










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.18 no.55 Murcia jul. 2019 Epub 21-Oct-2019
https://dx.doi.org/10.6018/eglobal.18.3.344971
Originals
Quality management in pre-natal care: urinary infections care in a municipality of the Legal Amazon
1PhD student of the Post-graduation Program in Nursing of Universidade Federal de Pelotas - UFPEL - Brazil. cecagno@gmail.com
2Associate Professor of Public Health Department of Universidade Federal do Rio Grande do Norte – UFRN– Brazil.
3Adjunct Professor of Hospital Department of Nursing School at Universidade Federal de Pelotas – UFPEL – Brazil.
4Adjunct Professor of Public Health Department of Universidade Federal do Rio Grande do Norte – UFRN – Brazil.
5Adjunct Professor of Public Health Department of Nursing School at Universidade Federal de Pelotas – UFPEL - Brazil.
Objective
To evaluate the effects of a quality improvement cycle in the prevention and management of UTI during pre-natal.
Methodology
This is a quantitative study with partly completed experimental design type before and after, with no control group, carried out in Cacoal/RO between March 2015 and February 2016. An external quality improvement cycle was applied for the prevention and management of pre-natal urinary infections. This occurred with evaluations of five quality criteria.
Results
Multi-variate analysis of quality improvement, it was observed that most of the criteria of statistical significance (p> 0.001), except criterion 1 which showed a p lower than expected. The criteria 1, 2 and 4 achieved a percentage above 65% compliance in both the samples. With respect to criterion 5, it can be inferred that 10.8% of the analyzed sample contained record examination results EQU and/or altered urine culture, and of these 53% had adequate treatment record.
Conclusion
The methodology used to improve the quality of the external cycle collaborated in the remodeling of the care processes of pre-natal and especially in the integration between care teams and managers of different levels of complexity worked, strengthening co-management and co-participation of workers involved directly in care for users in the municipal health management processes. It has also enabled reflections on the existing flowcharts, providing the re-design of the same as reflected in improving access of pregnant women to health services and quality care.
Key words: pregnancy; pre-natal care; quality management
INTRODUCTION
Gestation is permeated by innumerable physiological, psychological, cultural and social changes that have repercussions on significant changes in the female context1,2. It is a moment that requires health care actions for promotion and protection of injuries, with efficient and effective monitoring, in order to provide improvement in the quality of life for the mother and her fetus3,4.
The Brazilian Ministry of Health has designed strategies to strengthen and to qualify care actions during pregnancy, including the Program for the Comprehensive Assistance to Women's Health (PAISM) and the Humanization Program for Childbirth and Childbirth (PHPN) in order to actions for women2,5.
Anchored in PHPN, the Brazilian government launched the Stork Network instituted by Portaria No. 1459, of June 2011, which aims to improve and to qualify the maternal and child care line in the context of Health Care Networks. One of the principles of this Network is the pre-natal care. Pre-natal care is ensured through user accessibility to the health system, at all health care levels that require obstetric care, as well as the integral care of the specific pregnancy and puerperal cycle. It encourages the organization of the work process of the health services, in the aspects of planning to the monitoring of pregnancy and of its possible intercurrences6,7.
It is the responsibility of the municipalities to design and to implement strategies to ensure the early start of pre-natal care, including periodicity of consultations, health promotion actions and disease prevention through an integrated and effective health network4.
Among the possible fragilities that make pre-natal care difficult is the precariousness of users' access to pre-natal services, poor quality of care, high rates of maternal and perinatal mortality, and the lack of guidelines, especially in aspects related to delivery and childbirth8. Moreover, the shortage of qualified professionals and the precarious infrastructure of services that perform pre-natal care compromise the quality of life of pregnant women and fetuses, exposing them to avoidable risks9.
The frequent complications that affect pregnant women during pre-natal care deserve special attention by health teams, especially Primary Care (PC); the most common are urinary tract infections (UTIs), which are present in about 20% of pregnancies. UTIs are characterized as asymptomatic bacteriuria, cystitis and pyelonephritis, and can be diagnosed with simple urine and uroculture7,10.
