










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.20 no.64 Murcia oct. 2021 Epub 25-Oct-2021
https://dx.doi.org/10.6018/eglobal.466121
Originals
Urinary tract infection in prenatal care: role of public health nurses
1 . Universidad Federal de Tocantins , TO, Brasil. kim_guerra@hotmail.com
2. Enfermera del Programa de Graduación, Universidad Federal de Piaui . Teresina, PI, Brasil.
3 . Instituto de Salud y Gestión Hospitalaria del Hospital Regional Norte, Sobral, CE, Brasil.
Objective:
To explore and describe public health nurses' role in the prenatal consultation to prevent and control urinary tract infection.
Methods:
A qualitative, descriptive study was conducted in 24 basic health units in southern Piauí, northeastern Brazil. The study included 22 public health nurses and was carried out from February to March 2016. Data were collected through a semi-structured questionnaire containing sociodemographic data followed by the interview questions. The IRAMUTEQ software was used for data analysis using the Descending Hierarchical Classification method.
Results:
The following classes were created based on the evoked words: 1 - Routine care of public health nurses assisting pregnant women; 3 - Public health nurse's conduct for treatment and prevention of urinary infection in pregnant women; 4 - Difficulties in diagnosing urinary tract infection in pregnant women; 2 - Health education as the main measure adopted by public health nurses to prevent urinary tract infection in pregnant women.
Conclusions:
Public health nurses lacked protocols and agreement to guidelines. The main measures for preventing and controlling urinary tract infection in pregnant women were adequate intimate hygiene, increased fluid intake, and hygiene before and after sexual intercourse.
Key words: urinary tract infections; pregnancy; nurses; public health; qualitative research
INTRODUCTION
Urinary tract infections (UTIs) are among the most common infectious diseases in clinical practice, particularly in sexually active women, young adults and children 1,2.
Worldwide, about 150 million people are diagnosed each year with UTI, which has a substantial financial impact on both the health care system and society, at a cost that can vary in billions of dollars. In the United States, women who present symptoms linked to UTI represent about 3 to 4% of annual medical consultations. In Brazil, these percentages are nearly doubled. They are responsible for 80 in every 1,000 consultations 3,4. This pathology represents the most common form of bacterial infection during pregnancy, which usually manifests itself in the first trimester, affecting about 12% of pregnant women. In addition, UTIs are the third most common clinical complication due to their anatomical and physiological damage in the urinary tract 5,6.
Approximately 5 to 12% of pregnant women are affected by asymptomatic bacteriuria. However, pregnant women with symptoms may develop cystitis (30%), or pyelonephritis (50%). When not properly treated, asymptomatic bacteriuria can lead, in newborns with low birth weight, to pyelonephritis 7,8.
Therefore, it is essential to provide comprehensive care to pregnant women in prenatal care so that quality care allows early identification of those at risk. There is a large body of post-positivist research about UTI treatment, common microorganisms, type of diagnosis, and health professionals' knowledge 1,2. However, there is a scarcity of studies addressing the conduct and subjectivity of nurses' role in caring for pregnant women with urinary tract infection 9. Filling this knowledge gap could enable the understanding of the prevention and control practices adopted for this infection. Therefore, this study aimed to explore and describe public health nurses' role in the prenatal consultation to prevent and control urinary tract infection.
METHODS
Design and sample
This is a descriptive, exploratory study with a qualitative approach. The study was carried out in the twenty-four basic health units belonging to the Family Health Strategy Program (FHSP) of a health center in the south of Piauí, Brazil.
Out of 24 invited nurses, 22 professionals participated - one of them refused; and the other was on maternity leave during the data collection period. Participants were selected intentionally. We included public health nurses who worked in FHSPs for at least one year and performed prenatal consultations. Nurses who were on leave were excluded from the study.
Data collection
Data collection was carried out from February to March 2016, using a semi-structured questionnaire containing basic sociodemographic elements. The interview was guided by a script composed of the following guiding questions: Do you frequently assist or identify pregnant women with urinary tract infection? Talk about your service; What nursing care is provided to pregnant women with urinary tract infection? What is your conduct when, in the prenatal consultation, you find a positive test result for urinary tract infection? Regarding the prevention and control practices of urinary tract infection, what guidelines do you provide to pregnant women?
