










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.18 no.55 Murcia jul. 2019 Epub 21-Oct-2019
https://dx.doi.org/10.6018/eglobal.18.3.324401
Originals
Factors associated with depression in older adults over the age of 75 living in an urban area
1Nursing Department. University Jaume I. Castellón de la Plana.Spain. mjulio@uji.es
2Department of Health. Castellón de la Plana. Spain.
3Provincial Hospital Consortium of Castellón. Castellón de la Plana. Spain
Introduction
Depression in older adults is a major health problem, and it is considered the most common psychiatric disorder among this population in developing countries. It is associated with suffering and increased prevalence and poor evolution of health problems. The aim of the present study was to determine the prevalence of depression and related factors in people over the age of 75 years in the city of Castellón de la Plana, Spain.
Methodology
This was an observational, cross-sectional, and analytical study in which a questionnaire was administered to a sample of 400 community-dwelling older adults over the age of 75 and who were selected using purposive sampling in 2015.
Results
the overall prevalence of depression symptoms was 30.5%, a percentage higher among women (40.1%). Older adults living alone presented more symptoms of depression, 26.6% compared with 16.1% (p = 0.011). Good self-perceived health was related to fewer depression symptoms. Non-frail individuals presented lower rates of depression symptoms (12.1%) than frail (30.8%), and pre-frail individuals (57%) p<0.05. Negative aspects in social relationships showed a lower mean score (0.003) in individuals without depression symptoms (p = 0.006).
Conclusions
There is a link between the presence of depression symptoms and gender, self-perceived health, living condition, and frailty.
Key words: Depression; Older adults; Frail older adults; Risk factors
INTRODUCTION
Aging is influenced not only by biopsychosocial changes, but also by other multidimensional contexts, such as financial status, lifestyle, personal achievement, illnesses, accumulated suffering, and genetic factors.1
The concept of depression includes the presence of affective, cognitive, volitional, and somatic symptoms that mainly affect the emotional domain.2,3 Depression manifests in the older adult population in various ways: as a recurring illness from before old age, recent onset as a mental disorder secondary to a general medical condition, or as a secondary symptom associated by the use of medications. Similar to what occurs in other age groups, depression probably stems from a complex multidirectional interaction of biological, psychological (including personality), and social factors.4 A diagnosis of depression is based on observed data and the symptoms reported by patients, based on the International Statistical Classification of Diseases and Related Health Problems (ICD) and the American Psychiatric Association (DSM) criteria. Even though several population-based studies identify depression symptoms using screening scales, the Center for Epidemiological Studies Depression Scale (CES-D)5,6 is the most used instrument.
Depression in older adults is a major health issue and is considered the most common psychiatric disorder among this population in developed countries, associated with suffering and increased prevalence and poor evolution of health problems.7 The prevalence of depression in older adults is 13.5% worldwide.8 However, in a European study carried out with community-dwelling older adults, this percentage was 12.3%,9 whereas in Spain, it was 14%.10 The prevalence of major depression (recurrent episodes) in community-dwelling older adults is between 1 and 5%.11
Some factors specific to depression in older adults have been identified, such as comorbidity, neurological disorders, psychosocial factors, social support, and life stressors.12 Learning more about the factors associated with this pathology can help outline actions that aim to improve the health of older adults.
The objective of this study was to determine the prevalence of depression and factors associated with older adults over the age of 75 years in the city of Castellón de la Plana, Spain.
METHODOLOGY
Study design, location, and period
This was an observational, cross-sectional, and analytical study carried out in the city of Castellón de la Plana, Spain, throughout 2015, using individual interviews to administer the Fralle survey.13
Population and sampling. Inclusion and exclusion criteria
The population consisted of community-dwelling individuals over the age of 75 years (12,711 individuals). Inclusion criteria were older adults of both genders, who lived in family households, had healthcare cards, and who agreed to participate in the study, and individuals who presented cognitive impairments and had caregivers (in this case, the respondents were not asked questions about subjective data).