When UTI is not treated properly and in a timely manner, it can lead to significant perinatal complications, including amnionitis, premature rupture of amniotic membranes, labor, and preterm delivery. Concerning maternal complications, UTI can cause, among others, bacteremia, septic shock, anemia, dehydration, vomiting, nausea, acute renal and respiratory failure. In addition to the aforementioned alterations, some studies have affirmed that urinary infection is one of the factors related to pre-eclampsia in pregnancy, but still with an unknown causal mechanism7,11,12.
The lack of adequate diagnosis of UTI and timely treatment may imply an increase in maternal and neonatal comorbidities, as well as it may contribute to the saturation of obstetric and neonatal hospital beds, increasing public expenditures for health care at their levels of complexity . The psychosocial and familial aspects that encompass the comorbidities of the mother and child binomial in the puerperal gravid cycle are added as complicating factors of this panorama.
In this perspective of quality of care, the quality management programs provide a set of structured elements with activities that aim at the continuous improvement of the quality of services, among which are the cycles of quality improvement. They can be used to strengthen the managerial functions, contributing to the detection of problems or opportunities, for solving and/or improving them. In addition, they have applicability in different locations and produce knowledge about implantation and results that go beyond the context in which they originate13.
The external cycles of quality improvement present a series of difficulties to be realized, mainly because the evaluation starts from an external body, which is not directly linked to the actions that are proposed. They can opt for solving the problems identified and their answers will be optimized when all the agents involved in the action are integrated. Thus, it is perceived as an active instrument of construction, pointing out necessary articulations between objects, typologies and contexts14.
In the Brazilian health system, the external evaluations of health programs designed for the health of the population are still incipient. The Brazilian scientific literature is scarce in relation to the applicability of quality improvement cycles that evaluate and propose interventionist strategies to improve and to raise the levels of current health practices.
Nowadays, there are weaknesses in the knowledge about these supportive strategies that foster the improvement of the quality of Primary Health Care, especially regarding the management of the health system, assistance in the processes of formation and permanent education of the professionals15.
Among the management strategies currently employed by the Brazilian HM that seek to improve the promotion and prevention of comorbidities, the National Program for Improving Access and Quality of Primary Health Care (PMAQ) has been outstanding and has collaborated in the improvement of actions developed at the primary health level. However, the guiding indicators of this program that evaluate the care processes in women's health in the pregnancy cycle are presented in a simplified way. However, they provoke the remodeling of the actions in the primary health level, but with a purely quantitative focus, focused on the early intake, the proportion of pregnant women registered, number of visits/month performed, gestational immunization, number of home visits, and the ratio of cytopathological examinations in the gestation16.
In view of the presented context, this study aimed to evaluate the effects of an external cycle of quality improvement in the prevention and management of pre-natal urinary infections.
METHODOLOGY
This is a quantitative study, with a quasi-experimental design, before and after, without a control group, performed in Cacoal/RO between March 2015 and February 2016.
Cacoal is a municipality of the Brazilian Legal Amazon, a hub of the Coffee Health Region of the state of Rondônia and the second Macro-region of the state. There are 79,330 inhabitants (2010 Census), of which 50.1% are women, which, for the most part is included in the city's productive services sector. It has a territorial area of 3,792.81 km2 and is located in the south-central region of the State. In health, it has full management in the health system with 71% coverage of the Family Health Strategy in the years 2015 and 2016, whose teams are distributed in eight BHUs17.
The municipality of Cacoal/RO is characterized by a lack of assistance, mainly in the maternal and child care area, and there is a centrality of high complexity services in the state capital, depriving the interior of its capacity to deal with cases of greater severity. This characteristic contributes to the increase of maternal and neonatal morbidity and mortality rates in that locality.