The data was recorded and transcribed in full. Then, attentive reading of the transcripts was carried out to favor the analytical processing. The interviews were conducted in a private room in each Basic Health Unit. Some interviews were conducted in a private room at the Municipal Health Secretariat headquarters for nurses working in rural areas. All interviews were previously scheduled via a telephone call. Furthermore, the study participants were guaranteed confidentiality and anonymity, and there was no interference in the professional's daily activities at the unit. The average duration of the interviews was nine minutes.
Analytic strategy
The IRAMUTEQ software was used for data analysis (interface of R for multi-dimensional text and questionnaire analysis). IRAMUTEQ is a free program anchored in the R software and the Python language, allowing different statistical analysis forms on the textual corpus10,11. The corpus was defined as the interviews transcribed by the researcher. The transcribed interviews were placed in a single text file, following the IRAMUTEQ tutorial.
The Descending Hierarchical Classification (DHC) method was used to easily organize vocabulary distribution 10,11. This analysis was prepared to obtain classes of text segments that presented vocabulary similar to each other and different from the other classes' text segments. This way, the software organized the data analysis in a DHC dendrogram, which allowed us to obtain classes of text segments with statistically significant Chi-square tests (χ2) and relationships between the classes 10,11.
Subsequently, another dendrogram was constructed to illustrate the classes named with their most evoked words and their respective χ2 values. The words evoked with a frequency greater than or equal to 3 were considered, which presented χ2 greater than or equal to 10 and p-value less than or equal to 0.0001. Each class was described by the most significant words and their respective associations with the class.
This study received approval from the Research Ethics Committee of the Federal University of Piauí with opinion number 1.380.128.
RESULTS
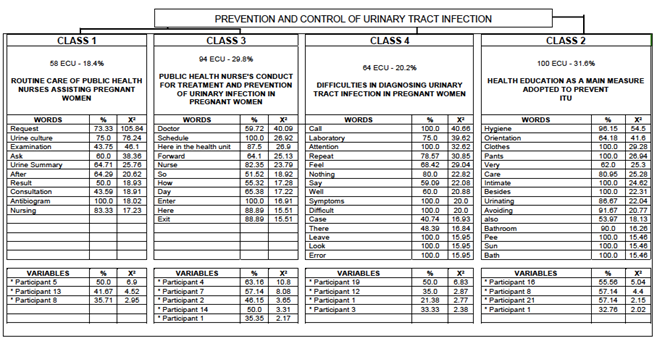
Figure 1. Dendrogram of nurses' assistance in prenatal care for the prevention and control of urinary tract infection
The corpus was divided into 316 analyzable text segments out of 492, with a 64.23% utilization. The analyzable words were distributed in the four classes of this study, as follows (Figure 1): Class 1 with 58 Elementary Context Units (ECU), corresponding to 18.4% of the total text segments; class 3, with 94 ECU, making up 29.8% of the total text segments; class 4 with 64 ECU, totaling 20.2% of the total text segments; and class 2, with 100 ECU, totalling 31.6% of the text segments.
Besides, the appointment of the respective meanings of the classes was: 1 - Routine care of public health nurses assisting pregnant women; 3 - Public health nurse's conduct for treatment and prevention of urinary infection in pregnant women; 4 - Difficulties in diagnosing urinary tract infection in pregnant women; 2 - Health education as the main measure adopted by public health nurses to prevent urinary tract infection in pregnant women. All words presented in the dendrogram of Figure 1 had a p-value of less than or equal to 0.0001.
According to the Descending Hierarchical Classification (DHC), the classes' analysis and discussion must accompany the dendrogram with its partitions, and the reading must proceed from left to right. Thus, the sequence of analysis in the dendrogram was Class 1, Class 3, Class 4 and Class 2.
Class 1 - Routine care of nurses assisting pregnant women
The most frequently and most significant words in this class's text segments are as follows: Request, Urine culture, Examination, Request, Urine Summary, After, Result, Consultation, Antibiogram, and Nursing.
From the speeches and the most evoked words, it was possible to perceive that professional routinely requested the Ministry of Health exams to check for UTI; however, they do it differently. Some request the summary of urine and urine culture for all pregnant women, especially in the first prenatal consultation; others require only urinalysis; as for urine culture, they asked the medical professional to do so. Some only request urine culture if the pregnant woman had any clinical condition (symptomatology) or laboratory alteration (urine summary).
