










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.19 no.60 Murcia oct. 2020 Epub 21-Dic-2020
https://dx.doi.org/10.6018/eglobal.422331
Originals
Acute coronary syndrome in women from the theory of symptom management
1Nursing Program. Universidad Surcolombiana. Colombia
2PhD in Health Sciences. Universidad Surcolombiana. Colombia
Objective:
To identify the risk factors for cardiovascular disease and the experience of the symptom of Acute Coronary Syndrome (ACS) in women, according to the theory of Symptom Management.
Method:
Observational cross-sectional study, 81 women with ACS attended at a University Hospital in Colombia participated. Sociodemographic variables, risk factors for cardiovascular disease, response actions to symptoms and perception, evaluation and response to symptoms were analyzed through the instrument application on the Experience of the Symptom in Women with ACS.
Results:
Of participants 80% were over 60 years old, the majority with a low level of education and urban residence. The main risk factor was hypertension and more than 50% of them reported sedentary lifestyle, dyslipidemia, and an unhealthy diet. Women presented an average of 10 atypical symptoms for each event, highlighting chest pain or discomfort in 85%. 66.3% defined the origin of the symptom as an extra-cardiac conditions and 4 out of 10 patients considered the manifestations as insignificant. 16% of the participants took home remedies and 25% of them waited the symptoms to improve without request professional attention. The relationship between time in attending medical consultation and ignoring the symptoms presents statistical significance (p = 0.000).
Conclusions:
Women with ACS presented a variety of symptoms, do not perceive the severity of its manifestations, and generally respond late to symptoms, a relevant factor for timely care and treatment.
Key words: Acute Coronary Syndrome; Clinical manifestations; Women; Nursing theory
INTRODUCTION
Acute Coronary Syndrome (ACS), with a higher degree of complications in women, is a set of manifestations caused by decrease in myocardial oxygen supply as a result of a thrombus in the coronary arteries lumen, after a ruptured atherosclerotic plaque or coronary vasospasm. It may lead to unsTable angina, acute myocardial infarction, or sudden death.1
ACS is part of the group of cardiovascular diseases (CVD) that constitute the leading cause of mortality worldwide, with more than 17 millions of these events per year; more than three-quarters of CVD deaths occur in low- and middle-income countries.2,3
In Latin America CVD affect 27.7% of the adult population approximately, whose cost exceeds 30 billion dollars.4 In Colombia, there is a higher total expense in their health system for this cause, with an approximate cost of 2.4 billion dollars. In addition to the economic implications, CVD alter population dynamics, decrease productivity, cause absenteeism and loss of years of healthy life by 18.37%.5
Currently, the ACS is one of the main diagnoses of morbidity and generates a large number of consultations in the emergency services with high demand for health resources.1,2 Overview, those who suffer from the syndrome present risk factors for CVD (modifiable and non-modifiable) that condition this pathology, and some of them, impact in a greater proportion to women, like dyslipidemia, Diabetes Mellitus (DM), and high blood pressure mainly.6,7
Hormonal response have an important role in the involvement of women by ACS, since estrogen at the vascular level translates into a positive reaction with nitric oxide in the inhibition of vascular atherosclerotic process;8 this decrease due to menopause brings about hemodynamic changes and changes in the lipid profile, because as estrogen levels decrease, HDL decreases, causing a progressive increase in LDL cholesterol, a precursor to the formation of atherosclerotic plaques.1,9
ACS manifestations are classified as typical and atypical; the former are related to discomfort, chest pain radiating to the upper limbs and diaphoresis.10 The latter, more frequently present in women, are associated with dyspnea, palpitations, fatigue, tiredness, jaw, neck, cough, and digestive disorders such as loss of appetite, nausea and vomiting. 11
The atypical manifestations for ACS are incomprehensible to relate to a cardiac disorder; therefore, they are difficult to identify and classify, which delays the management of diagnostic tests and timely treatments, leading to a higher rate of complications such as cardiogenic shock and death.1,12
It is the responsibility of nursing professionals to provide comprehensive care to people with ACS; for which they must assume leadership in the differentiation of manifestations that channel the development of successful and timely interventions. In this sense, the medium-range Symptom Management theory provides the conceptual support of the present study; approach from which is assumed a multidimensional process that allows the symptoms to be seen as subjective experiences that reflect a change in a person's biopsychosocial function, sensation or cognition.13,14
In this way, the objective of the present study was to identify the risk factors for cardiovascular disease and the experience of the ACS symptom in women, according to the theory of Symptom Management.
METHODOLOGY
Descriptive, correlational cross-sectional study. The population consisted of women with diagnosis and treatment for ACS, treated at the "Hernando Moncaleano Perdomo" University Hospital, located in the Surcolombian region, during the months from January to April 2018.
The type of sampling used was for convenience and the finite population equation to calculate the sample size, taking as reference the information on the average number of patients treated for this cause in the previous year, getting 81 patients.
Inclusion criteria for this research were: Women older than 18 years, confirmed diagnosis of ACS for the first time (clinical, electrocardiogram, biomarkers, and angiography), hemodynamically sTable, having no pain and desire to participate in the study. Women with cognitive or mental disorders that do not allow communication were excluded.
