










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.20 no.63 Murcia jul. 2021 Epub 02-Ago-2021
https://dx.doi.org/10.6018/eglobal.449531
Originals
Symptom Burden, Comorbidity and Functional Status of patients with Chronic Kidney Disease Stage 5 managed conservately
1 Profesor Departamento de Enfermería y Podología. Universidad de Málaga. Málaga. España. danieltunie@hotmail.com
2 Médico responsable del Equipo de Soporte y Cuidados Paliativos Hospital de Manacor, Mallorca, Islas Baleares. Coordinador del Grupo de Estudio de Cuidados Paliativos Renales de la Sociedad Española de Nefrología (SEN). Miembro del Comité Técnico para la implementación de Cuidados Paliativos en Enfermedad Renal Crónica en Islas Baleares. Mallorca. España.
Objective:
To determine the prevalence and severity of symptoms of patients with Chronic Kidney Disease Stage 5 managed conservately, and their association with the comorbidities and functional status.
Methods:
A cross-sectional, descriptive, and correlational design was used. Symptom data were collected using the Spanish modified version of Palliative care Outcome Scale-Symptoms Renal. Comorbidity was collected and scored according to the modified Charlson Comorbidity Index. For the evaluation of functional status, the Barthel index was used.
Results:
60 patients were included in this study. More than 50% of patients described weakness, pain, difficulty for sleeping, poor appetite and mouth problems. Diabetes, coronary artery disease, and peripheral vascular disease, and tumor, were the main comorbid conditions of these patients. The mean score of Barthel index was 88±14.2. There was no significant correlation between comorbidities and symptoms (p=0.43). There was a significant correlation between symptoms and functional decline (p=0.001).
Conclusions:
Patients with Chronic Kidney Disease Stage 5 experience a high level of symptom burden. Weakness was the most prevalent symptom in this sample population. Symptom burden correlated with functional decline. Further longitudinal studies are needed that analyse the impact of symptoms and their management in this population.
Keywords: Advanced Chronic Kidney Disease; Symptoms assessment; Outcome measure; Palliative care
INTRODUCTION
Chronic Kidney Disease (CKD) is a problem whose incidence and prevalence have increased in recent years globally 1. In Spain, the prevalence of Advanced Chronic Kidney Disease (ACKD) (defined as stage 4-5 of CKD with a glomerular filtration rate (GFR) <30 ml / min for at least three months) exceeds 1.000 patients per million inhabitants 2,3.
Patients with CKD stage 5 suffer a wide variety of physical and psychological symptoms with high cost of care and which also negatively affect quality of life 4)(5)(6. In this sense, nurses play an essential role in the evaluation and management of the patient's symptoms in this population 7. Uncontrolled symptoms in this population contribute to increased suffering and symptomatic management is a priority 8)(9)(10)(11. In this context, the collaboration of professionals in the areas of Nephrology and Palliative Care (PC) can have a positive effect on the quality of life of patients and their families 10. In this sense, patients with CKD stage 5 can benefit from PCs, especially those patients under conservative kidney management (CKM) 11. Along these lines, CKM is considered a reasonable option for those patients with high comorbidity, advanced age, and who do not wish to start dialysis 10,11.
There is little evidence on on the prevalence of symptoms in patients in CKM in Spain culture, so this aspect should be investigated 12.
The objectives of this study were to: (1) describe the prevalence and severity of symptoms in patients with CKD stage 5 (GFR <15 ml / min) in CKM, 2) explore the association between symptomatology and comorbidity; and (3) explore the association between symptoms and functional status.
METHOD
Participants and Procedure
Descriptive, correlational, cross-sectional study. All the data used in this study were obtained from a large sample of patients with ACKD as part of a larger study in which a cross-cultural adaptation and validation of an instrument for measuring symptoms in this population was carried out. In the present study, a descriptive analysis of the prevalence and severity of symptoms, comorbidity and functional status of patients with CKD stage 5 in CKM was performed. In addition, the association of symptoms with comorbidity and functional status was explored.