Terminally ill individuals, receiving institutional care, who presented cognitive impairments and did not have caregivers, and those who did not want to participate in the study were excluded.
The sample size was determined using a 95% confidence level and 5% accuracy, with significance set at p=0.5, resulting in a sample of n=373. Anticipating a nonresponse rate of 10% (survey errors or individuals who did not show up to the interview), the sample size was set as n=414. Purposive sampling was carried out over the year of 2015, and consisted of primary care team nurses conducting interviews with individuals during their appointments or by phone. Finally, a sample n=400 was obtained with individuals who visited seven out of nine of the department’s healthcare centers. This Figure, along with the distribution of the sociodemographic characteristics of the centers in which the individuals participated, ensured the representativeness of the sample.
Study protocol
As previously mentioned, data was collected by administering the Fralle survey13 designed on the basis of validated questionnaires for a study about non-institutionalized older adult population in Lleida, Spain. This sample consists of a series of questions distributed in 9 dimensions, measuring social relationships, self-perceived health, general health, and depression symptoms, among other factors.
Target study variables
Dependent variable
Presence of depression symptoms, measured by the Center for Epidemiologic Studies Depression Scale (CES-D)5 scale, which consists of 20 questions and investigates cognitive and behavioral components of depression symptoms in the population. Score ranges from 0 to 60, and higher scores indicate depression symptoms: scores ≥ 16 are associated with depression disorder.
Independent variables
Sociodemographic variables: living condition, monthly income, level of education, and gender. Living condition was measured using two items: “alone”, for people living alone in their home, and “with a partner”. Monthly income consisted of two categories, <900 euros and >900 euros per month, along with an option for nonresponse. Level of education was measured using the items “Cannot read or write”, “Did not finish elementary school”, “Complete elementary school”, “Complete junior high school”, “High school”, and “Higher education”, which was later categorized as “No formal education” (Cannot read or write or Did not finish elementary school) or “Formal education” (Complete elementary school, Junior high school, High school, or Upper education).
Self-perceived health was measured based on a question about general perceived health with five answer options: excellent, very good, good, regular or poor; after the interview, these categories become two: either good (including positive options: excellent, very good, good) or poor (including options for negative answers: regular or poor).
Frailty was defined according to the criteria set forth by Fried et al14: unintentional weight loss, grip strength, exhaustion, walk time, and low level of physical activity. Individuals are considered “frail” when three or more frailty criteria are met; “intermediate”, one or two criteria; and “not frail” when no criteria are met.
Social relationships were measured using the questionnaire “Aging in Leganés”, designed and adapted to the Spanish population in a study conducted in Leganés, according to the conceptual model created by Berkman and Glass.15 Information about the structure of the participants’ social network structure and psychosocial mechanisms involved in social networks were obtained.16 Drawing from the questions on social relationships, the following variables were formulated:
Social networks:
Rate of family ties with contact (score range 0-3)
Rate of community activities (score range 0-4)
Rate of network diversity: including the two rates above and contact with friends (score range 0-8)
Psychosocial mechanisms of social relationships:
Rate of received emotional support (mean score obtained from the emotional support scales from four family ties)
Rate of individual’s role (mean score obtained from the scales of the individual’s role in the life of friends and family ties).
Rate of negative aspects (score mean obtained from the scales of negative aspects for each one of the children, extended family, friends, and partner ties).
Ethical considerations
Prior to the study, the authors obtained permission from the Fralle Survey to replicate the study in the city of Castellón. The Clinical Research Ethics Commission of the health department of Castellón approved the study project, and the participants signed informed consent forms. Data confidentiality was upheld at all times, in accordance with current legislation.
Data analysis
Statistical descriptive analysis was carried out with central tendency measures and percentage rates.
Bivariate analysis of the factors associated with depression, was conducted using Pearson’s Chi-square for qualitative analysis and Student’s T-test for quantitative analysis; significance level was set at p<0.05.