Below are some statements that portray these different approaches.
[...] the request for the exam is made according to the Ministry's schedule, at the beginning of pregnancy and after the 30th week. Now, in cases of urinary infection, yes, I request the exam [...] (Participant 14).
[...] my service was first to request the urine summary, which came with the result and the pregnant woman's complaints, which I remember well. They were dysuria and malaise. The medication was prescribed, and I referred her to the obstetrician at the clinic who requested urine culture [...] (Participant 5).
From this perspective, it is understood that the initial care for pregnant women with urinary tract infection was diverse, as some professionals used all information in the Ministry of Health manual, and others partially used it.
Also, there was a restriction on nurses' autonomy for their work based on the health system. Public health nurses may fear some practices because they do not know their real attributions due to the absence of an institutional protocol.
[...] when it arrives with the result, which is positive, gives positive nitrite, gives the number of leukocytes very large per field. We already identify a possible urinary infection as we have no protocol in the municipality for this service [...] (Participant 16).
On the other hand, the nurses in the study who referred patients for medical consultation to request urine culture performed this procedure unnecessarily. The nurse's request for urine and urine culture tests already exists as a routine in the first and third consultation prenatal.
When considering the professionals who requested the urine culture test, only according to the pregnant woman's clinical or laboratory condition, it can be seen that they followed the recommendations of the updated guideline; however, this request is a hasty form of execution since the manual does not include this type of procedure. However, some professionals performed the procedure of only requesting urine culture when the urine test was altered:
[...] I very often manage it when the summary has an alteration. I request urine culture… it comes with an alteration… Then, I prescribe what I have in the unit and what is in the antibiogram, for example [...] (Participant 8).
In this study, some professionals' practice could be supported by understanding that it is unnecessary or a waste of resources if urine culture is requested concurrently with the urine test.
Class 3 - Public health nurse's conduct for treatment and prevention of urinary infection in pregnant women
The most evoked and significant words in this class's text segments were: Doctor, Schedule, Here in the health unit, Forward, Nurse, So, How, Day, Enter, Here and Exit.
Throughout this class's speeches, the word doctor was constantly evoked, demonstrating that the nurses' conduct is based on the doctor's referral to prescribe treatment if UTI is present. The medical consultation referral took place at the health unit and referral hospital.
[...] having identified this alteration in the abnormal elements and sediment exam, we provide the necessary guidance, but we do the referral because I do not prescribe antibiotics for urinary infections [...] (Participant 4).
[...] so, I start counseling even without an infection. When she has an infection, first, I make the referral either to the doctor from here or directly to the hospital when articulating with the stork network and the use of medication [...] (Participant 7).
Class 4 - Difficulties in diagnosing urinary tract infection in pregnant women
The most significant words for Class 4 were: Call, Laboratory, Attention, Repeat, Feel, Nothing, Say, Well, Symptoms, Difficult, Case, There, Leave, Look, and Error.
It was observed that the number of pyocytes used as parameters to confirm the diagnosis of urinary infection was different among professionals. Some reported having followed what was recommended by the Ministry of Health and others from the reference values specified by laboratories, as can be seen in the statements below:
[...] the number of pyocytes depends, the Ministry of Health says 10 pyocytes per field, but it also depends on the patient's symptoms. For example, if pyocytes are ten per field, the patient is not feeling anything; she has no symptoms [...] (Participant 19).
[...] so, there are always laboratories they vary a lot, and I consider pyocytes above 12, also depending on what the patient reports to me [...] (Participant 12).
With the testimonies, the different references used to complement the complex diagnosis of urinary infection were confirmed. Although some professionals reported doing drug treatment with low reference values (e.g., five pyocytes), this practice is not recommended because an association with other factors is necessary, including the symptoms and presence of the laboratory exam's microorganism, to confirm the diagnosis.
Also, it was possible to perceive that some professionals suspected laboratory error in cases of extreme number of pyocytes without explicit signs and symptoms.
This possible fear can be noticed when the professionals asked the patient to retake the exam in another laboratory. On the other hand, there were cases suggestive of irregularities in the urine collection procedure, storage, or transport of the material. Consequently, these issues may have led to distorted results, as can be seen in the reports below:
[...] we take into account if there is a very absurd result, and the person has no symptoms or characteristics. Then, I try to repeat the exam in another place to compare the results [...] (Participant 3).