The patients were recruited from the Nephrology Service of the Regional University Hospital of Malaga. The study data were collected between the months of April and September 2015.
The inclusion criteria were: (1) Spanish-speaking adult patients with CKD stage 5 (GFR <15 ml / min) in CKM; and (2) written informed consent. Patients with cognitive impairment and those under 18 years of age were excluded.
The patients were informed about the study and subsequently a written informed consent was obtained. Sociodemographic and clinical data were collected during the interviews that took place in the ERCA consultation.
Instruments
Spanish modified version of the Palliative care Outcome Scale-Symptoms Renal (POS-S Renal)
The original version of this instrument was designed to measure symptomatology in patients with ACKD, and assesses 17 symptoms 13. This original version has been translated and adapted into Spanish and has proven to be a valid and reliable instrument in the evaluation of symptoms in ACKD (14). In this sense, the questionnaire showed adequate psychometric properties in terms of structural validity, test-retest reliability and criterion validity (14). A new item was added to the modified Spanish version of the POS-S Renal (cramps). As a result, the modified Spanish version of this questionnaire contains 18 symptoms, and can be completed by the patient 14.
Modified Charlson comorbidity index (mCCI)
To assess comorbidity, the modified Charlson comorbidity index (mCCI) was used 15. The mCCI is a valid and reliable comorbidity index that has been widely used in the renal population. The mCCI contains 19 comorbid conditions, which are scored from 1 to 6, adding a score of 1 for each decade from the age of 40 (15). In this modified version, the item "acute myocardial infarction" has been replaced by "cardiovascular disease" 15. An mCCI score greater than or equal to 8 is considered to be highly predictive of mortality 15.
Barthel index
To assess functional capacity, the Barthel index 16 was used. The Barthel index is a valid and reliable instrument that has been widely used in the renal population 17,18. This instrument assesses the patient's independence with respect to ten basic activities of daily life: feeding, personal hygiene, dressing, grooming, stool, urination, use of the toilet, transfers, ambulation, and climbing stairs 16. The score for each activity is different, assigning a score of 0, 5, 10 or 15 points. The total score ranges from 0 (total dependence) to 100 points (independence) 16.
Statistical analysis
A descriptive analysis of the sociodemographic and clinical variables of the population was carried out. Mean and standard deviation were used for continuous variables and percentages for categorical variables.
To describe the symptoms, percentages and 95% confidence interval (CI) were used. The Kolmogorov-Smirnov test was performed to determine the distribution of the sample. Pearson's correlation coefficient was used to explore the relationship of the symptoms with the comorbidity and functional status of the patient. The value of p <0.05 was taken as statistically significant. Analyzes were performed using SPSS version 24 statistical software.
Ethical aspects
This study has been approved by the Provincial Ethics Committee of Málaga. The standards of good clinical practice and the ethical principles established for research on human beings, in accordance with the Declaration of Helsinki and its subsequent revisions, were maintained at all times.
The clinical data was separated from the personal identification data and the databases were encrypted and stored on devices specifically reserved for this project. Prior to participation in the study, the caregivers received information on the content and scope of the study and gave their written consent.
RESULTS
Characteristics of the sample
60 patients with CKD stage 5 in CKM were included in this study. The sociodemographic and clinical characteristics are shown in Table 1. The missing values were less than 2%. The mean mCCI was 6.2 ± 2.2 and the main comorbid conditions were: diabetes, ischemic heart disease, neoplasms, and peripheral vascular disease (Table 2). The mean Barthel index was 88 ± 14.2 (Table 3).