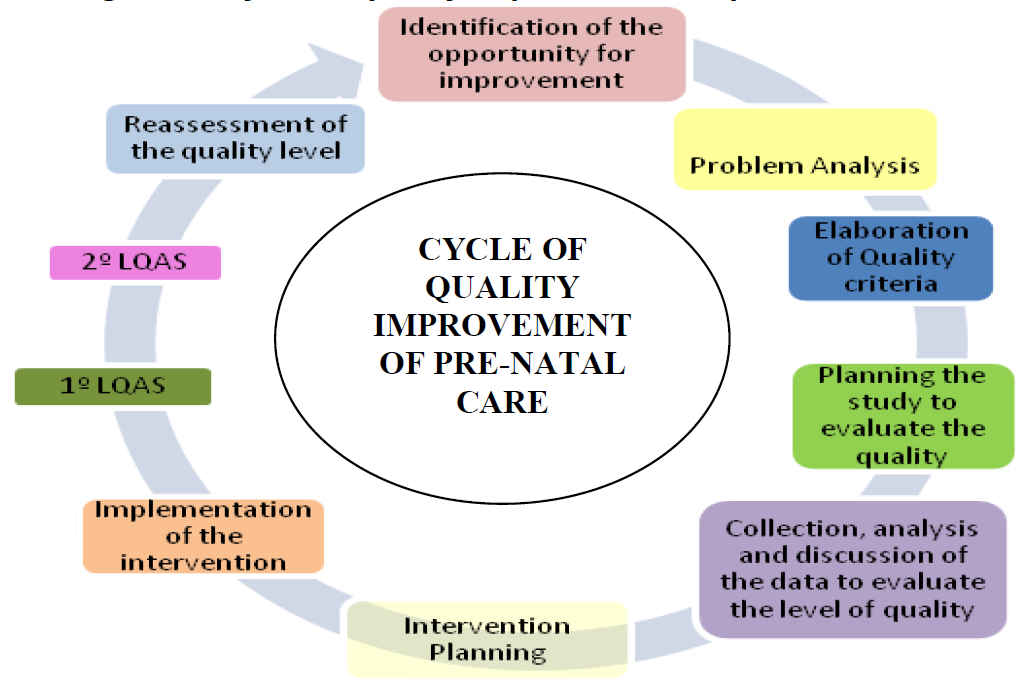
An external cycle of quality improvement was applied (Figure 1) for the prevention and management of pre-natal UTIs. This occurred with evaluations of five quality criteria and two sentinel indicators. Two evaluations were carried out, with a three-month temporality between them, and among them two Lot Quality Acceptance Sampling (LQAS) monitoring. Between the first and second evaluation, a participatory intervention was planned and guided by the results of the first evaluation.
This cycle is part of the activities proposed by the Quality Management Programs aimed at developing and improving the effectiveness, efficiency and satisfaction of the main actors in health care, and should be a conscious and quantifiable process for the excellence of services13. It is considered an external cycle, since it emerged as a strategy proposed by the Second Regional of Health Department of the State of Rondônia (IIGRS), to qualify maternal and child care in the region.
In order to identify the level of quality, the point estimate and confidence interval (95%) were used to meet the criteria. And, in order to prove the effectiveness of the intervention, the absolute and relative improvements between the first and second evaluation were calculated, as well as their statistical significance with unilateral z-test.
For fast assessments with LQAS the sample size and decision number for conclusions were calculated based on 5% of false positives and 10% of false negatives in the identification of problem situations. Thus, the sample was of 17 cases, being accepted the lot when 12 cases of compliance with the criteria were present.
For the applicability of the external improvement cycle, the first evaluation of the quality level was made based on the construction and application of pre-natal care quality criteria, intervention planning and two lot sampling monitoring activities, called LQAS-Lot Quality Acceptance Sampling. Subsequently, a reevaluation was performed to analyze the fulfillment of the previously established criteria as quality standards. These monitoring enabled decision-making based on small samples to compare with an estimation of the level of quality of the desired standard19.
The cycle was developed over a period of 12 months and involved municipal health care institutions at the primary and secondary levels that offer standard and high risk prenatal care according to the programmed and spontaneous demands of each service.
The quality criteria used were selected based on the recommendations of the Ministry of Health for routine and high-risk pre-natal care. They were adapted to the realities of the municipality and became indicators of quality of gestational care. The face, content and criterion validities were ensured in all these criteria. In addition, the Kappa index, whose accepted values for each criterion evaluated was> 0.6, was calculated.
The planning of the interventions proposed by quality management programs was based on the analysis and discussion of results of service evaluations. These interventions used structured methods that ensured the participation of those involved in the problem and monitored the implementation of improvement strategies. Interventions were most effective because they were data-driven and planned with the participation of all those responsible for the practice19. The actions were grouped according to the following categories:
Category 1 -Management:among the actions developed are: elaboration of the protocol of care for pregnant women who are affected by UTI, reorganization of the care flow of pregnant women, redistribution of urine sample and EQU examinations among BHUs, strategies were designed of optimization of quotas, tactics were traced to identify alteration of the results of exams and active search of the pregnant women for treatment in a timely manner; planning was carried out to provide materials and supplies in sufficient quantity to meet the demands of the health units; creation of groups of pregnant women in the BHUs that had not completed this type of activity and strengthened those that were already performed, proposing the incorporation of the other groups of pregnant women who were coordinated by the Pastoral da Criança in the municipality.