Date were collected by reviewing medical records, an exercise that allowed the identification of important sociodemographic variables, cardiovascular risk factors, clinical manifestations and response time to symptoms, according to the clinical practice guideline for the ACS.
In addition, in a private interview with each study participant, the instrument that evaluates the experience of the symptom designed in Colombia by Cespedes was applied, based on the theory of symptom management. This instrument includes three dimensions: perception, evaluation, and response to the symptom14, it has 37 items, with a dichotomous response option, and adequate validity and reliability.
The information was obtained by researchers directly, after obtaining endorsement by the Institutional Ethics Committee and signing by the participants of informed consent. In both cases, study objectives, methods to be used, and benefits for each of the participants were socialized.
The analysis variables were sociodemographic characteristics (age, place of residence, socioeconomic status, level of education, marital status, social security system, occupation) and modifiable and non-modifiable risk factors for cardiovascular disease. Likewise, the medical diagnosis, place and activities carried out during the symptom and times to seek care help were verified. Lastly, the perception, origin, seriousness and response to ACS symptoms were evaluated.
Date collected were condensed in Microsoft Excel 2016, then exported to the STATA 14® statistical program, for the respective processing. Descriptive statistics were used in the analysis through frequency distribution and measures of central tendency. For the bivariate analysis, the Pearson's chi-square test was applied, taking a value of p <0.05 as significant.
This inquiry was carried out taking into account the ethical principles for research in human beings (Declaration of Helsinki), the scientific, technical, and administrative standards for health research in Colombia (Resolution 8430/1993) and the code of ethics for Nursing (Law 911 from 2004).
OUTCOMES
The women with ACS participating in the study were a total of 81, with a minimum age of 50 and a maximum of 91 years, with an average of 71 years. Eight of every 10 participants live in the urban area, 88.9% of them belong to the low socioeconomic stratum (1 and 2); more than half report income under the minimum wage. 76.5% of the participants reported not having any incomplete primary or school level; Approximately half of them have family support, manifested in married civil status (35.8%) and cohabitation (13.6%). More than 80% are engaged in housework and are affiliated with the subsidized health system.
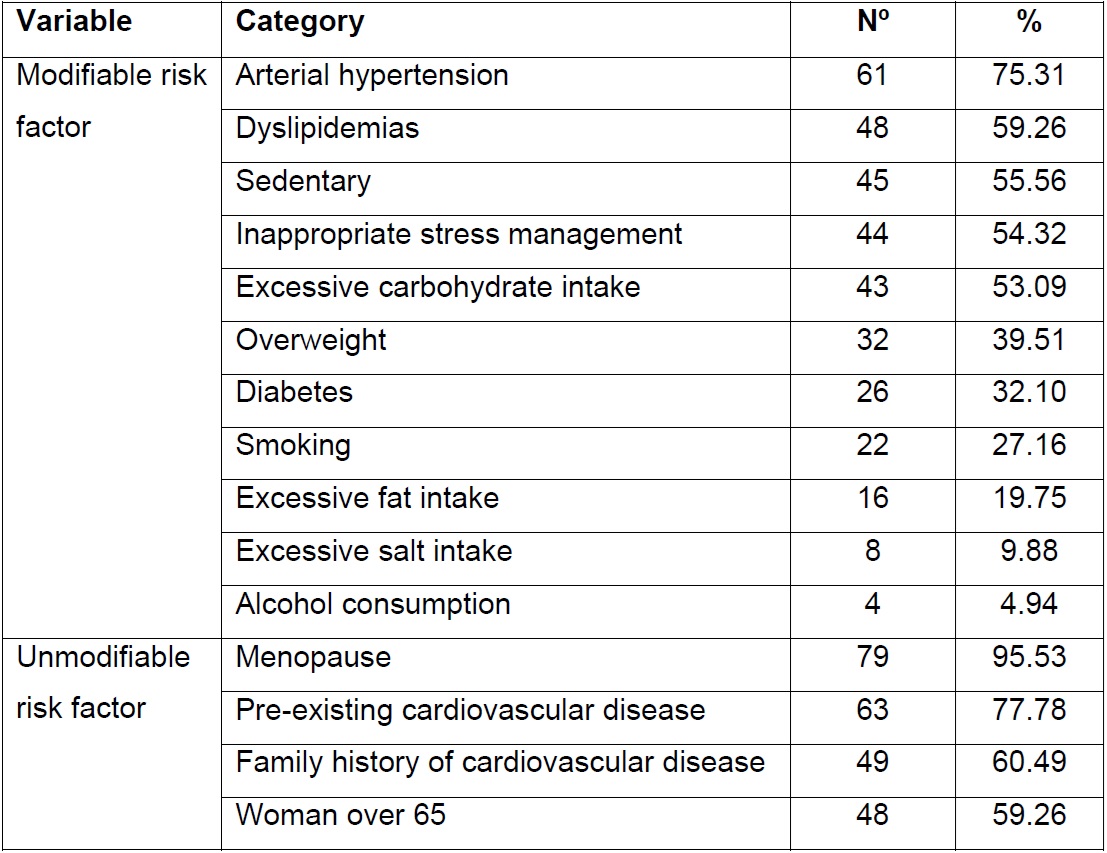
In health / disease domain, it was evident that prevailing medical diagnoses were acute myocardial infarction (AMI) in its different classifications with 78%, and Angina with 22%. The modifiable risk factors for cardiovascular disease were mainly those related to chronic non-communicable diseases and unhealthy lifestyle habits (Table 1). Likewise, it was identified that 73% of the participants suffered from 3 to 5 risk factors, 21% from 1 to 2 risk factors, 4% presented 6 risk factors, and only 2% of participants did not present any modifiable risk factor. The non-modifiable risk factors found were mainly menopause and a family history of CVD.