These laboratory errors mentioned by nurses cause avoidable health costs. It would also be essential to closely monitor customers and laboratories to identify where the failure occurs.
In this study, the professionals reported previous guidance regarding urine collection before the exam. There were cases that nurses asked pregnant women to repeat the information they received to ensure that the guidelines were understood.
[...] and also when they are going to collect the urine test, I advise that they have to discard the first jet and collect the subsequent one immediately. I do these guidelines [...] (Participant 17).
Class 2 - Health education as the main measure adopted by public health nurses to prevent urinary tract infection in pregnant women
The words that appear most frequently and significantly in this class's text segments are as follows: Hygiene, Orientation, Clothes, Pants, Very, Care, Intimate, Besides, Urinating, Avoiding, Also, Bathroom, Pee, Sun, and Bath. The words belonging to this class were extracted predominantly from interviews 16, 8, and 21.
Based on the words most evoked by the software to compose this class, it was noted that nurses' measures varied. Some were already mentioned in the previous class, such as guidance and health education.
Among the guidelines that were mentioned in the testimonies, some included alerts for the possibility of acquiring UTI due to being pregnant. Others were directed to care for intimate hygiene, avoiding the use of tight clothes and delay in emptying the bladder. It was what can be seen according to the statements below:
[...] and one of these guidelines is aimed at urinary tract infection, which we advise her to say that she may have a urinary tract infection because something that, in practice, we observe happens a lot [...] (Participant 16).
[...] another recommendation is intimate hygiene, regardless of whether or not it is associated with sexual activity, which is like a normal hygiene practice recommended for any woman, regardless of whether or not she is pregnant. But I still reinforce it [...] (Participant 8).
Public health nurses perceived the need to continually educate the user and establish a trust (bond) to carry out the guidelines provided during prenatal consultations. This way, they can ensure that there is a change in behavior:
[...] for pregnant women with urinary tract infections, we give a lot of guidance on the intake of liquid, water, juices [...] (Participant 21).
[...] women during the course of pregnancy have urinary tract infection. So, I usually advise on constant water intake, not holding urine for a long time, especially avoiding wearing tight clothing [...] (Participant 16).
Multiple orientations in the context of sexual intercourse were passed on to pregnant women. They received advice on hygiene practices before and after sexual activities to minimize urinary infection chances, as can be seen in the statement below.
[...] be careful with sexual relations, right? Because you may have a little infection, [...] be careful about hygiene after sex, most of them need this information before and after sex [...] (Participant 2).
On health education, some professionals carried out activities in groups and had students' support. However, some nurses found it more convenient to provide guidance individually, as their clients came from communities far from the countryside. Additionally, in this study, as a health education strategy, some professionals provided guidance and then asked patients to repeat what was said, as seen in the following speeches:
[...] they are in very distant locations, and it is not possible to gather these pregnant women due to distance, geographical difficulties. So, we were not very successful in relation to this group of pregnant women to provide these guidelines. So, it is really individual, as there are few, it is possible to guide them well [...] (Participant 21).
[...] just wash a little. Let the first stream of urine come out; then you'll collect that part right in the middle; it doesn't have to be all of it. Then I ask her to explain to me what she understood [...] (Participant 18).
DISCUSSION
In this study, there was a discrepancy concerning the follow-up protocols established by the Ministry of Health. Also, nurses lacked regional health protocols. For the smooth running of health procedures, protocols are important technology resources for managing human, physical or material resources. For a long time, the use of instruments integrates the health work process, permeating a large part of the spaces and moments of care. Nevertheless, few efforts are observed in the literature to systematize knowledge in this area, which contributes and justifies that its production and use, in part, seem marked by empiricism 12,13. Similarly, UTI therapy can be conducted empirically if it is based on prevalence rates of local urinary infections, protocols developed with the care team, and urine cultures 14.
Protocols are documents to support professional practice; therefore, professionals who use protocols should perform safe procedures. In this regard, public health nurses' protocols are essential in primary care since nurses provide primary and continuous care, aiming to avoid problems throughout the gestational and postpartum period 15,16. Brazilian protocols do not impose on nurses to prescribe medications, request exams or referrals. However, they may allow nurses to these practices if they have scientific and technical capacity 17.
