










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.21 no.65 Murcia ene. 2022 Epub 28-Mar-2022
https://dx.doi.org/10.6018/eglobal.485981
Originals
Depression implications on older adults' quality of life: a cross-sectional study
1 Universidad de São Paulo, Escuela de Enfermería de Ribeirão Preto, Programa de Posgraduación en Enfermería Fundamental, Ribeirão Preto, São Paulo, Brasil. edison.vitorio@usp.br
2 Universidad Estadual del Sudoeste de Bahia , Programa de Posgraduación en Enfermería y Salud, Jequié, Bahia, Brasil.
3 Universidad Norte do Paraná. Jequié, Bahia, Brasil.
4 Universidad Federal de Minas Gerais, Facultad de Medicina, Departamento de Medicina Preventiva y Social, Belo Horizonte, Minas Gerais, Brasil.
5 Universidad Federal de Alfenas, Programa de Posgraduación en Enfermería, Alfenas, Minas Gerais, Brasil.
Objective:
To analyze the association between depressive symptoms and quality of life in older adults.
Method:
Cross-sectional study carried out between July and October, in 2020, with 596 older adults who answered three instruments, namely: bio-sociodemographic, Geriatric Depression Scale and WHOQOL-Old. Data were analyzed using Chi-square, Kruskal-Wallis, Spearman correlation and linear regression tests, considering a 95% confidence interval (p<0.05).
Results:
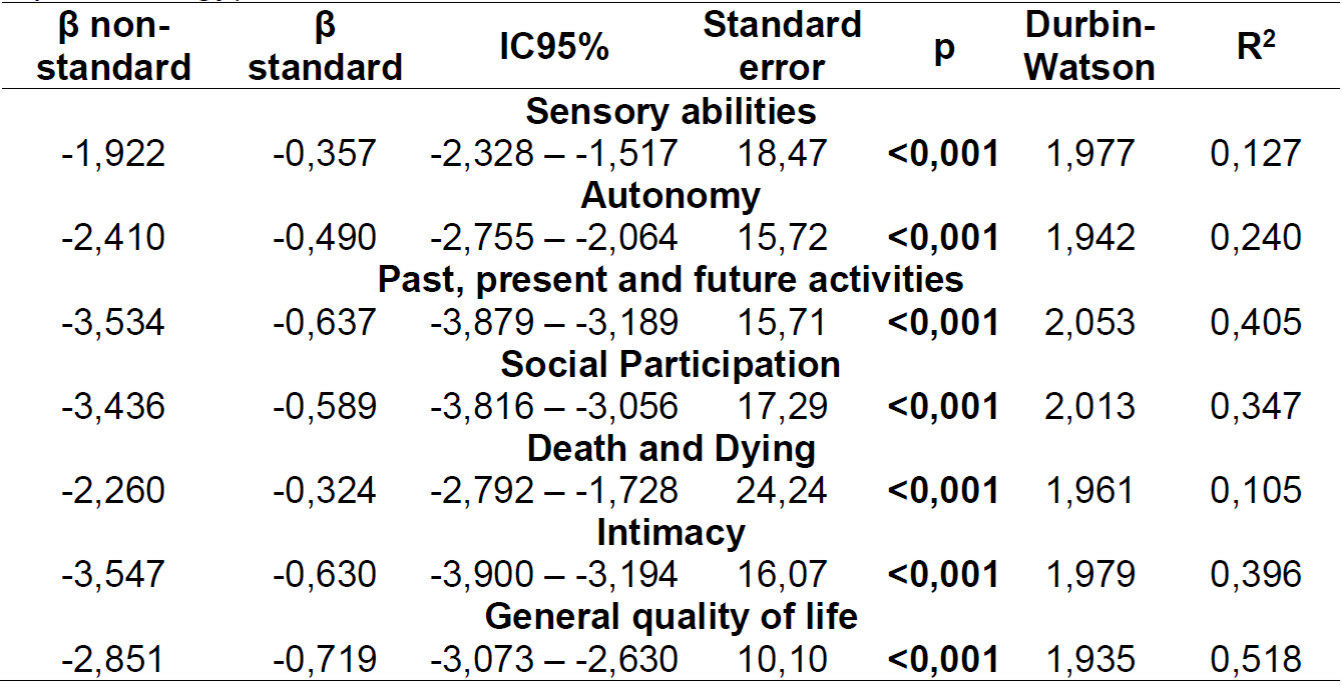
Depressive symptoms were negatively and statistically significantly associated with all facets of quality of life: sensory abilities (β= -1.922 [CI95%= -2.328 - -1.517]); autonomy (β= -2.410 [CI95%= -2.755 - -2.064]); past, present and future activities (β= -3.534 [CI95%= -3.879 - -3.189]); social participation (β= -3.436 [CI95%= -3.816 - -3.056]); death and dying (β= -2.260 [CI95%= -2.792 - -1.728]) and intimacy (β= -3.547 [CI95%= -3,900 - -3.194]).