Table 1. Sociodemographic and Clinical Characteristics of the Sample (N=60)
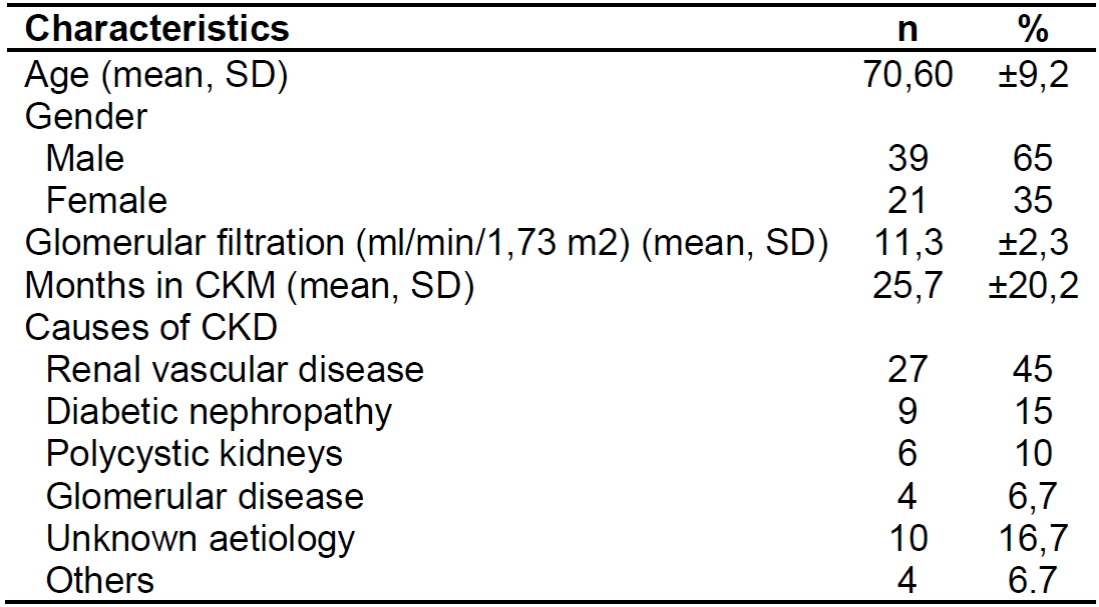
Source: Research data
Values represent frequency (n), percentage (%) or mean (SD)
Table 2. mCCI and Prevalence of Comorbid Conditions (N=60)
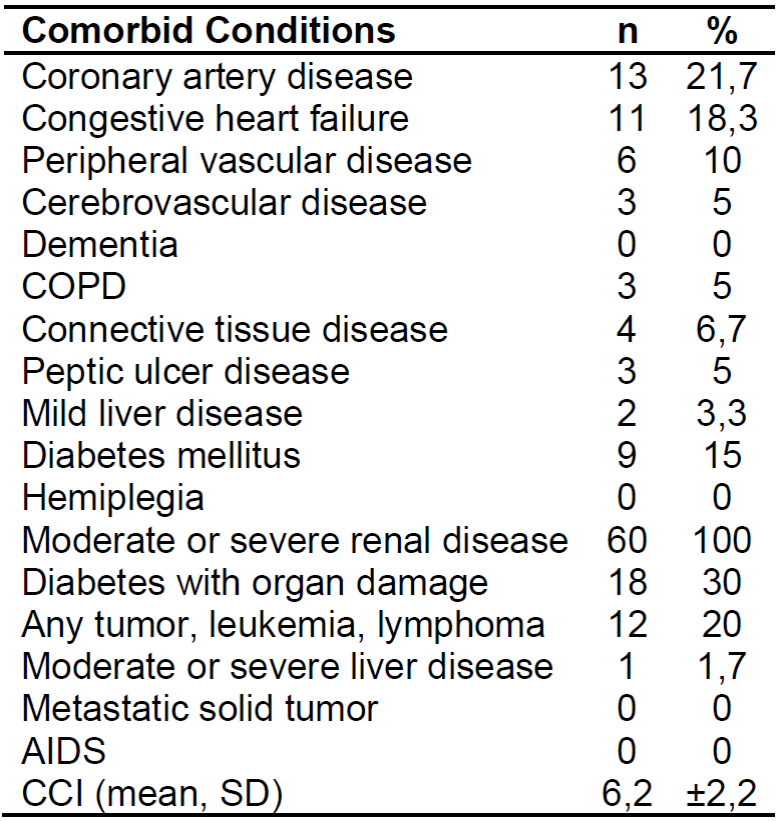
Source: Research data
Values represent frequency (n), percentage (%) or mean (SD)
Table 3. Barthel index and dependency levels (N=60)
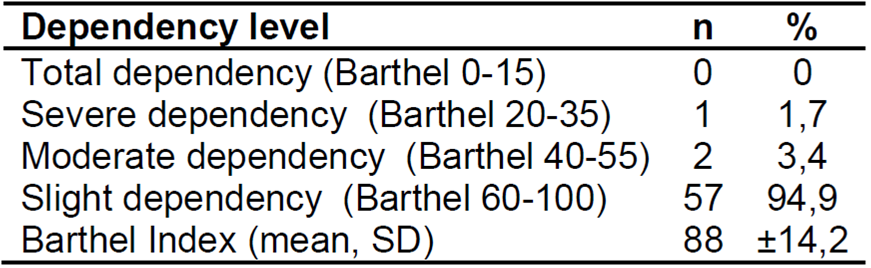
Source: Research data
Values represent frequency (n), percentage (%) or mean (SD)
Prevalence and severity of symptoms
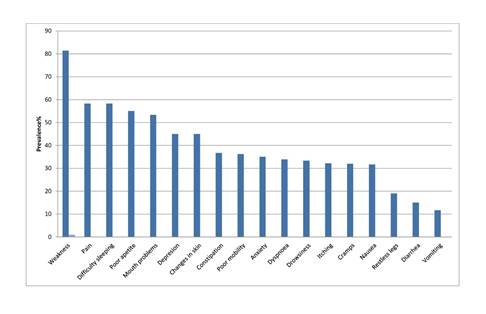
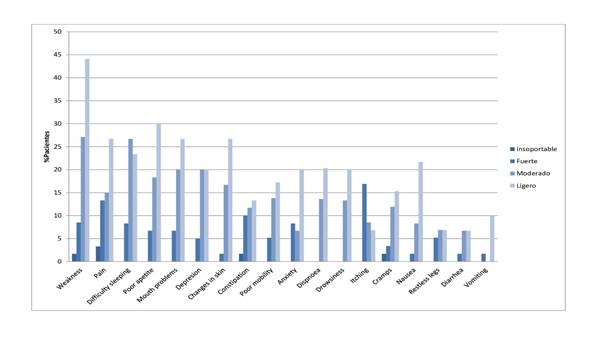
The most frequent symptoms were: weakness - 81.4% (CI: 71-92%), pain - 58.3% (CI: 42-69%), difficulty sleeping - 58.3% (CI: 48-75 %), poor appetite - 55% (CI: 40-67%), mouth problems - 53.3% (CI: 35-60%), depression - 45% (CI: 33-60%), changes in skin - 45% (CI: 29-56%), constipation 36.7% (CI: 24-50%), poor mobility - 36.2% (CI: 24-50%), anxiety - 35% (CI : 24-50%), dyspnea - 33.9% (CI: 20-46%), drowsiness - 33.3% (CI: 24-50%), itching - 32.2% (CI: 22-48% ), cramps - 32% (CI: 20-46%) and nausea - 31.7% (CI: 19-44%). The prevalence of symptoms is shown in Figure 1.
The mean number of symptoms suffered per patient was 6.7 ± 3.6 out of a maximum of 18, with a range of 0-15 symptoms per patient. The most intense symptoms (from severe to unbearable) were: pain, weakness, constipation and itching (Figure 2).
Association Between Symptoms and Comorbidities
The association between symptomatology and comorbidity was evaluated. The results indicated that there was no significant correlation between symptom burden and comorbidity (r = 0.11, p = 0.43).
Association Between Symptoms and Functional Status
The association between symptoms and functional status of the patient was also evaluated. The results obtained indicated that there was a negative association between symptom burden and functional status (r = -0.48, p = 0.001), and therefore the symptom burden was higher in those patients with worse functional status.