It was also noted in this study difficulties in diagnosing urinary tract infection in pregnant women. The diagnosis of urinary infection in pregnant women is based on the symptoms and laboratory tests requested during the prenatal consultation. These analysis elements are good indications of bacteriuria and are generally considered indirect signs of inflammation 2)(6)(18. Although the diagnosis of urinary infection seems simple, it is often characterized by a more complex situation, given that the presence of leukocytes and nitrite establishes a probable diagnosis. On the other hand, for confirmation, urine culture is necessary because it will isolate and quantify pathogens19.
The urine analysis with positive leukocytes should not be used in isolation to diagnose UTI or initiate antimicrobial therapy in any patient population. Symptoms, too, should be considered for diagnosis. Otherwise, ignoring symptoms may result in unnecessary treatment with a rate of up to 47% 20.
Several public health nurses highlighted questionable results of laboratory tests. The most frequent causes of errors in carrying out and analyzing urine test results are inadequate collection, delay in urine processing, and contamination 21.
A Brazilian study in two groups of pregnant women assisted by two public health nurses at different periods during prenatal care found that one group struggled to follow guidelines for urine collection 22. The preparation for the exam, although little valued, impact the reliability of the results. Additionally, urinalysis is highly susceptible to pre-analytical errors. It is believed that about 30 to 75% of all errors in a laboratory occur in pre-analytical processes. Therefore, measures that ensure the tests' collection's quality must be put into practice 23.
It was noted that nurses use health education to guide pregnant women on the prevention of UTI. Nursing guidelines recommend the nurse's role as an educator, given that there is no education without care and vice versa. Nurses should make critical judgment of their performance and reflect on their role as an educator 24.
Another orientation evidenced concerns fluid intake and hygiene before and after sexual intercourse. Our study corroborates with a study carried out by 25. The authors demonstrated the importance of non-pharmacological measures to prevent UTI in pregnant women, including the habit of urinating after sexual intercourse 25. Nurses should guide and, if necessary, demonstrate a technique for correct hygiene of the genitalia and encourage women to drink plenty of fluids 25.
Regarding sexual activity, it is highlighted that sex predisposes to a higher UTI occurrence, as there is a risk of contamination of the urethra due to the bacteria Escherichia coli being more frequently found in the perineal and intestinal regions 26,27. If a pregnant woman does not have habits of cleaning the pre- and post-coital genitalia and not urinate after intercourse, the risk is even greater. Therefore, the action of urinating after coital and previously washing the genitalia helps to eliminate pathogens that may have migrated to the urethra 26,27.
In our study, public health nurses provided relevant guidance to pregnant women about UTI; however, prenatal care could still be improved with light technologies, such as communication, in the context of primary care. A Brazilian study on health communication with public health nurses showed that professionals sought to implement health education actions through differentiated communication for each user 28. This study highlighted that the most used instrument was verbal communication with patients through lectures, listening, and clear language; however, they also reported that non-verbal communication was satisfactory for educational practice 28.
CONCLUSION
According to study participants, the role of public health nurses in prenatal consultations to prevent and control UTIs should include non-pharmacological measures through educational interventions. These strategies include adequate intimate hygiene, increased fluid intake, and hygiene before and after sexual intercourse. Also, public health nurses should emphasize the importance of wearing light clothing and not delaying voluntary bladder emptying. In this study, the absence of protocol and agreement with the guidelines probably hampered and fragmented patient care. This fragmentation of care goes against health promotion and prevention of UTI.
According to the relationship between the DHC classes, the routine of attending pregnant women seems to be related to public health nurses' practices, leading to difficulties in diagnosis. On the other hand, health education covers all other classes and is the main measure adopted by nurses in their care to prevent UTIs.
A possible limitation of the study was the subjectivity of responses since they were based on each professional's experience. Therefore, there may have been a reduction in responses and, consequently, less accuracy of the study's information.