Category 2 -Training:a) Assistance to pregnant women affected by urinary tract infections, according to the protocol created, in order to standardize the care provided. b) Interpretation and guidance on the collection of routine pre-natal laboratory exams. c) Workshop with community health agents when subjects related to the importance of early fetal initiation for pre-natal initiation, compliance with pre-natal consultation routines, provision of information for active search of pregnant women with risk for obstetric and neonatal complications and symptomatology suggestive of urinary tract infection, for capturing and caring, in a timely manner, minimizing damages to the mother/child binomial
Category 3 -Users:were strengthened, along with health professionals, to promote co-responsibility of the users in the quest for the quality of pre-natal care.
Subsequent to the design of the actions to be implemented, and in order to follow up and to supervise the execution of the actions, the Gantt diagram was constructed, which represents the correct temporal sequence of the activities of the action plan19.
The analysis of the data resulting from the two evaluations and the monitoring cycles followed the recommendations of the quality management programs. Dichotomous variables of the quality criteria were evaluated. For the evaluation and reassessment, a point estimate was calculated with a 95% confidence interval of the level of compliance of the criteria in the selected random samples, with calculation of the absolute and relative improvements of each quality criterion. And, in order to prove the statistical significance of the identified improvement, a unilateral hypothesis test was performed, by calculating the value of z, considering as null the null hypothesis to the absence of improvement, which was rejected when the p-value was less than 0,0520.
This study followed the relative ethical aspects according to Resolution 466/12 and 510/16.
RESULTS
During the first evaluation of pre-natal quality, some fragility was observed in the fulfillment of most of the quality criteria designed for this study, as shown in Table 1. The Ministry of Health recommends the screening of gestational UTIs in the first and third trimesters for all pregnant women, encouraging the improvement of care with early diagnosis and treatment in a timely manner7.
Table 1. Quality levels of the 1stand the 2ndassessments after the intervention performed and statistical significance of the improvement identified, Cacoal, RO, Brazil, 2015/2016

C1 - Pregnant women should start pre-natal care before the 12thgestational week
C2 - Pregnant women should undergo the type I of the urine test in the third trimester of pre-natal carep
C3 - Pregnant women should perform urine sample test in the third trimester of pre-natal care
C4 - Pregnant women should have their urine tests evaluated in the consultation subsequent to the one in which their request is made, according to the routines of pre-natal consultations, performed according to the gestational age
C5 -Pregnant women with type I urine with leukocyturia and/or positive urine sample test should be adequately treated in the Basic Health Unit and/or referred to the referral service for high-risk pre-natal care
Among the main gaps observed in this study, the lowest proportion of criteria for urine sample examinations (17%) was observed, followed by therapeutic management with results suggestive of gestational UTI (38%), %), and early capture (79%). The criterion for conducting the consultation was 89%, and the best performance against the evaluated results.
In the analysis of quality improvement, it was observed that most of the criteria presented statistical significance (p <0.001), except criterion 1, that presented a higherpthan what was expected. Through the results presented in Table 1, which reveal the absolute, relative improvement and statistical significance, the levels of fulfillment of pre-natal quality improvement criteria are visualized. Criteria 1, 2 and 4 achieved a percentage above 71% in their compliments.
Regarding criterion 5, it can be inferred that in 10.8% of the sample analyzed, the results of altered EQU and/or urine sample exams were recorded, of which 53% had adequate treatment records. Among the evaluated criteria, it can be evidenced that the registries, in relation to the care and therapeutic actions, regarding gestational UTIs, had a significant absolute improvement (33%), standing out against the other parameters evaluated.
In the rapid assessments, systematized by the LQAS, which briefly monitored the intervention in relation to criteria 1 to 4, only the early collection and the pre-natal consultation were accepted in the first evaluation. In the second rapid assessment, only the performance of the urine sample examination did not reach the desired quantity, which was 12 compliments for the acceptance of the batch analyzed.
