










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.20 no.63 Murcia jul. 2021 Epub 02-Ago-2021
https://dx.doi.org/10.6018/eglobal.446241
Originals
Incidence, characteristics and measures applied in patients with influenza A virus (H1N1) in the hospital context during the 2016-2018 period
1aServicio de Urgencias del Hospital Universitario de Bellvitge. Barcelona. España. marina.ignaciotorres@gmail.com
1bInstituto de Investigación Biomédica de Bellvitge (IDIBELL). Barcelona. España.
2a Departamento de Control de Infección, Hospital Universitario de Bellvitge. Barcelona. España.
2bInstituto de Investigación Biomédica de Bellvitge (IDIBELL). Barcelona. España.
3a Departamento de Gestión del Conocimiento y Sistemas de Información en Enfermería, Hospital Universitario de Bellvitge. Barcelona. España.
3bInstituto de Investigación Biomédica de Bellvitge (IDIBELL). Barcelona. España.
Introduction
The influenza virus causes seasonal epidemics worldwide and it is estimated that between 5 and 20% of the population suffers from influenza each year. The first cases of human infection caused by a new influenza A virus (H1N1) were confirmed in April 2009.
Objective and Method
In the epidemic period (week 40-20) of 2016-2018, a multicenter prospective descriptive observational study was carried out in two public hospitals in the southern metropolitan area of Barcelona in order to determine the incidence of positive patients in influenza A (H1N1), as well as the demographic and clinical-evolutionary characteristics of these patients, the timing of virus detection and measures applied for infection control.
Results:
The results of the present work indicate that the cumulative incidence of Influenza A during the study period was 233,68 per 100,000 inhabitants. Almost 90% of the patients had an underlying chronic conditions, mostly heart disease and respiratory pathology. Furthermore, 40% of the patients presented complications, mainly pneumonia. Treatment and days of isolation were according to standard recommendations.
Conclusion:
These findings show the high incidence of influenza A virus (N1H1) as well as the benefits that apports the infection control teams surveillance, monitoring the compliance with treatment and days of measures to avoid the transmission.
Key words: Influenza Virus A; Infection; Virology; prevalence; N1H1
INTRODUCTION
Influenza is an important health problem for the health system, both due to the associated morbidity and mortality and due to the economic and social impact it entails.
In April 2009, the first cases of human infection caused by a new influenza A (H1N1) virus were confirmed. The virus causing the new pandemic was the result of a recombination between a rearranged American porcine virus from 1997-1998, which in turn contained porcine, avian and human virus segments, and a Euroasian porcine virus containing avian virus segments 2.
On April 25, 2009, the World Health Organization (WHO) issued its first statement warning of the presence of an epidemic outbreak caused by a new influenza A (N1H1) virus in the US and Mexico, declaring a major international public health emergency. On April 27, the WHO raised the pandemic alert level to phase 4, after verifying human-to-human transmission capable of causing outbreaks at the community level. On April 29, the WHO changes the phase from 4 to 5, considering that there are cases with transmission between people in two countries of the same health region: the US and Mexico. On June 11, 2009, the WHO raised the alert for influenza A, to level 6, the maximum of the scale that conFigures a pandemic, after verifying the high and sustained transmission of the virus in the world. This fact has not occurred since 1968 with the Influenzavirus A subtype H3N2, known as the Hong Kong flu 3.
At the end of September 2009, Influenza A (H1N1) affected more than 343,298 people worldwide, causing 4,108 deaths 3. The incidence of national level hospitalized cases with confirmed influenza was 36 per 100,000 inhabitants; 9 admissions for every thousand diagnosed cases of flu syndrome, 8% of which caused stay in intensive care units. Mortality was 17 cases per 100,000 inhabitants, but among the cases of patients admitted to intensive care units, the mortality increased in more than 20% 1,4. In one of the Catalan public hospitals during the pandemic period, 1,144 patients with clinical suspicion of influenza A (H1N1) were treated in the emergency department, of which 44.8% (513 patients) required admission 2.
According to previous studies, approximately 26% of confirmed cases were hospitalized. As risk factors for complications, in addition to advanced age, pregnancy, asthma, pulmonary disease, heart disease, immunodeficiency and obesity appear as factors with the greatest impact 5.
On the one hand, many studies show the need for infection control teams in hospitals to prevent and early detect possible outbreaks of influenza A among patients and professionals in pandemic periods 5,6.
On the other hand, the evidence shows that the surveillance systems carried out by the infection control teams and the vaccination campaigns should continue after the pandemic period (7, in addition to the need to continue researching on the incidence and characteristics of patients affected by this virus.