Nonresponse (when any of the survey questions were not answered or the person presented cognitive impairment) was calculated as recommended by Demaio17, considering that nonresponse rates lower than 10% allow for inference based on available cases. Allocation was not used in the analysis.
To assess the impact of several factors on depression symptoms, logistic regression analysis was carried out. Different models of logistic regression were designed, introducing the control variables one-by-one: the first model was designed based only on gender; the second model included living conditions; and the third model, health condition and social relationships. Data analysis was conducted with the help of the SPSS Statistics program, version 2.0.
RESULTS
A total of 400 individuals were interviewed, with a mean age of 81.29 ranging from 75 to 96 years of age, of which 46.8% were male and 53.2% were female.
Descriptive analysis by gender (Table 1) showed that 30.5% of the individuals presented depression symptoms, with women presenting higher rates (40.1%) than men (19.7%). Most 78.2% individuals had partners, but among women, this percentage was lower (68.7%) than men (88.9%). Regarding level of education, 51.8% of the individuals did not have a high school education.
In terms of income, 41.5% of the older adults earned less than 900 euros monthly, and among women this rate was higher.
Self-perceived health was considered good by 62.9% of the sample. Women perceived their general health as good less often than men: 55.5% compared with 71.4%.
On comparing frailty by gender, 23.2% of the sample self-reported as frail, wherein women presented higher rates than men: 28% compared with 18%.
Table 1. Sample characteristics by gender: count (n) and percentage (%)
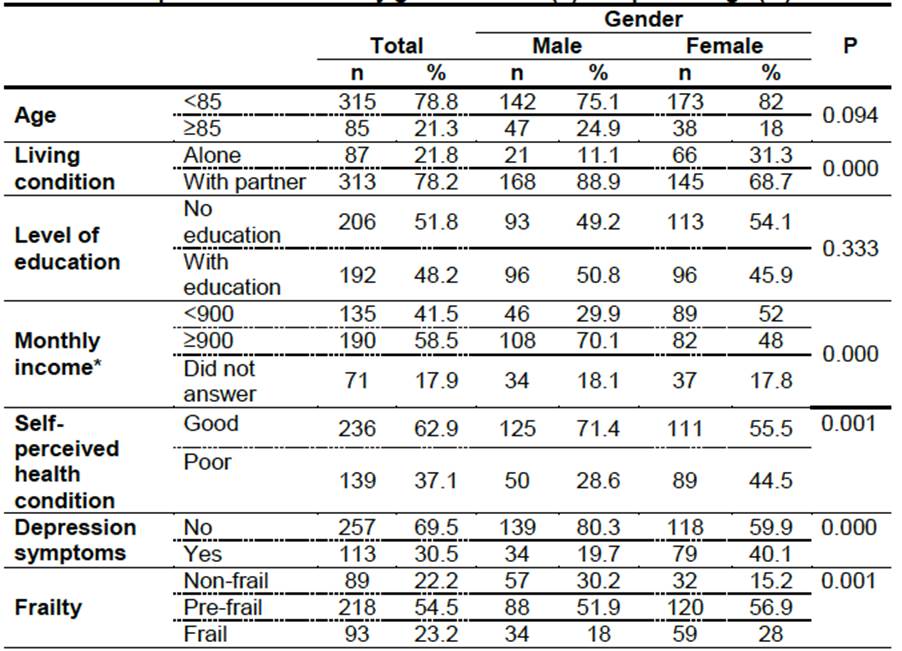
Note: *NDue to the level of nonresponse for this variable (see Demaio 1980), the inferred values may not represent the population’s characteristics.
Bivariate analysis of the association of depression symptoms with the studied variables (Table 2), showed that, in terms of age, there were no statistically significant differences between individuals under the age of 85 years and 85 years old or older.
Statistically significant differences (p=0.011) were found related to living conditions: older adults living alone showed more depression symptoms than those living with a partner: 26.6% compared with 16.1%.