Priorities of Intervention
As prioridades de intervenção foram representadas por meio do diagrama de Pareto antes e depois, representado na Figura 2. Ele apresenta a frequência dos não cumprimentos dos critérios avaliados, na primeira e na segunda avaliação, do maior ao menor número das inconformidades, além da curva de frequência acumulada. Objetiva apontar os defeitos de qualidade, permitindo uma melhor compreensão das prioridades intervencionistas planejadas para este estudo, além de dar visibilidade gráfica às melhorias atingidas com a intervenção.

The data presented in Pareto Diagram 2, observed in the first evaluation, guided intervention planning, which, among the "little vital" quality problems, criteria 3 and 2 were the ones prioritized in the design of improvement strategies. These criteria represent more than 50% of the nonconformities in the execution of the pre-natal actions. And in the re-evaluation, it is visualized an improvement in the conformity of the four evaluated criteria. However, criterion 3 continues with more than 50% of non-compliance.
DISCUSSION
Compared with baseline leveling and the techniques used to plan the intervention, it was observed that the results could be hypothetical, related to the current work processes in the municipal basic network and the lack of standardization of care for pregnant women with UTI. Another possible inference to justify these results would be the lack of knowledge of the professionals regarding the flowchart of the examinations of EQU and urine sample test, which were the main driving factors for the interventionist activities and which guided the proposed strategies.
In view of the objective of improving the pre-natal care quality proposed and guided by the improvement cycle, it can be inferred that early capture (C1), despite being a criterion that needs to be improved, has presented since the first evaluation a proportion of accomplishments within the national standard (79%), and according to the indicators that guide the national PMAQ16. Despite this finding, it was decided to keep it within the interventionist context of improvement to increase the number of pregnant women who initiate their pre-natal care in a timely manner. The early collection did not reach a level of statistical significance, but had, after the intervention, an absolute improvement of 4%, which contributes to the increase of access and the number of pre-natal consultations as recommended by the Ministry of Health.
It is believed that early capture is intrinsically related to the accessibility of pregnant women to services that perform pre-natal care. It is necessary to strengthen strategies that allow women to perform rapid pregnancy tests at BHUs, because although this prerogative is recommended by the Stork Network, it is still not a practice performed at the primary level of the municipality in the period studied.
The early initiation of gestational care promotes the accessibility to diagnostic and therapeutic methods for pathological investigation that can affect the health of the mother/child binomial. It is emphasized that a more accurate estimate of gestational age, in order to refine the monitoring of fetal growth and development, provides a better arsenal to support decisions related to care and possible interruption of pregnancy9.
Health promotion and education practices need to be implemented and activities outside health units need to be effective. The municipal management should seek entities that guarantee health actions and reassure the collectivities where these pregnant women are inserted, aiming at adding institutions to strengthen the activities carried out by municipal health co-ordinations.
The improvement in the actions of attention to women also reflects the results of continuing education activities carried out with primary health care professionals on urinary tract infections in pregnancy and their possible complications. It is corroborated that the action of changing the practices, the work process of the subjects and their relationships, is essential to the qualification of health management, education and participation, demands education processes to transform work practices20.
Regarding the performance of the common urine tests, the data indicate that there was an absolute improvement of 24% in compliance with this criterion of pre-natal care quality proposed in this study. The HM care protocol advises that all pregnant women perform at least one EQU in the last gestational trimester, aiming at the screening, diagnosis and timely treatment of gestational urinary infections7.
The EQU test should be performed at least once in the last gestational trimester, which affects directly the reduction of perinatal diseases and maternal and neonatal morbidity and mortality, and, in addition to benefiting from the binomial, decreases public expenditures resulting from hospital admissions7,21. It is believed that outpatient treatment of urinary tract infections, in addition to being less expensive, allows greater comfort, convenience, safety and reduces the risks of a hospital treatment.
However, it is observed that 89% of the pregnant women had undergone UTI screening, with the EQU examination. It is corroborated that the absence of results in 100% of the pregnant women represents loss of the opportunity for diagnosis and treatment of possible control complications, thus providing negative perinatal outcomes and for which effective preventive interventions can be generated9.