OBJECTIVES
Main objective
To determine the incidence of positive patients for Influenza A (H1N1) in two tertiary hospitals in the 2016-2018 epidemic period.
Specific objectives
To determine the demographic and clinical-evolutionary characteristics of patients affected by the Influenza A (H1N1) virus.
To know the timing of the detection of Influenza A (H1N1) in the patients of the two hospitals included in the study.
To describe the measures applied by the infection control team of the Hospital Universitari de Bellvitge to patients positive by the Influenza A (H1N1).
METHODOLOGY
The study was carried out in two tertiary hospitals located in the southern metropolitan area of Barcelona. Both hospitals are a reference centers for the municipalities of Hospitalet and El Prat de Llobregat and a territorial tertiary reference center for the entire South axis of Catalonia. They have all the specialties, including oncology, except maternal and childcare.
An observational, descriptive, quantitative and prospective study was conducted from week 40 of 2016 to week 19 of 2018. During the pandemic period, the center's infection control team carries out an exhaustive follow-up of new cases of influenza A, establishing measures of treatment, follow-up and recommendation of care regarding isolation while the patient is hospitalized and produces an annual report with these data.
The inclusion criteria were patients diagnosed with influenza A (H1N1) virus with a positive PCR in the study period and that the diagnosis of influenza was made through RT-PCR by pharyngeal swab, tracheal aspirate or bronchial aspiration of secretions (BAS). For the selection of the sample, consecutive non-probabilistic sampling was used during the study period of all the patients who met the inclusion criteria.
Data was obtained prospectively through daily monitoring carried out by the infection control team. The variables were collected from the electronic medical record using the SAP® platform (Systems, Applications & Products, Waldorff, Germany). The main data collected were sociodemographic data (gender, age) and clinical-evolutionary variables (chronic conditions, Charlson index, days of admission, days in the detection of influenza, method of obtaining the smear, discharge diagnosis, PCR date, drug therapy, days of treatment, hospitalization unit, days of isolation and complications during admission). The patient was considered to be a carrier of the influenza A (H1N1) virus if, during the study period, a positive PCR was obtained from the patient and this one was analyzed in the laboratories of our participating centers.
This study did not require informed consent since the follow-up of patients with influenza is part of the usual practice of the center. The bioethical principles and current regulatory standards in clinical research and the principles established in the Declaration of Helsinki and its subsequent amendments were met. The treatment, communication and transfer of personal data of all participating subjects were in accordance with current legal regulations. The data was anonymized using a consecutive numerical code. This study was approved by the Ethics Committee for Clinical Research of the participating centers with code PR091 / 17.
The data analysis was carried out with the IBM SPSS version 25.0 program. A descriptive analysis of all the variables has been carried out. The adjustment variables were analyzed according to the type of variable and presented in Tables. Nominal categorical variables were described by the number of cases, the percentage with respect to the total by category and the number of missing data. Continuous variables that followed a normal distribution were described by the number of cases, the mean, and the standard deviation. Continuous variables that did not follow a normal distribution are described by the number of cases, the median, the first and the third quartiles.
RESULTS
During the study period, 146,353 patients were admitted, of which 341 were positive for Influenza A, the cumulative incidence during the two study periods was 233.68 cases per 100,000 inhabitants. In the first study period between weeks 40 and 20 of the years 2016-2017, the incidence was 124.35 cases per 100,000 inhabitants. In the second period of 2017-2018 the incidence was 109.33 cases per 100,000 inhabitants. Among the 341 positive PCR determinations, the majority method of detection was the pharyngeal smear in 95% of the cases, followed by nasal exudate / pus in 4.4% of the cases and ending with the BAS method in 0, 6%.