Table 2. Depression symptoms according to study variables: count (n) and percentage (%)
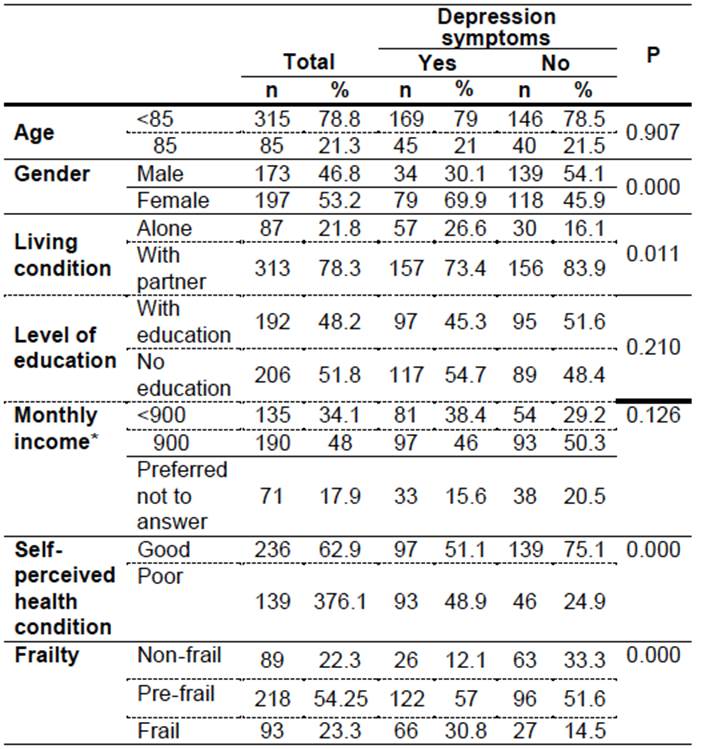
Note: *Due to the level of no answer for this variable (see Demaio 1980) the inferred values may not be representative of the population characteristics.
No statistically significant differences were found between the presence of depression symptoms and monthly income; the same was true for level of education.
Conversely, regarding self-perceived health, individuals who self-reported good health conditions did not present depression symptoms at higher rates (75.1%) than those who perceived their health as poor (24.9%) (p=0.000).
Regarding frailty, non-frail individuals presented less depression symptoms (12.1%) than intermediate (57%) and frail individuals (30.8%) (p=0.000).
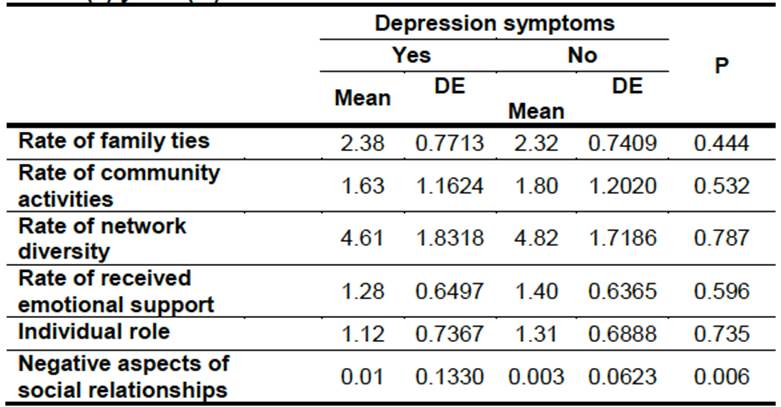
An analysis of the participants’ social relationships (Table 3) shows that there were no significant differences in the rates of family ties, community activities, network diversity, and received emotional support; however, mean scores were lower among individuals who presented more depression symptoms. Considering only the negative aspects of social relationships, the mean score was significantly (p=0.006) higher among individuals with depression symptoms.