REFERENCIAS
1. Gupta K, Grigoryan L, Trautner B. Urinary tract infection. Ann Intern Med [Internet]. 2017 Oct 3;167(7):ITC49. Available from: http://annals.org/article.aspx?doi=10.7326/AITC201710030 [ Links ]
2. McLellan LK, Hunstad DA. Urinary tract infection: pathogenesis and outlook. Trends Mol Med [Internet]. 2016 Nov;22(11):946-57. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1471491416301186 [ Links ]
3. Akram M, Shahid M, Khan AU. Etiology and antibiotic resistance patterns of community-acquired urinary tract infections in J N M C Hospital Aligarh, India. Ann Clin Microbiol Antimicrob [Internet]. 2007;6(1):4. Available from: http://ann-clinmicrob.biomedcentral.com/articles/10.1186/1476-0711-6-4 [ Links ]
4. Martini R, Horner R, Roehrs MCMS, Gindri L, Mielke TP, Rodrigues MDA, et al. Caracterização de culturas de urina realizadas no laboratório de análises clínicas do hospital universitário de Santa Maria - Santa Maria, RS, no período de 2007 à 2010. Saúde (Santa Maria) [Internet]. 2011 Sep 15;37(1):55. Available from: https://periodicos.ufsm.br/revistasaude/article/view/3565 [ Links ]
5. Kalinderi K, Delkos D, Kalinderis M, Athanasiadis A, Kalogiannidis I. Urinary tract infection during pregnancy: current concepts on a common multifaceted problem. J Obstet Gynaecol (Lahore) [Internet]. 2018 May 19;38(4):448-53. Available from: https://www.tandfonline.com/doi/full/10.1080/01443615.2017.1370579 [ Links ]
6. Szweda H, Józwik M. Urinary tract infections during pregnancy - an updated overview. Dev period Med [Internet]. 2016;20(4):263-72. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28216479 [ Links ]
7. Hackenhaar AA, Albernaz EP, Tomasi E. Infecção urinária sintomática na gestação e sua associação com desfechos neonatais e maternos desfavoráveis. VITTALLE - Rev Ciências da Saúde [Internet]. 2014;23(2):19-26. Available from: https://periodicos.furg.br/vittalle/article/view/4511 [ Links ]
8. Vasconcelos-Pereira EF de, Figueiró-Filho EA, Oliveira VM de, Fernandes ACO, Fé CS de M, Coelho LR, et al. Urinary tract infection in high risk pregnant women. Rev Patol Trop [Internet]. 2013 Apr 8;42(1). Available from: http://www.revistas.ufg.br/index.php/iptsp/article/view/23590 [ Links ]
9. Hein S, Bortoli CD, Massafera GL. Fatores relacionados à infecção de trato urinário na gestação: revisão integrativa. J Nurs Heal [Internet]. 2016;6(1):83-91. Available from: https://periodicos.ufpel.edu.br/ojs2/index.php/enfermagem/article/view/5977 [ Links ]
10. Camargo B V, Justo AM. IRAMUTEC tutorial [Internet]. 2013. Available from: http://www.iramuteq.org/documentation/fichiers/IRaMuTeQ Tutorial translated to English_17.03.2016.pdf [ Links ]
11. Souza MAR, Wall ML, Thuler ACMC, Lowen IM V, Peres AM. The use of IRAMUTEQ software for data analysis in qualitative research. Rev da Esc Enferm da USP [Internet]. 2018 Oct 4;52. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0080-62342018000100444&lng=pt&tlng=pt [ Links ]
12. Mourão Netto JJ, Dias MSA, Goyanna NF. Uso de instrumentos enquanto tecnologia para a saúde. Saúde em Redes [Internet]. 2016;2(1):65-72. Available from: http://revista.redeunida.org.br/ojs/index.php/rede-unida/article/view/655 [ Links ]
13. Borry EL, Henderson AC. Patients, protocols, and prosocial behavior: rule breaking in frontline health care. Am Rev Public Adm [Internet]. 2020 Jan 10;50(1):45-61. Available from: http://journals.sagepub.com/doi/10.1177/0275074019862680 [ Links ]
14. Miranda AL, Oliveira ALL, Nacer DT, Aguiar CAM. Results after implementation of a protocol on the incidence of urinary tract infection in an intensive care unit. Rev Lat Am Enfermagem [Internet]. 2016;24. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-11692016000100415&lng=en&tlng=en [ Links ]