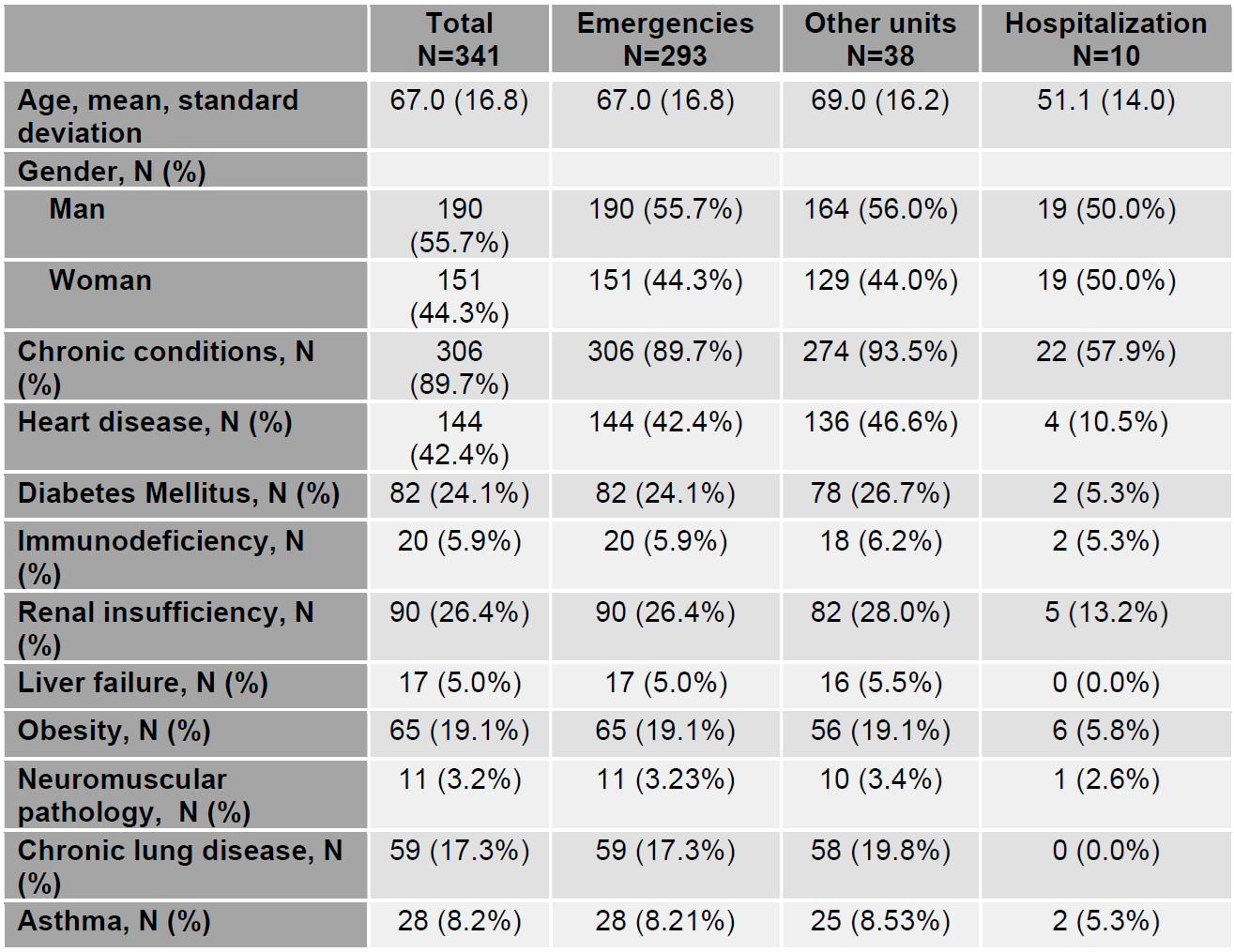
Of the total sample, 55.7% (n = 190) of the patients were men and the mean age was 67 years (standard deviation [SD] = 16.8). The median days of hospitalization was 5 days (interquartile range [IQR]: 3-10). Regarding the underlying chronic conditions, the results of this study determine that 89.7% of them had some associated comorbidity. Heart disease has been the most prevalent antecedent in 42.2% of patients, chronic renal failure in 26.4%, diabetes in 24.1%. Obesity (19.1%), lung disease (17.3%), and asthma (8.2%) were less prevalent comorbidities (Table 1). Based on the personal medical history of the patients studied, it has been determined that the median Charlson index in patients with positive Influenza A N1H1 was 2 points (Interquartile range [IQR] = 1.00; 3.00).
Table 1. Socio-clinical data of the patients affected by the N1H1 virus: Data according to the sample collection unit.