DISCUSSION
Symptoms in patients with CKD stage 5 in CKM is considered a difficult construct to measure, since it is determined by physical and psychological aspects, and is influenced by factors such as renal failure itself, comorbidity or treatment 5)(19)(20. Furthermore, symptoms in this population do not present in isolation, but rather in the form of groups of symptoms 21. In this sense, conducting studies that address symptomatology in this population allows optimizing symptomatic management.
To our knowledge, this is the first study carried out in Spain that analyzes the prevalence and severity of symptoms in 5 CKD stage in patients in CKM and its association with comorbidity and functional status.
The results of this study indicate that patients with CKD stage 5 in CKM present a high burden of symptoms and comorbidity, although they maintain an accepTable functional status. Symptoms such as weakness (81.4%) and pain (58.3%) presented a high frequency in these patients. In addition, more than 50% of the patients presented weakness, pain, difficulty sleeping, poor appetite, and mouth problems, with pain and weakness among the most intense symptoms. These symptoms are consistent across studies and are associated with a poor quality of life 5)(6)(22.
Weakness is a frequent symptom in this population and is associated with other symptoms such as depression and sleep disorders. This symptom has an impact on the functional status of the patient, which suggests that an adequate management of the global symptomatic burden with a multidimensional approach, can improve the frequency and intensity of this symptom 23. In this study, weakness was the most frequent and intense symptom. These findings were comparable to those described in other studies 5)(19)(23.
Pain continues is a prevalent symptom in this population. The etiology of pain in is usually related to vascular-ischemic problems, peripheral neuropathy, and muscular and osteoarticular problems 24. In addition, pain is also related to other symptoms such as insomnia and depression, and also has an effect on the functional status of the patient 25. In this study, pain was the second most frequent and intense symptom. These results are comparable to those described in other studies 5,19.
Regarding the association between symptoms and comorbidity, no significant correlation was found (p = 0.43). These findings were comparable to those described in other studies 21.
Regarding the association between symptoms and functional status, a negative and significant association was found (p = 0.001), which indicates that the burden of symptoms was higher in those patients with worse functional status. In this sense, the symptomatic burden has a negative effect on the functional capacity and the level of dependency of this population 26.
Palliative care in this population can have a positive impact by optimizing the symptomatic management of these patients 27,28. Therefore, the principles of PC should be integrated in the Nephrology Services for patients with ACKD, especially in those in CKM (10-11). This is especially important in Spain, where the integration of PC principles in Nephrology Services is under development.
This study shows the value of symptoms evaluation with valid and reliable instruments such as the modified Spanish version of the POS-S Renal. This instrument provides the clinician with an optimal evaluation method of symptoms in ACKD 14. In this sense, nurses play an essential role in the evaluation and management of the patient's symptoms in CKM 7.
This study has several limitations. This is a cross-sectional study that has been carried out in a single center and therefore the results are not directly transferable to other centers. In this regard, additional multicenter studies using a larger population are needed.
CONCLUSIONS
Patients with CKD stage 5 in CKM suffer a high burden of symptoms that negatively affects the functional status of the patient. Weakness was the most frequent symptom in this population. Future studies on the impact of symptoms in these patients, as well as the interventions necessary for their optimal management should be considered.