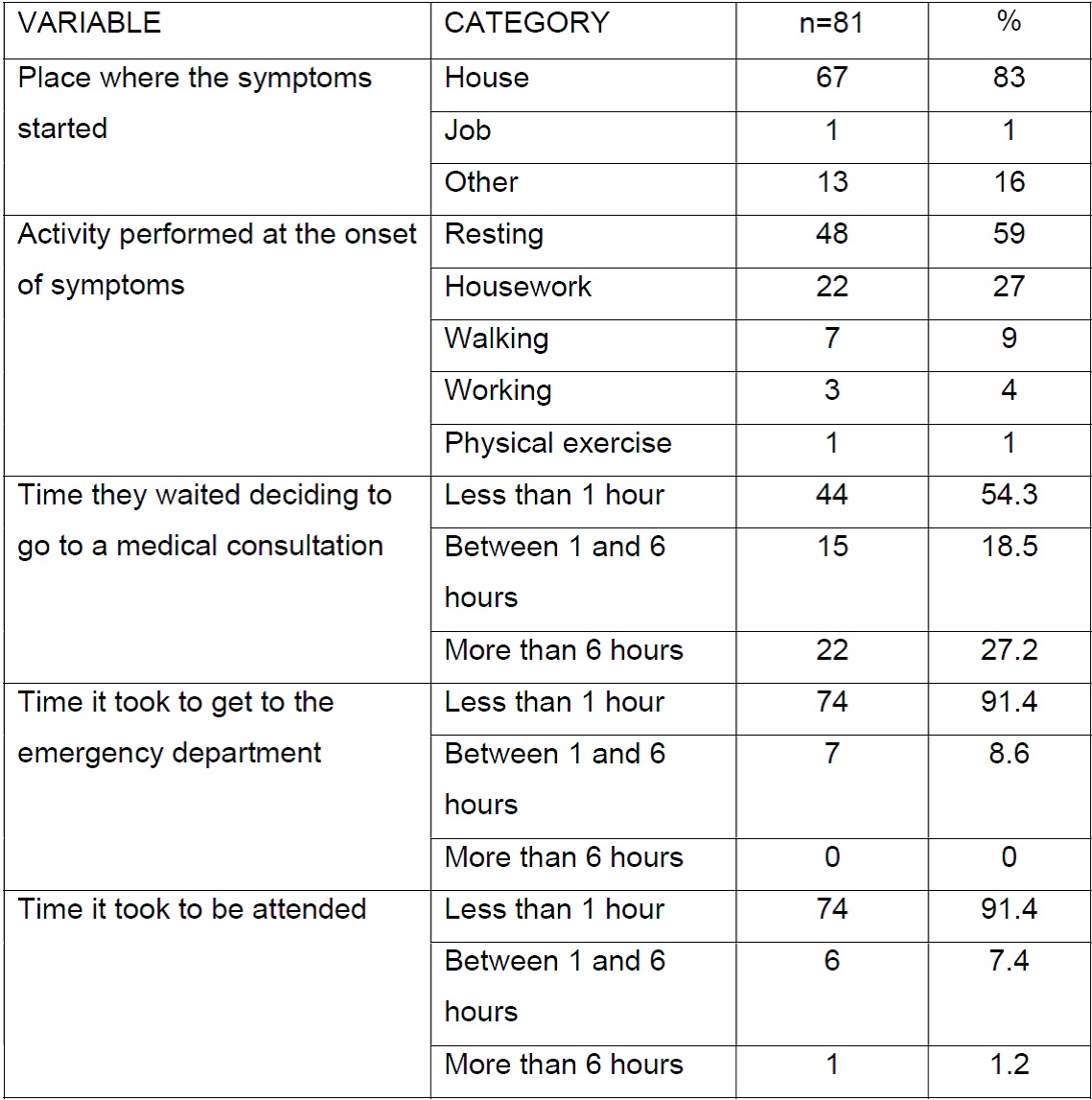
Most women reported that symptoms started at home while they were resting. The delay time variable reports that most of them took less than an hour to decide to seek medical help; Likewise, in the first hour they arrived at emergency department and received professional attention (Table 2).