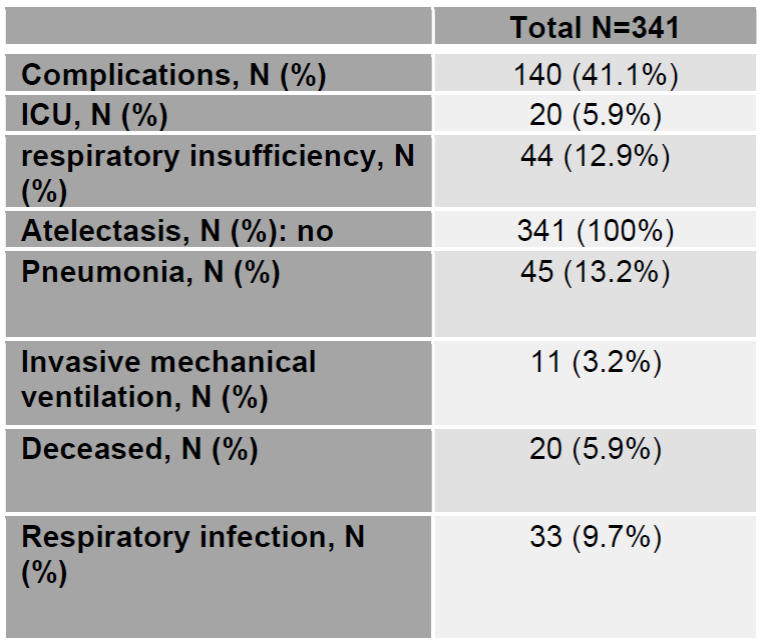
Regarding the complications suffered by patients with Influenza A (N1H1) in the study period, it should be noted that 41.1% of patients presented some type of complication. Among the most prevalent complications, pneumonia stands out in 13.2% of cases and respiratory failure in 12.9%, requiring admission to the ICU in 5.9%. (Table 2).
Table 2. Main complications of Influenza A (N1H1): Data according to the unit used to obtain the sample
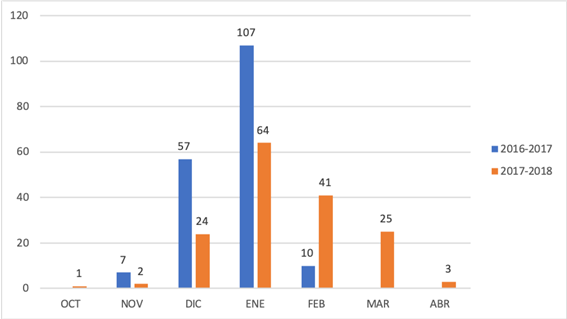
Regarding the timing of the detection of the N1H1 Virus, 86.5% of the cases were confirmed through swab with a positive PCR in the first 48 hours after the patient visited the hospital. The remaining 13.5% were considered nosocomial cases. The highest number of cases detected in both periods was between December and February (Graph 1). It should be noted that, during the study period, specific treatment was administered to 76.9% of confirmed influenza A patients in the first 48h, with a median of 4 days with contact and droplet transmission precautionary measures (IQR = 3-6).
DISCUSSION
According to the information plan for acute respiratory infections in Catalonia (PIDIRAC), in the 2016-2017 period, the incidence rate was 64.79 cases per 100,000 inhabitants 8. In our study, the incidence among patients who consulted the emergency room is higher, obtaining results of 124.35 cases per 100,000 inhabitants. In the 2017-2018 period, the incidence was 95.62 cases per 100,000 inhabitants 8), along the same lines, in this study an incidence rate of 109.33 cases per 100,000 inhabitants was obtained.
The results of this study indicate that the accumulated incidence of Influenza A during the study period was 233.68 cases per 100,000 inhabitants, results above the global incidence of Catalonia published in the PIDIRAC report, which they publish as the global incidence of both periods was 160.41 cases per 100.00 inhabitants. Furthermore, it is observed that the months where the greatest number of cases were detected was between December-February, as shown by previous studies 8. (see Graph 1)
It should be noted that, as reported in other studies, there are practically no differences in gender involvement 9. In relation to the chronic conditions, our study shows that approximately 90% of the patients had some urderlying disease. This data shows numbers above previous bibliography, as shown in the study by Bouned R, et al, where they publish a percentage of 70% 10. Previous cardiac disease was higher in incidence in our study, followed by renal and respiratory pathology. This data coincides with the results of a history of pulmonary origin published by Álvarez Lerma F, et al., with a percentage of affected people of 17.9% 11. Even so, this data is controversial since it does not coincide with other previously published studies where the approximate number of patients with risk factors was around 65% 5 and the most prevalent antecedent was obesity with an incidence of 34.8% 12.
Regarding respiratory complications, pneumonia and respiratory failure are the most prevalent. These results are in line with González's publication. R et al. where it is shown that respiratory complications are those with the highest incidence, occurring in 64.3% of cases 4). This data confirms the results of Álvarez Lerma F et al, where more than 34% of the patients required ventilatory support of some kind 11.