REFERENCIAS
1. Bikbov B, Purcell CA, Levey AS, Smith M, Abdoli A, Abebe M, et al. Global, regional, and national burden of chronic kidney disease, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet. 2020 Feb 29;395(10225):709-33. Disponible en: https://doi.org/10.1016/S0140-6736(20)30045-3 [ Links ]
2. Gorostidi M, Sánchez-Martínez M, Ruilope LM, Graciani A, de la Cruz JJ, Santamaría R, et al. Chronic kidney disease in Spain: Prevalence and impact of accumulation of cardiovascular risk factors. Nefrología (English Edition). 2018 Nov 1;38(6):606-15. Disponible en: https://doi.org/10.1016/j.nefroe.2018.04.010 [ Links ]
3. K/DOQI Clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J KidneyDis. 2002;39(2 Suppl1):1-266. [ Links ]
4. Davison SN, Levin A, Moss AH, Jha V, Brown EA, Brennan F, et al. Executive summary of the KDIGO Controversies Conference on Supportive Care in Chronic Kidney Disease: developing a roadmap to improving quality care. Kidney international. 2015;88(3):447-59.1. doi:10.1038/ki.2015.110 [ Links ]
5. Murtagh FE, Addington-Hall J, Edmonds P, Donohoe P, Carey I, Jenkins K, et al. Symptoms in the month before death for stage 5 chronic kidney disease patients managed without dialysis. J Pain Symptom Manage. 2010 Sep;40(3):342-52. Disponible en: https://doi.org/10.1016/j.jpainsymman.2010.01.021 [ Links ]
6. Abdel-Kader K, Unruh ML, Weisbord SD. Symptom burden, depression, and quality of life in chronic and end-stage kidney disease. Clinical journal of the American Society of Nephrology : CJASN. 2009;4(6):1057-64. Disponible en: https://doi.org/10.2215/CJN.00430109 [ Links ]
7. Barrett BJ, Garg AX, Goeree R, Levin A, Molzahn A, Rigatto C, et al. A Nurse-coordinated Model of Care versus Usual Care for Stage 3/4 Chronic Kidney Disease in the Community: A Randomized Controlled Trial. Clin J Am Soc Nephrol. 2011 Jun;6(6):1241-7. Disponible en: https://doi.org/10.2215/CJN.07160810 [ Links ]
8. Steinhauser KE, Christakis NA, Clipp EC, McNeilly M, McIntyre L, Tulsky JA. Factors considered important at the end of life by patients, family, physicians, and other care providers. JAMA. 2000;284(19):2476-82. [ Links ]
9. Manns B, Hemmelgarn B, Lillie E et al. Setting research priorities for patients on or nearing dialysis. Clin J Am Soc Nephrol 2014; 9: 1813-1821. Disponible en: https://doi.org/10.2215/CJN.01610214 [ Links ]
10. Leiva-Santos JP, Sánchez-Hernández R, García-Llana H, Fernández-Reyes MJ, Heras-Benito M, Molina-Ordas Á, et al. Cuidados de soporte renal y cuidados paliativos renales: revisión y propuesta en terapia renal sustitutiva. Nefrología (Madrid). 2012;32(1):20-7. Disponible en: http://scielo.isciii.es/scielo.php?script=sci_abstract&pid=S0211-69952012000100005&lng=es&nrm=iso&tlng=es [ Links ]
11. Brown MA, Crail SM, Masterson R, Foote C, Robins J, Katz I, et al. ANZSN renal supportive care 2013: opinion pieces [corrected]. Nephrology (Carlton). 2013 Jun;18(6):401-54. Disponible en:https://doi.org/10.1111/nep.12065 [ Links ]
12. Gutiérrez Sánchez D, Leiva-Santos JP, Sánchez-Hernández R, Gómez García R. Prevalencia y evaluación de síntomas en enfermedad renal crónica avanzada. Enfermería Nefrológica. 2015 Sep;18(3):228-36. Disponible en: https://doi.org/10.4321/S2254-28842015000300010 [ Links ]
13. Murphy EL, Murtagh FEM, Carey I, Sheerin NS. Understanding symptoms in patients with advanced chronic kidney disease managed without dialysis: use of a short patient-completed assessment tool. Nephron Clinical Practice. 2009;111(1):74-80. Disponible en: https://doi.org/10.1159/000183177 [ Links ]