In this perspective, it is pointed out that the screening of the urinary tract infection during pregnancy, even in cases of absence of clinical symptoms, is an indicator of the pre-natal care quality. The failure to perform common urine tests and uroculture at least once in the last gestational trimester may lead to maternal and neonatal comorbidities, including an increase in the mortality rate of this target population12.
However, although the EQU test is extremely useful in the screening of urinary tract infections during pregnancy, uroculture is still considered the gold standard for the diagnosis of these diseases7,22. It is indicated for the screening and diagnosis of symptomatic or asymptomatic urinary tract infections and to control treatment after seven days of antibacterial therapy21.
This study indicates a significant improvement of 30% between the baseline level and the second evaluation of the criterion of quality of achievement of EQU. However, despite the realization of improvement strategies that were monitored by the rapid evaluations, gaps still remain to be observed, since only 47% of the pregnant women performed the uroculture in the last gestational trimester in the analyzed period. This may have an unfavorable impact on the prenatal care quality. The objective is that 100% of the pregnant women can have their examination guaranteed and performed and, with this, there may be a decrease in the perinatal mortality rates of the municipality, whose basic causes of deaths are related to maternal urinary tract infections7.
The Ministry of Health, through the Stork Network, has financed 100% of the culture of bacteria in the urine in prenatal examinations6. It is a further stimulus of costing in public management to enable that municipalities do not use their own resources for such a procedure. This strategy may contribute to the guarantee of all pregnant women with gold standard screening and diagnosis for urinary tract infections. The lack of financial resources for this was not a gap identified in relation to those results, since the municipality had joined the Stork Network and had already received a cost incentive to offer these exams.
It is believed that health managers need sensitivity and responsibility to ensure that their teams are able to comply with prenatal care routines by keeping quotas of examinations in sufficient quantity. In addition, encouraging and employing management strategies, such as quality improvement cycles that assess care actions, interfere with care practices, and improve the results of work processes that are very important for quality care of pregnant women.
Based on the results of this study it is possible to infer that there is a need to strengthen the care processes, regarding gestational UTIs in prenatal services. It is an examination that deserves to be valued by the professionals of the basic attention, mainly for the guiding therapeutic thermometer, which refers to positive results for the adopted behaviors and corroborates for the reduction of maternal and neonatal comorbidities.
The criterion for evaluating pre-natal care appointments in the last trimester, from the first evaluation, indicates a satisfactory percentage of compliance (89%), with an absolute improvement of 9% after the intervention. At the same time, it is important that pregnant women have their exams evaluated and gestational consultations guaranteed according to the schedule established by the Ministry of Health7.
The user approach needs to be based on the gestational risk of the last trimester, especially those ones that are related to repetitive UTIs, the characteristics of the users and the prevalence of the most common diseases of this period of pregnancy23. It is believed that the return of the users to the BHUs contributes to the improvement of quality pre-natal care and guarantees maternal and neonatal health through the identification of risk situations that can lead to unfavorable outcomes.
More significant improvement was sought in the conduct of the appointments. However, the result found suggests that it is related to the care culture of the third gestational period, from the search for pre-natal care to hospital institutions in the city, by association of possible symptomatologies to the predictive signs of labor and delivery. There is also fragility in the records of the visits to pregnant women performed by professionals in these institutions.
The criterion for evaluating the records of drug therapy in the face of the tests with indicative results of UTIs was the one that had the highest absolute improvement compared to other parameters evaluated (33%) in both evaluations. This result refers to the importance of the intervention that had repercussions in strengthening the work processes of health teams that perform pre-natal care and in raising the awareness of the importance of care records in pregnancy record cards. This logic of thought reaffirms the standardization of medication assistance in case of pathological confirmation and, mainly, of the potential risk assessment of the neonatal complication in the gestational period studied, which has repercussions on the remodeling of the care practices of the staff who cares birth and delivery.
The rapid assessments, such as the LQAS that was used between the systematic ones, helped in the maintenance of the direction of the activities proposed by the intervention and in the identification of care and managerial gaps that permeated the strategies designed for this intervention. This evaluative modality facilitated the maintenance of the direction and the design of activities that were proposed after the basal leveling and collaborated to improve all the evaluated criteria18.
Some authors have affirmed that the main problems that corroborate the unfavorable outcome of gestation are directly related to the failures in the prevention and response capacity due to intercurrences during gestation, delivery and puerperium, coinciding with the perinatal period24,25.
