, examination and treatment of same.
In a similar study carried out with the same instrument was also evidenced in the field security climate that 80% of the participants shared the idea feel safe if treated in the unit as patients, 85.6% knew the appropriate means to address the issues related to patient safety and 82.2% answered that they were encouraged by colleagues to report any concerns regarding patient safety (8 .
In this context, it is believed that healthcare organizations should consolidate a paradigm shift of the safety culture where human errors can be analysed, where people may be able to create a culture of reporting of incidents, a learning culture where there is a balance between blame and accountability.
The domain ' job satisfaction ' presented the best score, evaluated as the most relevant by participants; presenting a favourable outcome of the safety culture. This result presents a direct relation with fewer adverse events (13 .
These results converge with other studies, where the item "job satisfaction" got the highest score, more relevant referenced by participants 3)(15)(16).
Job satisfaction is related to working conditions in the institutions, with the health of the worker, as well as team relations, which results in a more humane environment and better quality of care, which implies directly at best evolution Clinic patients. Can still be connected the appropriate conditions of work, professional remuneration, the power of efficaciousness and the optimisation of worker (17 .
The ' Perception of stress ' was recognized by participants as a factor that undermines the performance at work where factors related to fatigue and excessive journey of work translate into less efficiency and productivity.
Contribute to positive individual perception of professionals is to collaborate positively to your satisfaction, where maintaining a balance between the care provided and the employee caregiver is critical 8 .
Some authors believe that factors related to human resources may interfere with the development of a safe, being closely linked to the recognition of stress such as fatigue, the shortage of human resources, the barriers to communication, interpersonal relations, not the distractions, interruptions, errors of judgement, lack of attention and the emotional factor of the professionals (4 .
The ' Perception Management ' introduced index lower, indicating that research participants do not recognize the promotion of patient safety by their leaders, whether they are inserted in the unit or in the organization.
Corroborating with this analysis, a study in mid-sized private hospital of a municipality in Minas Gerais, using the SAQ measurement tool of the security climate, also highlighted the ' Perception Management ' with the worst average of 58.90 points and evaluates as be an indicator of professional dissatisfaction regarding management actions against security issues correlated this domain for approval of actions of management or administration, both the unit and the hospital as a whole (18 .
Among the items not related to any field, the item 14, reflects the perception of security from the perspective of professionals and your collaborative involvement with the organization. Although the average for the SAQ to item 14 (65.2) can see that the professionals have responded "neutral" (48.1%) for the response to the item, it is not possible to classify as a positive result.
The "33 to 35 items" related to the existing collaboration between the health care team members realize that she is present and finally the ' 36 ' item directed the perception on miscommunication where calls attention for demonstrating the lowest score obtained.
It is understood that communication is essential to the provision of a safe and effective assistance, being defined as one of the objectives of the proposal from the World Health Organization (who) in its guidelines laid out in the manual of surgical safety by setting the need to establish an effective communication and information exchange between the team for conducting a safe surgical procedure.
In the context of safe surgical assistance, the use of the surgical safety checklist is an important tool for improving communication and patient safety at transoperatório. When on your incorporation to recognize broader aspects of the institutional-political influence in this process by health services, namely: management, leadership, planning, education, audit and feedback to the team of surgical Center (14 .
A study of reflection carried out about patient safety and mounting process of operating room nurse's attention to the multifaceted look of perioperative period that involves a combination of decision making and brings relevant factors to be considered: as the competence of the team, the technical skill of the surgical team, the satisfactory performance of the team and effective communication between these professionals as proposal for improving patient-focused care (19 .
In relation to ' working conditions ' was analyzed that there should be a plan for improvements vis-à-vis the quality of working environment whereas the result points to an average 57.6. In other research was also found scores ranging from 40 to 65 18)(10 .
CONCLUSION
Through the analysis of the domains of the SAQ has become possible to assess the perception of safety climate, where the results revealed a panorama of fragility in all six areas assessed, indicating the need for improvement and changes in the organization.
The recognition of the security climate stands out as a priority measure for sustaining actions directed to effective practice of surgical safety where the study indicates need for attention of high lead in the adoption of an integrated activities that support the initiatives the implementation of evidence-based safe practices and to promote the engagement of all healthcare professionals in attention to these actions.