Conclusion:
The presence of depressive symptoms is negatively associated with the quality of life of older adults, thus requiring interventions in this area.
Keywords: Public Health; Health for the aged; Mental Health; Depression; Primary Health Care
INTRODUCTION
Population ageing is a reality worldwide especially due to mortality and fecundity rates reduction, as well as life expectancy increase 1. Currently, in Brazil, the demographic expansion of the aged population occurs at an accelerated rate. In 2013, estimates indicated a total 26 million of older adults, representing 12.5% of the population 2. In 2018, the projections pointed to 28 million people aged 60 years or more 3. The estimate for the year 2025 is that there will be 32 million older adults in the Brazilian territory 2, becoming, therefore, the sixth country with the largest aged population in the world 4.
It is important to point out that, as this population grows, there is also an increase in the prevalence of pathologies in old age, such as neurological-degenerative diseases and depression 5. Depression is characterized by interest loss, sadness and depressed mood symptoms, considered one of the most prevalent sufferings globally, being responsible for 5.9% of the total disability-adjusted life years 6. It is a disorder that is responsible for a tremendous economic 7, familiar, community and welfare burden (6), and occupies the 15th position concerning public health spending 7.
It is estimated that, worldwide, depressive symptoms affect 350 million people in different age groups. Moreover, according to a mental health survey developed in 17 countries, about one in 20 people reported having a depressive event in the previous year, and one in five people have developed a major depressive disorder at some point in their life cycle 8.
Besides depression, many researchers have been concerned with scientifically investigating the prevalence of the symptoms present in depressive disorders. Thus, the depressive symptomatology is manifested in a subtle way, where dysphoria and somatizations, commonly associated with depressive characteristics, are evidenced 7. Thus, the discussions about senescence and the great current challenge: maintaining autonomy, independence and quality of life (QoL) in old age become increasingly important 9.
QoL has been interpreted through several concepts that have emerged in recent years due to its comprehensive, subjective and multidimensional character 10. It is a variable that depends on several intrinsic and extrinsic factors and which have started being conceptualized in the seventies, in the medical advance context 11. Thus, the World Health Organization (WHO) has defined the QoL concept, which will be adopted as the theoretical reference of the present study, as "an individual's perception of their standing in life, in the cultural context and value systems in which they live and in relation to their goals, expectations, standards, and concerns" 12.
This definition is marked by comprehensive aspects that permeate the individual's life cycle and is not restricted only to individual factors. Therefore, it refers to a concept that ratifies the need for holistic care with an expanded look at the conditioning and health determinants and people's QoL, especially for the aged, to add better quality to their additional life years.
Thus, the research development that investigates the prevalence of depressive symptoms and QoL among this population is essential to assist in making decisions about preventive strategies and appropriate therapy 7, and promoting and maintaining QoL in this age group. Nevertheless, it is necessary to reveal that most studies that address the depressive symptoms and the aged QoL have similar characteristics, such as participants who live in a non-literate, low-education community.
Based on this reality, this study's distinguishing feature is the contribution of highly educated aged people who interact actively in social media through Internet access and electronic devices, which, consequently, can provide better access to information, a reality not very common among most Brazilian aged people. However, due to the gradual increase of undergraduate and graduate courses in Brazil, we infer that this reality will be frequent in the not-too-distant future. Therefore, studies with this population with these characteristics are needed, in order to have an early understanding of their particularities. Hence, this study aims to analyze the association between depressive symptoms and the aged quality of life.
MATERIALS AND METHODS
This is a sectional study with a descriptive and analytical approach. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) tool was used to direct the research development, from data collection to final writing. The study was conducted entirely online between July and October 2020 via the Facebook Social Network. There were no face-to-face meetings between participants and researchers. Thus, during participation in the study, participants were at their respective homes with internet access and active social network accounts.
Sample selection was determined a priori assuming infinite population, 50% conservative proportion, α=5%, and CI=95% (zα/2 = 1.96), obtaining a 385-participant minimum in the study. However, considering the high possibility of dropouts and incomplete answers to the questionnaire, it was decided to add more than 50% (n=211) to the final calculation, totaling 596 participants included in the study through the non-probability consecutive sampling technique.