There is a need to qualify the pre-natal care methodologies, prioritizing the investment in strategies to qualify care practices and quality care management, such as the improvement cycles that have been presented in this study.
The quality improvement cycles encourage the improvement of the practices, the redirection of the management activities, implying in the improvement of the objectives that are proposed and of the work contexts. They improve the effectiveness, efficiency and satisfaction of all those people involved, aiming at excellence in the quality of services13,15.
Pregnant women also need to be encouraged to have commitment and co-responsibility for the unique care at this moment of their lives. It is argued that this is possible when women feel integrated into caregiving, with adequate and equiTable access to health services that perform pre-natal care. This service should be based on the guiding principles of SUS and the humanization of care, with individualized and integrative care.
FINAL THOUGHTS
This study made it possible to identify gaps in care and management that are considered fundamental for the quality of pre-natal care, and recommended by the maternal-child health care network. It allowed reflections on the current flow charts, providing their redesign, which reflected in the improved access of pregnant women to health services and the quality of care. In addition, it can be inferred that improvement cycles are an important quality improvement tool that can be used by managers in the three spheres of public management to evaluate, to monitor and to improve identified problems, looking for effectiveness, efficiency and excellence in the expected results.
It presents as limits the absence of standardization in the records of the cards, which affected the quality of the data and the lack of important information for the analyses carried out, including outcome variables, explanatory or effect modifiers. Also, the lack of control in sustaining that the change in the improvement of the presented indicators is associated intrinsically to the intervention or to other factors related to the health context. In addition, the design used has not allowed the control of some confounding variables. In order to give sustainability to the results pointed out by this study, new measurements should be made, besides the control of the biases identified here.
It is suggested the complementarity of qualitative research, which allows the understanding of factors whose results are not provided by quantitative research. It is believed that this association fosters more favorable and impacting results in the access and quality of care in the different health care levels.
REFERENCIAS
1. Silva LS,Pessoa FB, Pessoa DTC, Cunha VCM, Cunha CRM, Fernandes CKC. Análise das mudanças fisiológicas durante a gestação: desvendando mitos. Revista Faculdade Montes Belos. 2015;8(1):1-16. [ Links ]
2. Brasil. Ministério da Saúde. Programa de Humanização no Pré-natal e Nascimento. Brasília: Ministério da Saúde; 2000. [ Links ]
3. Guimarães WSG, Parente RCP, Guimarães TLF, Garnelo L, Acesso e qualidade da atenção pré-natal na Estratégia Saúde da Família: infraestrutura, cuidado e gestão. Cad Saúde Pública. 2018;34(5):1-13. [ Links ]
4. Silva EP, Lima RT, Ferreira NLS, Costa MJC. Pré-natal na atenção primária do município de João Pessoa PB: caracterização de serviços e usuárias. Revista Brasileira de Saúde Materno Infantil. 2013;13(1):29-37. [ Links ]
5. Holanda CSM. Ciclo gravídico puerperal: avaliação da assistência no serviço público de saúde. [Tese]. Natal: Universidade Federal do Rio Grande do Norte; 2015. [ Links ]
6. Brasil. Ministério da Saúde. Portaria nº 1.459 de junho de 2011. Institui a Rede Cegonha. Diario Oficial da União 2011; 24 jun. [ Links ]
7. Brasil. Ministério da Saúde. Atenção ao Pré-Natal de Baixo Risco. Brasília: Editora do Ministério da Saúde, 2012; 320 p. [ Links ]
8. Tomasi, E. et al. Qualidade da atenção pré-natal na rede básica de saúde do Brasil: indicadores e desigualdades sociais. Cadernos de Saúde Pública. 2017;33(3) e00195815. [ Links ]