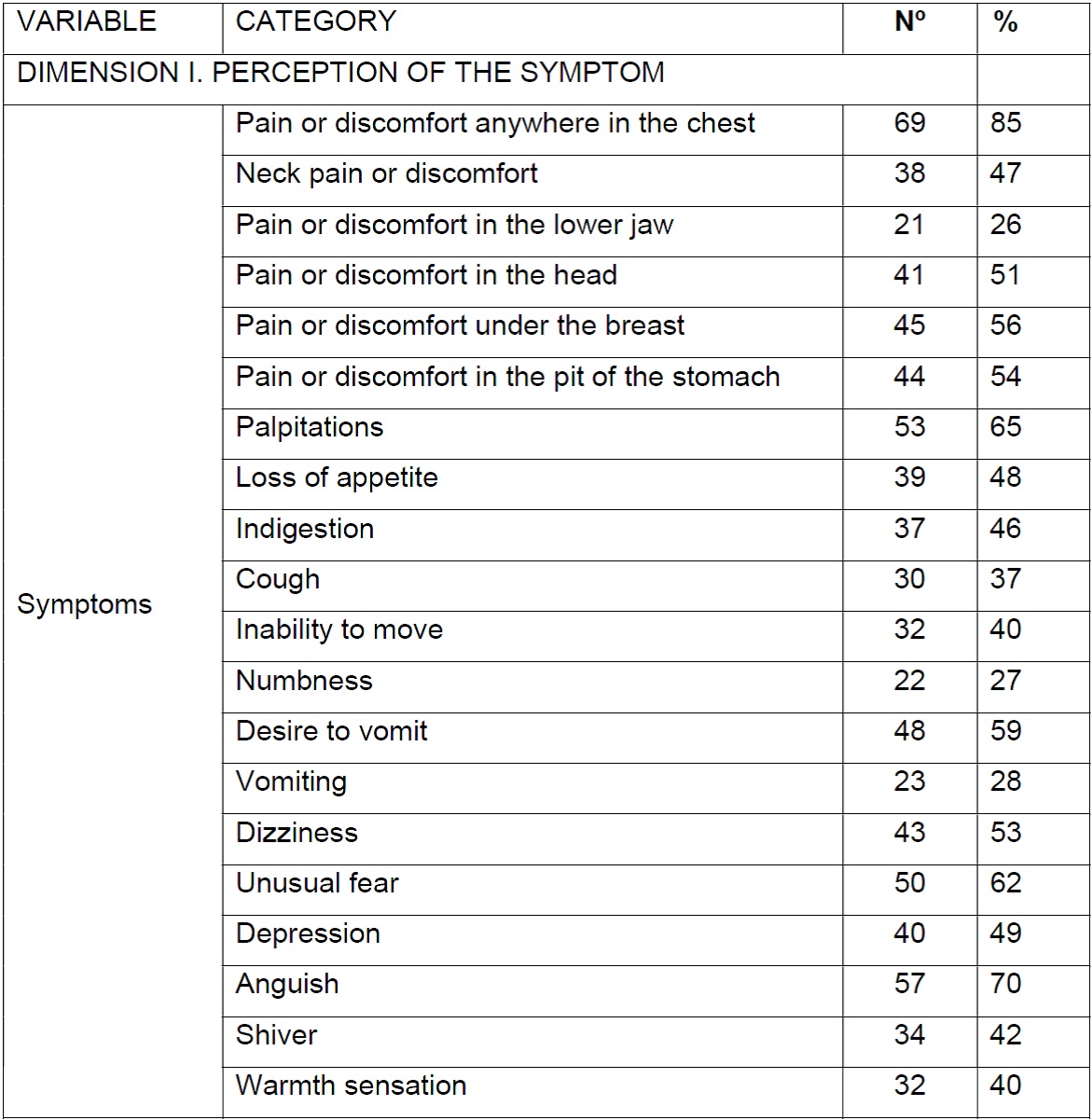
The experience of the symptom was evaluated through the Céspedes instrument, which in the first dimension allows to establish the perception of symptom (Table 3) by means of the question: when did it all start did you feel ...?, It was found that the average of symptoms reported by women with ACS is ten atypical symptoms simultaneously, pain or discomfort anywhere in the chest with 85% of cases, followed by distress, palpitations and unusual fear.
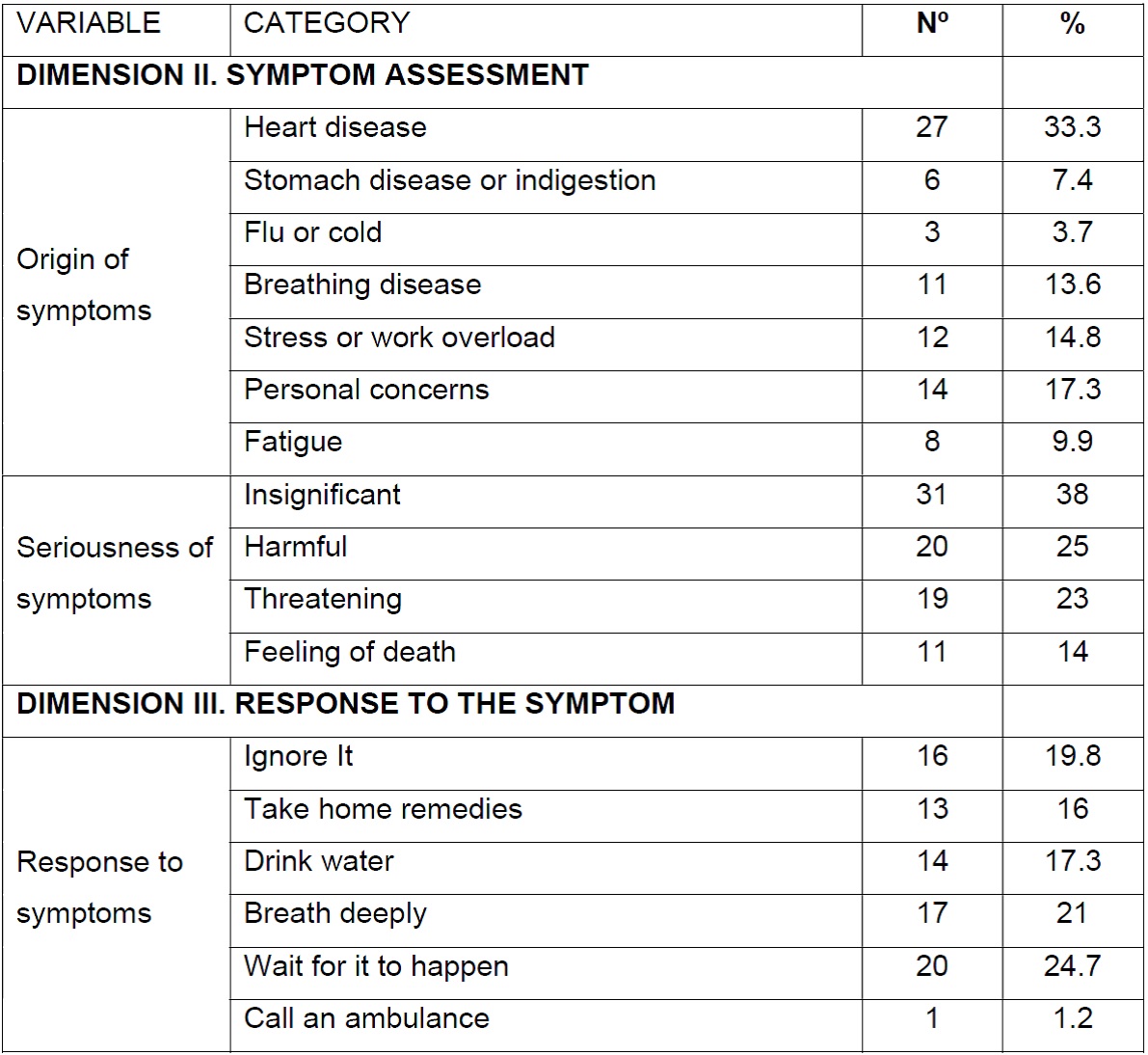