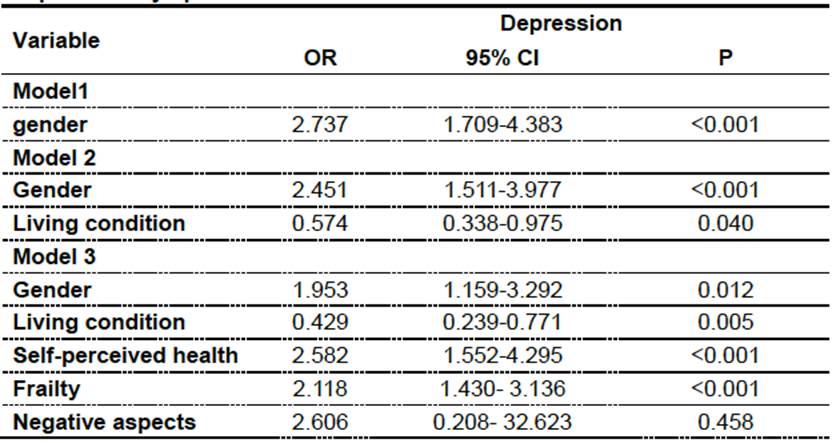
As for binary logistic regression analysis, which assessed the possibility of presenting depression (Table 4), the variables that presented statistical significance in bivariate analysis were introduced one by one: gender, living condition, frailty, self-perceived health, and negative aspects of social relationships. Gender (female) was statistically significant in the three models, with women presenting almost double the risk of men of being affected by depression (OR: 1.953; CI: 1.159-3.292). Additionally, living condition also presented a significant association with depression: Individuals living with partners showed lower risk of suffering depression symptoms (OR: 0.429; CI: 0.239-0.771). Negative self-perceived health was associated with a higher risk of presenting depression symptoms (OR: 2.582; CI: 1.552-4.295). Frailty was positively associated with depression symptoms, in which frail older adults presented twice the risk of suffering from depression symptoms (OR: 2.118; CI: 1.430-3.136). There was no link between the negative aspects of social relationships and depression symptoms.
DISCUSSION
The prevalence of depression estimated in different studies varies considerably. The Figures obtained in the current work (30.5%) are very similar to those presented in the study conducted in Lleida18 applying the same methodology. However, the results are lower than those obtained in the works of Sánchez-García et al 19 and Estrada et al.20, which used the CES-D-R (modified CES-D scoring) as a measuring tool (56.8% and 47.6% respectively). This may be because the modified CES-D scoring method has proved to be more sensitive in identifying depression symptoms among the older adult population.19Variability in the prevalence of depression may be due to the fact that the researchers did not perform a screening test first, followed by diagnostic confirmation.21
In the current study, differences between gender were observed with more depression symptoms occurring in women, data that coincide with the findings of other studies,18,19,22 and can be related to social and cultural factors. In contrast, some authors claim that differences in the prevalence of depression between men and women decrease with age, as shown by a study by Urbina et al.23.
Regarding age, no significant differences were found in the Castellón sample, in contrast to the findings of studies with populations of Valle (Mexico), and Moscow.7,19,24 A possible explanation is that there were very few older adults 85 years old or older in the Castellón sample.
Regarding living condition, significant differences were observed among older adults living alone, who presented more symptoms of depression. This agrees with the studies of Zavala-González7, Domínguez-Sosa25, Escobar et al.18 and Ferreira & Tavares.26 Contrary to the results of the present study, Acosta & García27 found no significant differences in terms of living conditions, perhaps because they included a broader age group.
The perceived monthly income was not related with depression symptoms, although these results may be taken with caution, since the percentage of losses in the question is high, especially taking into account that, in the consulted literature, a relationship between the economic factor and depression was observed.7,18
Positive self-perceived health was associated with lower prevalence of depression,20 in agreement with the results of the current study. Considering that positive health perception is linked to a better physical health condition, the present results are in accordance with those obtained by Escobar et al,18 and Kronfly Carlos-Gil et al.28
Differences were found in the frailty of participants, in that the frail and intermediate individuals were associated with the presence of depression symptoms, a finding that coincides with the works of Díaz de León et al29 and Carlos-Gil et al.30 This relationship may be explained by the increased vulnerability of frail and intermediate older adults when faced with stressful situations.31
Regarding social relationships among the Castellón population, significant differences were found regarding negative perceptions of their friends and family ties. The results are in accordance with those of Ferlander et al.24 and Marroquin & Nolen-Hoeksema.32 Along the same lines, Zavala et al.7 described a link between poor family ties and higher risk of depression. However, in the current study, this variable did not present predictive value.