9. Domingues RMSM, Hartz ZMA, Dias MAB, Leal MC. Avaliação da adequação da assistência pré-natal na rede SUS do Municipio do Rio de Janeiro. Cadernos de Saúde Pública, 2012; 28(3):425-37. [ Links ]
10. Ahmed MA, Shukla GS, Bajaj HK. Incidence of Urinary Tract Infectons and determination of their susceptibility to antibiotics among Pregnant Women. International Journal of Cell Science and Biotechnology. 2016;5(1). Disponível em: http://inpressco.com/wp-content/uploads/2016/01/Paper212-16.pdf [ Links ]
11. Oliveira SMJV; Caroci AS; Mendes EPB; Oliveira SG; Silva FP. Disfunciones del suelo pélvico en mujeres primíparas después del parto. Enfermería Global. 2018;(51):26-39. [ Links ]
12. Hackenhaar AA, Albernaz EP. Prevalência e fatores associados à internação hospitalar para tratamento da infecção do trato urinário durante a gestação. Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(5). [ Links ]
13. Saturno PJ. Planejamento e implantação de programas de gestão da qualidade em serviços de saúde: módulo I [recurso eletrônico] / Pedro Jesus Saturno Hernández; Zenewton André da Silva Gama (tradutor). - Natal: SEDIS-UFRN, 2017. [ Links ]
14. Portela MC, Pronovost PJ, Woodcock T, Carter P, Dixon-Woods M. How to study improvement interventions: a brief overview of possible study types. BMJ Quality & Safety. 2015;24(1):325-36. Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/25810415 [ Links ]
15. Pinto LF; Rocha CMF. Inovações na Atenção Primária em Saúde: o uso de ferramentas de tecnologia de comunicação e informação para apoio à gestão local. Ciênc saúde colet. 2016;21(5):1433-1448. [ Links ]
16. Brasil. Ministério da Saúde. Programa Nacional de Melhoria do Acesso e da Qualidade da Atenção Básica: Manual Instrutivo. Brasília, 2012. [ Links ]
17. Cacoal, Secretaria Municipal de Saúde. Relatório de Gestão do 4º trimestre de 2015 do Município de Cacoal/RO. 2015. [ Links ]
18. Métodos e instrumentos de monitoramento da qualidade: módulo IV [recurso eletrônico] / Pedro Jesus Saturno Hernández; Zenewton André da Silva Gama (tradutor). - Natal: SEDIS-UFRN, 2017. [ Links ]
19. Saturno PJ. Atividades básicas para melhoria contínua: métodos e instrumentos para realizar o ciclo de melhoria: módulo II [recurso eletrônico] / Pedro Jesus Saturno Hernández ... [et al.]; Zenewton André da Silva Gama (tradutor); Pedro Jesus Saturno Hernández (organizador). - Natal: SEDIS-UFRN, 2017. [ Links ]
20. Pinto HA. Política Nacional de Educação Permanente em Saúde: aprender para transformar. In: Gomes LB; Barbosa MG; Ferla AA.(Orgs). A Educação Permanente em Saúde e as Redes Colaborativas: conexão para a produção de saberes e as práticas. Série Atenção Básica e Educação na Saúde. 1º Ed. Porto Alegre: Rede Unida, 2016. [ Links ]
21. Vettore MV, Dias M, Vettore MV, Leal MC. Avaliação do manejo de infecção urinária no pré-natal em gestantes do Sistema Único de Saúde do Município do Rio de Janeiro. Revista Brasileira de Epidemiologia. 2013;16(2). [ Links ]
22. Federação Brasileira das Associações de Ginecologia e Obstetrícia (FEBRASGO). Comissões Nacionais Especializadas Ginecologia e Obstetrícia. Manual de orientação: gestação de alto risco. 2011;197-204. [ Links ]
23. Mayor MS, Herrera SDSC, Araujo MQA, Santos FM, Arantes RV, Oliveira NA. Avaliação dos Indicadores da Assistência Pré-Natal em Unidade de Saúde da Família, em um Município da Amazônia Legal Revista Cereus. 2018;10(1):91-100. [ Links ]
24. Netto A, Silva RMM, Santos MF, Tacla MTGM, Caldeira S Brischiliari SCR. Mortalidade infantil: avaliação do programa rede mãe paranaense em regional de saúde do Paraná. Revista Cogitare enfermagem. 2017;22(1):1-8. [ Links ]
25. Ronchini CE, Franchini AA, SIIERO PC. Mortalidade Infantil e na Infância no Brasil de 1990 a 2011: Acompanhamento dos Objetivos de Desenvolvimento do Milênio (ODMs). Caderno de Estudos Interdisciplinares 2014; 1(1):57-66. [ Links ]
Received: October 07, 2018; Accepted: December 14, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