14. Gutiérrez-Sánchez D, Leiva-Santos JP, Sánchez-Hernández R, Hernández-Marrero D, Cuesta-Vargas AI. Spanish modified version of the palliative care outcome scale-symptoms renal: cross-cultural adaptation and validation. BMC Nephrol. 2016 Nov 18;17(1):180. Disponible en: https://doi.org/10.1186/s12882-016-0402-8 [ Links ]
15. Beddhu S, Bruns FJ, Saul M, et al. A simple comorbidity scale predicts clinical outcomes and costs in dialysis patients. Am J Med 2000;108(8):609-13. Disponible en: https://doi.org/10.1016/S0002-9343(00)00371-5 [ Links ]
16. Mahoney FI, Barthel DW. FUNCTIONAL EVALUATION: THE BARTHEL INDEX. Maryland State Medical Journal. 1965 Feb;14:61-5. [ Links ]
17. Andreu Periz L, Andreu-Periz L, Puig Llobet M, Puig-Llobet M, Cases Amenós A, Cases-Amenós A. Grado de dependencia de las personas sometidas a hemodiálisis en Cataluña y evolución de su mortalidad. Nefrología. 2012 Sep 1;32(5):613-21. Disponible en: https://doi.org/10.3265/Nefrologia.pre2012.Jun.11460 [ Links ]
18. Cook WL, Jassal SV. Functional dependencies among the elderly on hemodialysis. Kidney International. 2008 Jun 1;73(11):1289-95. Disponible en: https://doi.org/10.1038/ki.2008.62 [ Links ]
19. Murtagh FEM, Addington-Hall JM, Edmonds PM, Donohoe P, Carey I, Jenkins K, et al. Symptoms in advanced renal disease: a cross-sectional survey of symptom prevalence in stage 5 chronic kidney disease managed without dialysis. J Palliat Med. 2007 Dec;10(6):1266-76. Disponible en: https://doi.org/10.1089/jpm.2007.0017 [ Links ]
20. Gutiérrez Sánchez D, Leiva-Santos JP, López M, José M, Vargas C, I A. Perfil sintomático de los pacientes con Enfermedad Renal Crónica Estadio 4 y 5. Enfermería Nefrológica. 2017 Sep;20(3):259-66. Disponible en: https://doi.org/10.4321/s2254-28842017000300010 [ Links ]
21. Gutiérrez Sánchez D, Leiva-Santos JP, Cuesta-Vargas AI. Symptom Burden Clustering in Chronic Kidney Disease Stage 5. Clin Nurs Res. 2017 Nov 1;1054773817740671. Disponible en: https://doi.org/10.1177/1054773817740671 [ Links ]
22. Murtagh FEM, Addington-Hall J, Higginson IJ. The prevalence of symptoms in end-stage renal disease: a systematic review. ACKD2007;14(1):82-99. Disponible en: https://doi.org/10.1053/j.ackd.2006.10.001 [ Links ]
23. Almutary H, Douglas C, Bonner A. Multidimensional symptom clusters: an exploratory factor analysis in advanced chronic kidney disease. J Adv Nurs. 2016 Oct;72(10):2389-400. Disponible en: https://doi.org/10.1053/j.ackd.2006.10.001 [ Links ]
24. Davison SN, Koncicki H, Brennan F. Pain in chronic kidney disease: a scoping review. Semin Dial. 2014 Mar;27(2):188-204. Disponible en: https://doi.org/10.1111/sdi.12196 [ Links ]
25. Davison SN, Jhangri GS. Impact of pain and symptom burden on the health-related quality of life of hemodialysis patients. JPSM. 2010 Mar;39(3):477-85. Disponible en: https://doi.org/10.1016/j.jpainsymman.2009.08.008 [ Links ]
26. Weiner DE, Seliger SL. Cognitive and Physical Function in Chronic Kidney Disease. Curr Opin Nephrol Hypertens. 2014 May;23(3):291-7. Disponible en: https://doi.org/10.1097/01.mnh.0000444821.87873.7b [ Links ]
27. Tamura MK, Meier DE. Five policies to promote palliative care for patients with ESRD. Clin J Am Soc Nephrol 2013; 8: 1783-1790. Disponible en: https://doi.org/10.2215/CJN.02180213 [ Links ]
28. Kurella Tamura M, O'Hare AM, Lin E, Holdsworth LM, Malcolm E, Moss AH. Palliative Care Disincentives in CKD: Changing Policy to Improve CKD Care. American Journal of Kidney Diseases: The Official Journal of the National Kidney Foundation. 2018;71(6):866-73. Disponible en: https://doi.org/10.1053/j.ajkd.2017.12.017 [ Links ]
Received: October 08, 2020; Accepted: January 16, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