Regarding the evaluation of symptom origin, most related it to extra-cardiac conditions and only 3 out of 10 women related it to heart disease. In turn, response actions to symptoms were varied, highlighting waiting for it to finish and taking deep breaths as the most frequent actions performed by the patients (Table 4).
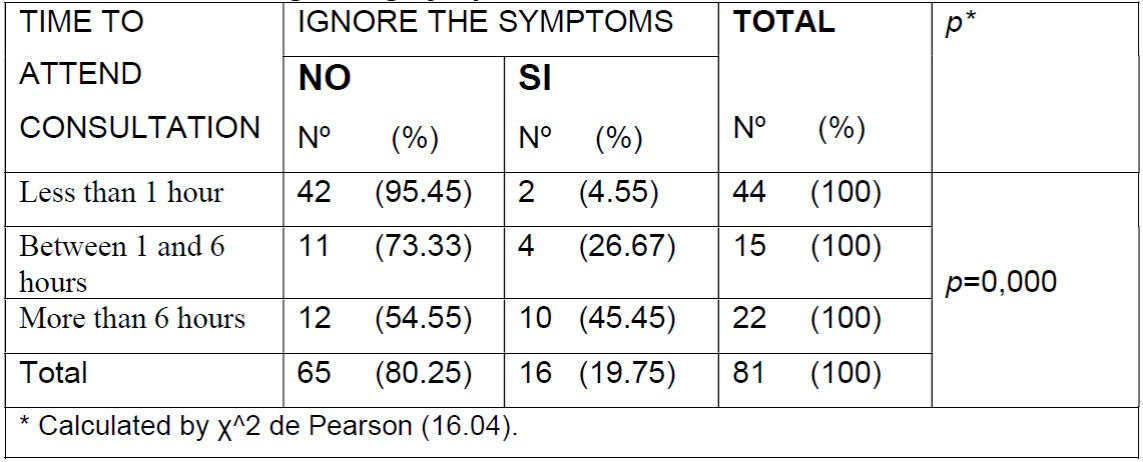
Finally, there was a statistically significant association between time of seeking professional help and low importance given to symptoms (p=0,000) (Table 5).