REFERENCIAS
1. La Organización Mundial de la Salud. Segundo reto de seguridad global del paciente: la cirugía segura salva vidas. Rio de Janeiro: 2009. 211 p. disponible en: http://bvsms.saude.gov.br/bvs/publicacoes/seguranca_paciente_cirurgia_salva_manual.pdf. [ Links ]
2. Moura MLO, Mendes w. evaluación de los eventos adversos quirúrgicos en los hospitales de Río de Janeiro. Brasil. Epidemiol Rev Bras [revista en línea] Febrero 2012 [2016 acceso 30 de octubre], 15, (3), p. 523-35 disponible en: http://www.scielosp.org/pdf/rbepid/v15n3/07.pdf. [ Links ]
3. CH PA, Göttems, MRGM, Oliveira Pires LBD MLC. Cultura de seguridad en un hospital público, en la percepción de los profesionales de la salud. Reverendo Latina AM Nursing. [revista en línea] 2015 Nov-Dic [2016 acceso 15 de septiembre]; 23 (6): 1041-8. Disponible en: http://www.scielo.br/pdf/rlae/v23n6/pt_0104-1169-rlae-23-06-01041.pdf [ Links ]
4. . TC da Correggio, LN, Barbosa SFF. Evaluación de la cultura de seguridad en una quirúrgica. São Paulo. Reverendo SOBECC. [revista en línea] 2014 Abr-Jun [2016 acceso 30 de octubre], 19 (2) 67-73 p. Disponible en: http://www.sobecc.org.br/arquivos/artigos/2015/pdfs/site_sobecc_v19n2/02_sobecc_v19n2.pdf. [ Links ]
5. Corona ARPD, Peniche ACG. La cultura de seguridad del paciente en la adhesión al Protocolo de cirugía segura. São Paulo. Reverendo SOBECC. [revista en línea] 2015 Jul/Set. [01 de enero del acceso de 2016]; 20 (3): 179-185. Disponible en: http://files.bvs.br/upload/S/1414-4425/2015/v20n3/a5210.pdf. [ Links ]
6. Ministerio de salud (Brasil). Ordenanza Nº 529, 01 de abril de 2013. EsTablece la seguridad del paciente nacional programa. Brasilia, 2013. [ Links ]
7. DCDA Lourenção; Necker debió ser DMR. Seguridad del paciente en el ambiente quirúrgico: traducción y adaptación cultural de instrumentos validados. ACTA Paulista de enfermeras. [revista en línea] enero-febrero de 2016 [acceso en 2016 10.20] 29 (1): 1-8. Disponible en: http://dx.doi.org/10.1590/1982-0194201600002. [ Links ]
8. Toso GL, L Golle, TSBS Magnago, et al. Cultura de segurança do paciente em instituições hospitalares na perspectiva da enfermagem. Revista Gaúcha de Enferm. [periódico en línea] 2016 Dez. 15 [acesso em 2016 Dez. 21] 37(4). Disponível em: http://dx.doi.org/10.1590/1983-1447.2016.04.58662. [ Links ]
9. Sacristán J, Helmreich R, T Neilands, Rowan K, K Vella, Boyden J, et al. El cuestionario de actitudes de seguridad: propiedades psicométricas, evaluación comparativa datos e investigación emergente. BMC Health Serv Res. [periódico en línea] 3 de abril de 2006 [acesso em: 2016 conjunto. 12] 6(44): 1-10. Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/16584553. [ Links ]
10. Rigobello. MCG; Roble. REFL; Cassiani. BHS; seguridad del paciente et al clima: percepción de los profesionales de enfermería. Acta Paul. personal de enfermería. [revista en línea] febrero de 2012. 08 [acceso en 2016 10.28] 25 (5): 728-35. Disponible en: http://dx.doi.org/10.1590/S0103-21002012000500013 [ Links ]
11. REFL CH; Cassiani SHB. Cuestionario de actitudes de seguridad: adaptación transcultural de la seguridad actitudes cuestionario corto formulario 2006 para Brasil. Reverendo Latina AM Nursing. [revista en línea] Mai 2012-Jun [acceso: 2016 conjunto. 12] 20 (3): [8 pantallas]. Disponible en: http://www.scielo.br/pdf/rlae/v20n3/pt_a20v20n3.pdf. [ Links ]
12. CH REFL. adaptación transcultural del cuestionario de actitudes de seguridad para Brasil - Cuestionario de actitudes de seguridad. Ribeirão Preto. Tesis [doctor en enfermería]-Universidad de São Paulo, Ribeirão Preto enfermería escuela; 2011. [ Links ]
13. Cauduro, FLF. Evaluación de la cultura de seguridad en unidades quirúrgicas. Tesis doctoral [programa de posgrado en enfermería]-sector de Ciencias de la salud. Universidad Federal de Paraná. Curitiba, 2013. [ Links ]
14. Tostes MFP; Haracemiw A; Checklist de seguridad quirúrgica ld. Mai: consideraciones desde la micropolítica. ESC. Anna Nery [revista en línea] ene 2016-Mar [consultado: 2016 10.28] 20 (1): 203-209. Disponible en: http://www.scielo.br/pdf/ean/v20n1/1414-8145-ean-20-01-0203.pdf. [ Links ]
15. Fidelis RE. Cultura de seguridad: perspectiva de personal en el adulto de emergencia de enfermería. Tesis [profesional master en gestión de cuidados de enfermería]-Universidad Federal de Santa Catarina, Florianópolis; 2011. [ Links ]
16. Mm. de enfermería cuidado de Marina y la cultura de seguridad del paciente: un estudio evaluativo en las unidades de admisión quirúrgica. Tesis doctoral [programa de posgrado en enfermería]. Universidad Federal de Santa Catarina, Florianópolis 2012. [ Links ]
17. Vegro TC, roca FLR, camello, AB. Garcia cultura organizacional de un hospital privado. Revista de enfermera de gaucho. [revista en línea] junio de 2016 [acceso en 2016 10.28] 37 (2): 1-6. Disponible en: http://www.scielo.br/pdf/rgenf/v37n2/0102-6933-rgenf-1983-144720160249776.pdf. [ Links ]
18. Barbosa MH, el Dr. Fox, Oliveira 2KF, KG de nacimiento, Fernández Ángeles. Clima de seguridad del paciente en un hospital privado. Texto contexto-enfermeras. [revista en línea]. 2016 Sep. 12, [consultado el 22 de abril de 2017] 25 (3). Disponible en: http://dx.doi.org/10.1590/0104-07072016001460015. [ Links ]
19. SOY de Lima, Souza CS, cuña ALSM. Seguridad del paciente y sala de operaciones: estudio de la reflexión. Revista de enfermería: Rev Enfem UFPE [revista en línea] Ene de 2013, [acceso en 2016 10.12] 7 (1): 289-94. Disponible en: http://www.revista.ufpe.br/revistaenfermagem/index.php/revista/article/viewFile/4047/pdf_1923. [ Links ]
Received: May 23, 2017; Accepted: November 23, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