The results of the present study confirm that being a woman, having positive self-perceived health, and frailty were strongly associated with the presence of symptoms of depression, similar to other studies.33,34 The negative aspects of social relationships did not present a significant association, even though it is presented by the literature as a predictor variable,35,36 and this can be an effect of the good family support networks presented by the sample of the current study.
Limitations of the present study include data loss from the participants who presented cognitive impairments and did not answer the survey’s subjective questions. Furthermore, purposive sampling is subject to the willingness of the healthcare centers to participate in the study and may have impacted the results. Last, the cross-sectional design of this work prevents the researchers from establishing casual relationships.
CONCLUSIONS
The results point to a relationship between the presence of depression symptoms and the female gender, negative self-perceived health, frailty, and living alone, in agreement with most of the bivariate analysis results.
The prevalence of depression symptoms was high. Related factors were gender, with higher rates among women; living condition, with higher rates among older adults living alone; and frailty.
The high prevalence of depression symptoms in the study population justifies the need to design interventions aimed at this issue. Efficient actions should focus on aspects associated with the presence of depression symptoms and propose new lines of longitudinal studies.
REFERENCIAS
1. Dabove Caramuto MI, Prunotto Laborde A, Barnett V. Derecho de la ancianidad?: perspectiva interdisciplinaria. Editorial Juris; 2006. 324 p. [ Links ]
2. Grupo de trabajo de la Guía de Práctica Clínica sobre el Manejo de la Depresión en el Adulto. Guía de Práctica Clínica sobre el Manejo de la Depresión en el Adulto. Servicios Sociales e Igualdad. Agencia de Evaluación de Tecnologías Sanitarias de Galicia; 2014. p. 264. [ Links ]
3. National Collaborating Centre for Mental Health. Depression: The Treatment and Management of Depression in Adults (Updated Edition). British Psychological Society. 2010. [ Links ]
4. Toro R, Vargas J, Murcia S, Galtán N, Umbarlla D, Sarmlento K. Depresión mayor en la adultez tardía: Factores causales y orientaciones para el tratamiento. Rev Vanguard Psicológica Clínica Teórica y Práctica-. 2014;4(2):147-53. [ Links ]
5. Radloff LS. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl Psychol Meas. 1977 Jun;1(3):385-401. [ Links ]
6. Eaton W, Muntaner C, Smith C. Revision of the Center for Epidemilogic Studies Depression (CES-D) Scale Baltimore: Johns Hopkins University. Prev Cent. 1998; [ Links ]
7. Vilagut G, Forero CG, Barbaglia G, Alonso J. Screening for Depression in the General Population with the Center for Epidemiologic Studies Depression (CES-D): A Systematic Review with Meta-Analysis. van der Feltz-Cornelis C, editor. PLoS One [Internet]. 2016 May 16 [cited 2018 Jul 30];11(5):e0155431. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27182821 [ Links ]
8. Zavala G, Núñez L, Chavarría R, Ochoa L, Suazo N, Morales R, et al. Depresión en adultos de 60 a 75 años en San Lorenzo, Valle, Marzo2011. Rev Fac Cienc Méd. 2011;8(2):9-22. [ Links ]