DISCUSSION
This investigation demonstrated the high number of risk factors for cardiovascular disease present in women with ACS. High blood pressure as the main modifiable risk factor for CVD found in the present study was 75,3%, coinciding with the results of research carried out in other contexts 70,5%15 y 75%.16 This increases stress on the arterial wall and exacerbates endothelial dysfunction, conditioning the appearance of ischemic heart disease in older people, more frequently in women.9
Regarding behavioral risk factors, excessive consumption of carbohydrates, sedentary lifestyle, overweight, and smoking were found in a high percentage. Which is similar to what was reported by the American Heart Association (AHA), who affirm that 76.3% of Hispanic American women are overweight or obese and 57.1% do not meet the guidelines of the physical activity guidelines.17 INTERHEART study shows that the union of smoking, high blood pressure, and diabetes increase the probability of AMI, showing statistical significance (p <0,0001).18
Prevalent medical diagnosis of AMI (78%) found in this study differs from unsTable angina (59%) reported by Noureddine et al.16 For its part, Reynolds et al found that the female sex was independently associated with a higher frequency of angina (odds ratio, 1.41; IC 95%, 1.13 - 1.76).19
Most of the sample (97.5%) presented menopause as the main risk factor that was not modifiable. In this regard, Saldarriaga et al. detected that only 63% of women in their first coronary event had this risk factor.20 Parvand et al.21 in 2018, through a review of the literature, identified menopause as a risk factor for coronary heart disease; like Isiadinso and Shaw describe that the risk in women increases 10 years after the onset of menopause, early menarche and premature menopause; associated factors with an increased risk of coronary heart disease.22
In relation to the perception of the symptom, 85% reported pain or discomfort in any part of the chest as the most frequent symptom, with lower percentages showing the presence of anguish, palpitations and unusual fear, among others. It is usual for women with ACS to present a variety of symptoms and to a greater extent those called atypical. 1
In a study carried out in Germany, the multivalent logistic regression found that women present atypical symptoms such as pain between the scapulae, sore throat, nausea, vomiting, and fear of death.23 For their part, Lichtman et al. identified that 61.9% of women had 3 or more symptoms associated with non-chest pain.11 For this purpose, Smith et al. reports that women are more likely to have atypical symptoms such as nausea, diaphoresis, fatigue, and pain in the arm or back.24
Regarding the evaluation of the symptom, 33.3% of the participants associated the symptoms with heart diseases; while most of them associated them with extra-cardiac conditions. In a study carried out in the United States with young women aged 18 to 55 years hospitalized for AMI, it was found that 54.7% associated their symptoms with extra-cardiac conditions, highlighting indigestion or acid reflux, stress and anxiety in a greater proportion.25 Another study conducted in China reported that 50.9% of the patients believed that it was a heart attack; the remaining percentage attribute the symptoms to stress / anxiety, indigestion, respiratory disease, hiatal hernia / gallbladder or other diseases.26
About the response to symptoms of ACS, 16% of the women in this study self-medicated with home remedies. A study carried out in the same direction found that 33% of Norwegian patients self-medicated, as a measure of initial response to ACS symptoms.27 In another study, 32% of women reported to another person, 18% self-medicated, 21% relaxed, 16% took herbal tea, and only 5% requested an ambulance.16 On the subject, Bjørnnes et al. they concluded that women tend to deny or rationalize their symptoms, resort to self-medication, consult others, and delay seeking medical attention; meanwhile the symptoms get worse.28
83% of women present with ACS symptoms at home, a condition that may be associated with response to symptoms and delay in seeking professional help.16,29 The late start of treatment against ACS is directly related to morbidity and mortality burden of cardiovascular diseases; due to the fact that a significant number of women seeking care late, they present life-threatening complications that become determining factors of infarct size and cardiac function, which reduce the possibility of being beneficiaries of definitive treatment such as angioplasty or therapy thrombolytic.1
In this study, the delay time or time variable for decision-making regarding seeking professional help after symptoms started was less than one hour in half of the participants; 27% took more than six hours. In this regard, Soto reported that 74.9% of women took more than 12 hours to request health care and the delay time was an obstacle to starting timely treatment.30 A Norwegian study identified that more than 56% of ACS participants took more than an hour to seek professional help and 21% took more than six hours.27
Overview, while deciding to seek care help, home-based measures are taken to manage symptoms, with the consequent loss of valuable time.1 In the case at hand, the delay in reaching the emergency department was less than one hour in 91% of cases. On this aspect, Sari et al. report that only 31% of patients with AMI arrived at hospital in the first 60 minutes after the onset of symptoms;31 while another study reveals that the average hospital attendance was 3.2 hours and 38.7% of women took more than 6 hours.11 This finding is corroborated by Lichtman et al.32 and McSweeney et al.33, who indicate that women are less likely than men to seek prompt treatment.
In summary, there is a significant association between the time that elapses between the onset of symptoms and the search for health care. Consequently, women are required to recognize the importance of symptoms and seek immediate professional help, for which the design of education, information and communication programs, with a preventive approach, is necessary.1
It follows from the above, that women underestimate the symptoms, which puts them at imminent risk. Hence the need to provide education, information and timely search for symptoms, since the goal for Nursing from this theoretical approach should be to avoid or delay a negative result. Proper management begins with the evaluation of the experience of symptoms from the person's perspective, the objective of this study. Future research aimed at identifying relevant, useful, and timely intervention strategies is required.
CONCLUSIONS
Women with ACS have multiple risk factors for cardiovascular disease. The presence of high blood pressure, dyslipidemia, sedentary lifestyle and unhealthy diet stand out among the modifiable ones. In turn, menopause and age over 65 years within the non-modifiable; they directly affect the probability of presenting occlusion of the coronary arteries.
The role of caregiver at home, low socioeconomic level and limited educational level, they translate into factors that condition the response to symptoms and late times in which women decide to seek professional care; which is directly related to the presence of complications when receiving inopportune care, consistent with the literature.