The detection of patients with influenza A was carried out in 86.5% of the cases in the first 48 hours after the patient's visit to the hospital due to flu symptoms. An immediate diagnosis and specific treatment with antivirals was administered in 76.9% of patients. These numbers are consistent with the literature already published by other authors of a diagnostic confirmation with a median of two days from the onset of symptoms and a slightly higher administration of antivirals corresponding to 87% of patients 4. As stated in the bibliography, treatment should begin when a positive sample is obtained, and a duration of 5 days is recommended 3.
Patients who required contact and droplet transmission precautions were isolated for a median of 4 days. This is due to the fact that most of the patients were discharged due to clinical stability before reaching the established 5 days. Since the period of the seasonal flu pandemic is concentrated in a few specific weeks 8, it is important to optimize all hospital resources to avoid the collapse of health services and contain hospital transmission of the virus. It is also important to provide the hospital with a team trained in infection that efficiently controls and coordinates the precautionary measures and the necessary days of isolation, the cohort of patients and that is capable of detecting if there is an outbreak of nosocomial influenza. The hospitals must commit to this work philosophy and invest resources, both material and human, promoting the Figure of the infection control nurse, specialized in both the control and prevention of healthcare-related infections.
CONCLUSIONS
The findings of this study confirm that underlying chronic conditions predisposes to a certain extent to infection with the influenza A H1N1 virus. The incidence of Influenza A (N1H1) in the study period is 233.68 cases per 100,000 inhabitants and complications appear in 41.1% of those affected. These data show the importance of infection control team made up of nurses who are capable of efficiently managing patients with flu symptoms during the pandemic period, in order to avoid contagion in the hospital environment and optimize resources
REFERENCIAS
1. Marin J. Et al. Pacientes con gripe por el virus influenza A (H1N1) pdm09 ingresados en la UCI. Impacto de las recomendaciones de la SEMICYUC. Med Intensiva. 2018;42(8):473-481. [ Links ]
2. Lera E, Wörner NT, Sancosmed M,et al. Impacto del virus de la gripe A (H1N1) 2009 en un servicio de urgencias de un hospital de tercer nivel. An Pediatr.2011; 75(1):13-20. [ Links ]
3. Moreno MC, Estrada JM, Fernández D, López A. Actualización sobre el virus de la gripe A: experiencia de una pandemia des de la perspectiva enfermera. Metas de Enferm.2010;13(5):8-16. [ Links ]
4. González R, Balasso V, Uriona S. Et al. Características de los pacientes y carga assistencial durante la pandèmia de gripe A (H1N1) 2009 en el Hospital Universitario Vall d'Hebron de Barcelona. Enferm Infecc Microbiol Clin. 2011;29 (8): 593-600. [ Links ]
5. Trilla A. Transmisión de la gripe en los servicios de urgencias. Emergencias. 2018;30:5-6. [ Links ]
6. Mendoza JL, Quirós V, Jiménez M. Et al. Impacto de la transmisión nosocomial del virus de la gripe en un hospital de agudos. Rev Esp Salud Pu´blica. 2018; 92:1-7. [ Links ]
7. Viasus D, Antón A, Pumarola T, Carratalà J. Influenza A(H1N1)pdm09: beyond the pandemic. Enferm Infecc Microbiol Clin. 2012;30(Supl 4):54-57. [ Links ]
8. Generalitat de Catalunya. Pla d'informació de les infeccions respiratòries agudes a Catalunya (PIDIRAC) [Internet]. 12.08.2019 [revisado; consultado]. Disponible en: http://canalsalut.gencat.cat/ca/professionals/vigilancia-epidemiologica/pla-dinformacio-de-les-infeccions-respiratories-agudes-a-catalunya-pidirac/ [ Links ]
9. Zhoua F. Et al. Risk factors for nosocomial infection among hospitalised severe influenza A(H1N1) pdm09 patients. Respiratory Medicine.2018;134 (1): 86-91. [ Links ]
10. Bouneb R. Et al. Characteristics and outcome of ill critical patients with influenza A infection. The Pan African Medical Journal. 2018; 29:174-182. [ Links ]
11. Alvarez Lerma F. Et al. Delay in Diagnosis of Influenza A (N1H1) pdm09 virus infection in critically ill patients and impact on clinical outcome. 2016; 20(1):337-348. [ Links ]
12. Alvarez Lerma F, et al. Characteristics of patients with hospital-acquired influenza A (H1N1) pdm09 virus admitted to the intensive care unit. Journal of Hospital Infection.2017; 95 (1):200-206. [ Links ]
Received: September 24, 2020; Accepted: January 13, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