15. Luz LA, Aquino R, Medina MG. Evaluation of the quality of Prenatal Care in Brazil. Saúde em Debate [Internet]. 2018 Oct;42(spe2):111-26. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0103-11042018000600111&tlng=pt [ Links ]
16. Facundo SHBC, Silva RM, Gonçalves JL, Netto FCB, Queiroz MVO, Brasil CCP. Communication technologies used by nurses in prenatal care. Rev Bras Promoç Saúde [Internet]. 2020;33:1-9. Available from: https://www.redalyc.org/jatsRepo/408/40863235002/html/index.html [ Links ]
17. PIAUI´. Fundac¸a~o Municipal de Sau´de. Diretoria de Articulac¸a~o das Ac¸o~es Assistenciais. Gere^ncia de Atenc¸a~o Ba'sica. Protocolo de Enfermagem na Atenc¸a~o Ba'sica e Ambulato´rios do Munici´pio de Teresina [Internet]. Teresina; 2016. Available from: https://fms.pmt.pi.gov.br/system/downloads/docs/133/original_protocolo_enfermagem.pdf?1531745297 [ Links ]
18. Silva RA, Sousa TA, Vitorino K de A. Infecção do trato urinário na gestação: diagnóstico e tratamento. Rev Científica FAEMA [Internet]. 2019 Jul 26;10(1):71-80. Available from: http://www.faema.edu.br/revistas/index.php/Revista-FAEMA/article/view/765 [ Links ]
19. Matuszkiewicz-Rowinska J, Malyszko J, Wieliczko M. State of the art paper Urinary tract infections in pregnancy: old and new unresolved diagnostic and therapeutic problems. Arch Med Sci [Internet]. 2015;1:67-77. Available from: http://www.termedia.pl/doi/10.5114/aoms.2013.39202 [ Links ]
20. Schulz L, Hoffman RJ, Pothof J, Fox B. Top ten myths regarding the diagnosis and treatment of urinary tract infections. J Emerg Med [Internet]. 2016 Jul;51(1):25-30. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0736467916001220 [ Links ]
21. Silva JMP, Vasconcelos MM de A, Dias C dos S, Vasconcelos MA, Mendonça ACQ, Froes B, et al. Aspectos atuais no diagnóstico e abordagem da infecção do trato urinário. Rev Médica Minas Gerais. 2014;24(Supl 2):20-30. [ Links ]
22. Barros SRAF. Urinary tract infection during gestation and its correlation with low back pain versus nursing interventions. Rev Dor [Internet]. 2013;14(2):88-93. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1806-00132013000200003&lng=pt&nrm=iso&tlng=en%5Cnhttp://www.scielo.br/pdf/rdor/v14n2/en_03.pdf [ Links ]
23. Perucci LO, Magalhães HPB, Borges KBG. Interferências pré-analíticas da urinálise. Anal - Inf técnico [Internet]. 2016;5(18). Available from: http://goldanalisa.com.br/arquivos/%7B2A4EFC61-F049-4ECD-8AC6-CDB7E764C84C%7D_Analisando 18_web.pdf [ Links ]
24. Chaghari M, Saffari M, Ebadi A, Ameryoun A. Empowering education: a new model for in-service training of nursing staff. J Adv Med Educ Prof [Internet]. 2017 Jan;5(1):26-32. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28180130 [ Links ]
25. Schneeberger C, Geerlings SE, Middleton P, Crowther CA. Interventions for preventing recurrent urinary tract infection during pregnancy. Cochrane Database Syst Rev [Internet]. 2015 Jul 26; Available from: http://doi.wiley.com/10.1002/14651858.CD009279.pub3 [ Links ]
26. Fioravante FFS, Queluci GC. Os fatores de risco da infecção do trato urinário na gravidez: revisão integrativa. Rev Enferm Atual Derme [Internet]. 2019 Apr 8;77(15). Available from: https://revistaenfermagematual.com.br/index.php/revista/article/view/375 [ Links ]
27. Lawani EU, Alade T, Oyelaran D. Urinary tract infection amongst pregnant women in Amassoma, Southern Nigeria. African J Microbiol Res [Internet]. 2015;9(6):355-9. Available from: https://academicjournals.org/journal/AJMR/article-abstract/BFB1BD550549 [ Links ]
28. Duarte AS, Alves E, Costa P, Yohanna J, Lima F. Comunicação no Processo Educativo Desenvolvido pelos Enfermeiros: As Tecnologias de Saúde em Análise. Saúde Transform Soc / Heal Soc Chang [Internet]. 2014;5(3):42-8. Available from: http://incubadora.periodicos.ufsc.br/index.php/saudeetransformacao/article/view/2448 [ Links ]
Received: February 01, 2021; Accepted: July 01, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