Women during the ACS event perceive diversity of symptoms, in a greater proportion atypical, highlighting pain or discomfort anywhere in the chest. By itself, only a third party of patients associate them with heart disease, downplaying them; leading to inappropriate behaviors such as waiting, self-medication and, in the worst case, ignoring them.
From what is described in the preceding paragraphs, the importance of understanding, from the women's perspective, the perception, evaluation, and response to ACS symptoms is denoted, which requires comprehensive and participatory interventions that involve the community, staff health and health service administrators.
REFERENCIAS
1. Mehta LS, Beckie TM, DeVon HA, Grines CL, Krumholz HM, Johnson MN, et al. Acute Myocardial Infarction in Women?: A Scientific Statement from the American Heart Association. Vol. 133, Circulation. Lippincott Williams and Wilkins; 2016. p. 916-47. [ Links ]
2. Wang H, Naghavi M, Allen C, Barber RM, Carter A, Casey DC, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016 Oct 8;388(10053):1459-544. [ Links ]
3. Organizacion Mundial de la Salud. OMS | Enfermedades no transmisibles [Internet]. Who. 2015 [cited 2019 Jul 18]. p. Notas Descriptivas. Available from: https://www.who.int/es/news-room/fact-sheets/detail/noncommunicable-diseases [ Links ]
4. World Health Congress of Cardiology and Cardiovascular. El costo de las enfermedades cardiacas en América Latina. In: El costo de las enfermedades cardiacas en América Latina. Mexico City; 2016. p. 3. [ Links ]
5. Social M de S. Análisis de Situación de Salud. Colombia, 2017 [Internet]. Imprenta Nacional de Colombia. 2018 [cited 2020 Mar 29]. Available from: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/ED/PSP/asis-nacional-2017.pdf [ Links ]
6. Lobos Bejarano JM, Brotons Cuixart C. Factores de riesgo cardiovascular y atención primaria: evaluación e intervención. Aten Primaria. 2011 Dec 1;43(12):668-77. [ Links ]
7. Rhee E-J Prevalence and Current Management of Cardiovascular Risk Factors in Korean Adults Based on Fact Sheets. Endocrinol Metab [Internet]. 2020 Mar 1 [cited 2020 Mar 28];35(1):85. Available from: https://synapse.koreaMedorg/DOIx.php?id=10.3803/EnM.2020.35.1.85 [ Links ]
8. Murphy E. Estrogen signaling and cardiovascular disease. Vol. 109, Circulation Research. NIH Public Access; 2011. p. 687-96. [ Links ]
9. Kane AE, Howlett SE. Differences in cardiovascular aging in men and women. In: Advances in Experimental Medicine and Biology. Springer New York LLC; 2018. p. 389-411. [ Links ]
10. López Martínez T, Prieto García E, de Dios del Valle R. MUJERES Y HOMBRES FRENTE AL SÍNDROME CORONARIO AGUDO. Enfermería en Cardiol. 2012;57(57):33-9. [ Links ]
11. Lichtman JH, Leifheit EC, Safdar B, Bao H, Krumholz HM, Lorenze NP, et al. Sex differences in the presentation and perception of symptoms among young patients with myocardial infarction. Circulation [Internet]. 2018 Feb 20 [cited 2019 Jan 2];137(8):781-90. Available from: https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.117.031650 [ Links ]
12. Björck L, Nielsen S, Jernberg T, Zverkova-Sandström T, Giang KW, Rosengren A. Absence of chest pain and long-term mortality in patients with acute myocardial infarction. Open Hear. 2018 Nov 1;5(2). [ Links ]
13. Bernal Cárdenas CY, Céspedes-Cuevas VM, Sanhueza-Alvarado OI. Modelo conceptual del manejo del síntoma: evaluación y crítica. Aquichan [Internet]. 2018 [cited 2020 Mar 25];18(3):311-26. Available from: https://aquichAnunisabana.edu.co/index.php/aquichan/article/view/8574/4846 [ Links ]
14. Céspedes Cuevas VM. Atypical nature of coronary artery disease in women: a proposal for measurement and classification. Av en Enfermería [Internet]. 2015 Aug 5 [cited 2020 Mar 26];33(1):10-8. Available from: https://revistas.unal.edu.co/index.php/avenferm/article/view/47855 [ Links ]
15. Olivencia Peña L, Bueno Cavanillas A, Soto Blanco JM, Yuste Ossorio ME, Barranco Ruiz F. Síndrome coronario agudo en la mujer. Diferencias de género. Med Clin (Barc) [Internet]. 2011 Nov [cited 2018 Oct 10];137(14):623-30. Available from: http://linkinghub.elsevier.com/retrieve/pii/S002577531100830X [ Links ]
16. Noureddine S, Arevian M, Adra M, Puzantian H. Response to signs and symptoms of acute coronary syndrome: Differences between Lebanese men and women. Am J Crit Care [Internet]. 2008 Jan 1 [cited 2019 Jan 3];17(1):26-35. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18158386 [ Links ]
17. Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart disease and stroke statistics-2015 update?: A report from the American Heart Association. Circulation. 2015 Jan 27;131(4):e29-39. [ Links ]