9. Barua A, Ghosh M, Kar N, Basilio M. Distribution of depressive disorders in the elderly. J Neurosci Rural Pract [Internet]. 2010 Jul [cited 2018 Jul 30];1(2):67-73. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21808506 [ Links ]
10. Copeland JRM, Beekman ATF, Braam AW, Dewey ME, Delespaul P, Fuhrer R, et al. Depression among older people in Europe: the EURODEP studies. World psychiatry. 2004 Feb;3(1):45-9. [ Links ]
11. Hasen T, Slagsvold B. The eas-guest divide in late-life depression in europe: resulted from the generations and gender survey. Scand psycologits. 2017;4(e4). [ Links ]
12. Sarró-Maluquer M, Ferrer-Feliu A, Rando-Matos Y, Formiga F, Rojas-Farreras S. Depresión en ancianos: prevalencia y factores asociados. Semergen. 2013;39(7):354-60. [ Links ]
13. Fiske A, Wetherell JL, Gatz M. Depression in older adults. Annu Rev Clin Psychol [Internet]. 2009 [cited 2018 Jan 11];5:363-89. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19327033 [ Links ]
14. Alvarado Garcia A, Salazar Maya A. Análisis del concepto de envejecimiento. Gerokomos. 2014;25(6):57-62. [ Links ]
15. Jürschik P, Nunin C, Botigué T, Escobar M, Lavedán A, Viladrosa M. Prevalence of frailty and factors associated with frailty in the elderly population of Lleida, Spain: the FRALLE survey. Arch Gerontol Geriatr. 2012;55(3):625-31. [ Links ]
16. Fried L, Tangen C, Walston J, Newman A, Hirsch C, Gottdiener J, et al. Frailty in older adults evidence for a phenotype. Journals Gerontol Ser A Biol Sci Med Sci. 2001;56(3):M146-57. [ Links ]
17. Berkman L, Glass T. Social integration, social networks, social support and health. In: Social epidemiology New Yor. 2000. p. 137-73. [ Links ]
18. Rodríguez Laso A. El efecto de las relaciones sociales sobre la mortalidad en las personas mayores: el estudio envejecer en Leganés. Universidad Autónoma de Madrid; 2004. [ Links ]
19. DeMaio TJ. Refusals: Who, Where and Why. Public Opin Q. 1980 Jan 1;44(2):223. [ Links ]
20. Escobar Bravo MÁ, Botigué Satorra T, Jürschik Giménez P, Nuin Orrio C, Blanco Blanco J. Sintomatología depresiva en ancianos. La influencia del género. Rev Esp Geriatr Gerontol. 2013 Mar;48(2):59-64. [ Links ]
21. Sánchez-García S, Juárez-Cedillo T, Gallegos-Carrillo K, Gallo JJ, Wagner FA, García-Peña C. Frecuencia de los síntomas depresivos entre adultos mayores de la Ciudad de México. Salud Ment. 2012;35(1):71-7. [ Links ]
22. Estrada Restrepo Alejandro, Cardona Arango Doris, Ángela María Segura Cardona, Jaime Ordóñez Molina, Jorge Julián Osorio Gómez, Lina Marcela Chavarriaga Maya. Síntomas depresivos en adultos mayores institucionalizados y factores asociados * Depressive Symptoms in Institutionalized Elderly People and Factors Associated. 2013 [cited 2017 Sep 8];12(1):1657-9267. Available from: https://www.cop-cv.org/db/docu/130715110112ILbs6w6tcQYj.pdf [ Links ]
23. Kok R, Avendano M, Bago d'Uva T, Mackenbach J. Can Reporting Heterogeneity Explain Differences in Depressive Symptoms Across Europe? Soc Indic Res [Internet]. 2012 Jan 15 [cited 2018 Jul 30];105(2):191-210. Available from:http://link.springer.com/10.1007/s11205-011-9877-7 [ Links ]
24. Li N, Chen G, Zeng P, Pang J, Gong H, Han Y, et al. Prevalence of depression and its associated factors among Chinese elderly people: A comparison study between community-based population and hospitalized population. Psychiatry Res. 2016 Sep 30;243:87-91. [ Links ]