18. Yusuf PS, Hawken S, Ôunpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet [Internet]. 2004 Sep [cited 2018 Dec 30];364(9438):937-52. Available from: http://linkinghub.elsevier.com/retrieve/pii/S0140673604170189 [ Links ]
19. Reynolds HR, Shaw LJ, Min JK. Association of Sex With Severity of Coronary Artery Disease , Ischemia , and Symptom Burden in Patients With Moderate or Severe Ischemia Secondary Analysis of the ISCHEMIA Randomized Clinical Trial. JAMA cardiol. 2020; [ Links ]
20. Saldarriaga CI, Franco G, Garzón AM, García I, Mejía N, Restrepo A. Factores de riesgo para la enfermedad coronaria temprana en mujeres Biomédica [Internet]. 2010 Mar 3 [cited 2018 Dec 30];30(4):559-66. Available from: http://www.revistabiomedica.org/index.php/biomedica/article/view/294 [ Links ]
21. Parvand M, Rayner-Hartley E, Sedlak T. Recent Developments in Sex-Related Differences in Presentation, Prognosis, and Management of Coronary Artery Disease. Can J Cardiol. 2018;34(4):390-9. [ Links ]
22. Isiadinso I, Shaw LJ Diagnosis and risk stratification of women with sTable ischemic heart disease. J Nucl Cardiol. 2016;23(5):986-90. [ Links ]
23. Kirchberger I, Heier M, Golüke H, Kuch B, Von Scheidt W, Peters A, et al. Mismatch of presenting symptoms at first and recurrent acute myocardial infarction. from the MONICA/KORA Myocardial Infarction Registry. Eur J Prev Cardiol [Internet]. 2016 Mar 20 [cited 2019 Jan 2];23(4):377-84. Available from: http://journals.sagepub.com/doi/10.1177/2047487315588071 [ Links ]
24. Smith R, Frazer K, Hyde A, O'Connor L, Davidson P. "Heart disease never entered my head": Women's understanding of coronary heart disease risk factors. J Clin Nurs. 2018;27(21-22):3953-67. [ Links ]
25. Lichtman JH, Leifheit EC, Safdar B, Bao H, Krumholz HM, Lorenze NP, et al. Sex Differences in the Presentation and Perception of Symptoms Among Young Patients With Myocardial Infarction. Circulation [Internet]. 2018 Feb 20 [cited 2019 Jan 3];137(8):781-90. Available from: https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.117.031650 [ Links ]
26. An L, Li W, Shi H, Zhou X, Liu X, Wang H, et al. Gender difference of symptoms of acute coronary syndrome among Chinese patients: a cross-sectional study. Eur J Cardiovasc Nurs [Internet]. 2018 Dec 17 [cited 2019 Jan 2];147451511882048. Available from: http://journals.sagepub.com/doi/10.1177/1474515118820485 [ Links ]
27. Løvlien M, Schei B, Hole T. Prehospital delay, contributing aspects and responses to symptoms among Norwegian women and men with first time acute myocardial infarction. Eur J Cardiovasc Nurs [Internet]. 2007 Dec 23 [cited 2018 Dec 30];6(4):308-13. Available from: http://journals.sagepub.com/doi/10.1016/Jejcnurse.2007.03.002 [ Links ]
28. Bjørnnes AK, Parry M, Leegaard M, Ayala AP, Lenton E, Harvey P, et al. Self-Management of Cardiac Pain in Women: A Meta-Summary of the Qualitative Literature. Qual Health res 2018;28(11):1769-87. [ Links ]
29. Padilla García CI, Sáenz Montoya X. Respuestas de la mujer frente a los síntomas de Síndrome Coronario Agudo basados en el Modelo Conceptual del Manejo de los Síntomas. Av en Enfermería. 2014;32(1):102-13. [ Links ]
30. Soto MA. Factores que intervienen en la demora de la solicitud de atención médica o de enfermería en mujeres que presentan dolor torácico de origen coronario. Av enferm [Internet]. 2007 [cited 2020 Apr 2];25(2):58-64. Available from: https://www.researchgate.net/publication/282315871_Factores_que_intervienen_en_la_demora_de_la_solicitud_de_atencion_medica_o_de_enfermeria_en_mujeres_que_presentan_dolor_toracico_de_origen_coronario [ Links ]
31. Sari I, Acar Z, Özer O, Erer B, Tekbas E, Üçer E, et al. Factors associated with prolonged prehospital delay in patients with acute myocardial infarction Akut miyokard infarktüslü hastalarda hastaneye geç gelis ile iliskili faktörler [Internet]. Vol. 36, Türk Kardiyol Dern Ars-Arch Turk Soc Cardiol. 2008 [cited 2019 Jan 3]. Available from: https://www.journalagent.com/tkd/pdfs/TKDA_36_3_156_162.pdf [ Links ]
32. Lichtman JH, Leifheit-Limson EC, Watanabe E, Allen NB, Garavalia B, Garavalia LS, et al. Symptom recognition and healthcare experiences of young women with acute myocardial infarction. Circ Cardiovasc Qual Outcomes. 2015;8:S31-8. [ Links ]
33. McSweeney JC, Cleves MA, Fischer EP, Pettey CM, Beasley B. Using the McSweeney Acute and Prodromal Myocardial Infarction Symptom Survey to Predict the Occurrence of Short-Term Coronary Heart Disease Events in Women. Women's Heal Issues. 2017;27(6):660-5. [ Links ]
Received: April 08, 2020; Accepted: July 05, 2020
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