25. Urbina Torija JR, Flores Mayor JM, García Salazar MP, Torres Buisán L, Torrubias Fernández RM. Síntomas depresivos en personas mayores. Prevalencia y factores asociados. Gac Sanit. 2007;21(1):37-42. [ Links ]
26. Ferlander S, Stickley A, Kislytsyna O, Jukkala T, Carlso P, Mäkinen I. Capital social ¿ Una bendición mixta para las mujeres? un estudio transversal de las diferentes formas de las relaciones sociales y la auto-evaluacion de la depresion en Moscú. BMC psiyhol. 2016;4(37):1-23. [ Links ]
27. Zavala-González M, Domínguez-Sosa G. Depresión y percepción de la funcionalidad familiar en adultos mayores urbanos mexicanos. Psicogeriatría. 2010;2(1):41-8. [ Links ]
28. Ferreira PC dos S, Tavares DM dos S. Prevalência e fatores associados ao indicativo de depressão entre idosos residentes na zona rural. Rev da Esc Enferm da USP. 2013 Apr;47(2):401-7. [ Links ]
29. Acosta Quiroz CO, Garcias Flores R. Ansiedad y depresión en adultos mayores. Psicol y salud. 2007;17(2):291-300. [ Links ]
30. Kronfly E, Rivilla Frías D, Ortega Abarca I, Villanueva Villanueva M, Beltrán Martínez E, Cornellas Villalba M, et al. Riesgo de depresión en personas de 75 años o más, valoración geriátrica integral y factores de vulnerabilidad asociados en Atención Primaria. Atención primaria Publicación Of la Soc Española Fam y Comunitaria, ISSN 0212-6567, Vol 47, No 10, 2015, págs 616-625. 2015;47(10):616-25. [ Links ]
31. Diaz de León E, Tamez H, Gutiérez H, Cedillo J, Torres G. Fragilidad y su asociación con mortalidad, hospitalizaciones y dependencia funcional en mexicanos de 60 años o más. Med Clin (Barc). 2012 Apr 28;138(11):468-74. [ Links ]
32. Carlos-Gil AM, Martínez-Pecino F, Molina-Linde JM, Villegas-Portero R, Romero-Tabares A, Aguilar-García J, et al. Predictores de fragilidad en el anciano. Rev multidiscip gerontol. 2011;21(2):67-73. [ Links ]
33. Sousa Pegorar M, dos Santos Tavares D. factores asociados al sindrome de fragilidad en ancianos residentes en area urbana. Rev Latino-Am Enferm. 2014;22(5):874-82. [ Links ]
34. Marroquin B, Nolen-Hoksema S. Regulación emocional y síntomas depresivos: relaciones cercanas y contexto social. J Pers Soc Psychol. 2015;109(5):836-55. [ Links ]
35. Soysal P, Veronese N, Thompson T, Kahl KG, Fernandes BS, Prina AM, et al. Relationship between depression and frailty in older adults: A systematic review and meta-analysis. Ageing Res Rev. 2017 Jul;36:78-87. [ Links ]
36. Lino VTS, Portela MC, Camacho LAB, Atie S, Lima MJB. Assessment of Social Support and Its Association to Depression, Self-Perceived Health and Chronic Diseases in Elderly Individuals Residing in an Area of Poverty and Social Vulnerability in Rio de Janeiro City, Brazil. LoGerfo J, editor. PLoS One. 2013 Aug 12;8(8):e71712. [ Links ]
37. Ferlander S, Stickley A, Kislitsyna O, Jukkala T, Carlson P, Mäkinen IH. Social capital - a mixed blessing for women? A cross-sectional study of different forms of social relations and self-rated depression in Moscow. BMC Psychol. 2016 Dec 22;4(1):37. [ Links ]
38. Marroquín B, Nolen-Hoeksema S. Emotion regulation and depressive symptoms: Close relationships as social context and influence. J Pers Soc Psychol. 2015 Nov;109(5):836-55. [ Links ]
Received: March 12, 2018; Accepted: July 30, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