Inclusion criteria included age (≥ 60 years), gender (male and female), residence in any Brazilian region (North, Northeast, Midwest, Southeast, and South), Internet access and active Facebook account. All the dependent older adults, the hospitalized older adults, and those living in long-stay institutions were excluded from the study. Because these were people with active interaction in social networks and sufficient skills in handling Internet access devices, no instruments were applied to assess cognitive status.
In July 2020, after approval by the REC (Research Ethics Committee), the authors created a page on the social network Facebook to develop scientific studies and disseminate relevant information regarding sexuality, health and QoL for the aged. This is an innovative and promising strategy, especially when there are health restrictions that preclude face-to-face meetings, as is the case with the COVID-19 pandemic. Moreover, the speed at which information is disseminated with the potential for sharing between profiles is a positive point, especially for developing educational activities targeted at different groups.
We published a personalized invitation on the page created, inviting the target audience to participate in the study. This invitation included the research title, the researchers' names, inclusion criteria, and contact information (e-mail address and telephone number). Moreover, the publication was accompanied by a hyperlink that directed the participants to the Google Forms page and the platform in which the instruments were structured.
Three instruments were used to collect bio-sociodemographic data, depressive symptomatology and QoL information. The researchers developed the bio-sociodemographic instrument that contained information regarding gender, age, religious belief, education, marital status, time living with the partner, sexual orientation, Brazilian region, whether they lived with their children, and ethnicity. In this same instrument, three questions were added to know if the aged were dependent, institutionalized or hospitalized during the collection period, in order to meet the exclusion criteria.
The instrument used to evaluate the depressive symptomatology was the Geriatric Depression Scale (GDS) validated for the Brazilian population and comprising 15 questions 13.
The final result was classified as: no symptoms (0 to 5 points), mild depressive symptoms (6 to 10 points) and severe depressive symptoms (11 to 15 points), adopting, therefore, a 5/6 cutoff point (no case/case) 1. It is an instrument built from the original scale constituted by 30 items and approaches aspects related to motivation, cognitive complaints, mood, irritability, energy, past/future orientation and anxiety, considered as recurrent symptoms in geriatric depression 14. In the present study, the EDG showed excellent reliability attested by the 0.855 Cronbach's alpha.
The instrument used to assess QoL was the World Health Organization Quality of Life - Old (WHOQOL-Old), specific for the older adult population, built and validated for application in the Brazilian population 15. It comprises 24 questions that are distributed in six facets: sensory abilities; autonomy; past, present and future activities; social participation; death and dying; and intimacy 16.
The final score varies between 24 and 100 points, and the higher the score, the better the QoL 10,16. Prior to the analyses, the following items were recoded: old_01, old_02, old_06, old_7, old_8, old_9 and old_10. The recoding consisted of assigning new values to the answers given, so that the following rule was obeyed: (1=5; 2=4; 3=3; 4=2 and 5=1), as recommended 17. Finally, this instrument showed excellent reliability by Cronbach's alpha with a 0.900 value. Stratifying Cronbach's alpha by facets, we have the following scores: sensory abilities (0.809); autonomy (0.704); past, present and future activities (0.764); social participation (0.826); death and dying (0.828) and intimacy (0.888).
All these instruments were structured in a single block in Google Forms. We emphasize that, prior to directing the participant to the instruments' block, it was mandatory to include a valid e-mail address so that the second copy of the TCLE could be sent and serve as a data control mechanism, allowing researchers to correct possible multiple answers and, consequently, reduce the chances of bias.
Moreover, the authors hired the post boosting service, allowing Facebook to expand the research dissemination to the entire Brazilian territory and increase people's engagement in the research publication. Thus, it was possible to reach the intended sample entirely online.
As the participants filled out the instruments through Google Forms, the data were automatically stored in an Excel spreadsheet. After the data collection was completed, the authors transported these data to the statistical software IBM SPSS® version 25, in which all the analyses were performed considering a 95% confidence interval (p<0.05). Initially, data distribution was verified using the Kolmogorov - Smirnov test, which showed non-normal distributions (p<0.05) and, therefore, the need to adopt non-parametric statistics.
Thus, we used the chi-square test (χ2) to evaluate qualitative variable proportions and the Kruskal-Wallis H test with Bonferroni posthoc when necessary to evaluate quantitative variables, which were presented via mean ranks, median (Md), and interquartile range (IQR). In order to analyze the existing relationships between the independent variable (depressive symptomatology) and the dependent variable (QoL), Spearman's correlation analysis (ρ) was applied, and its results were presented by the correlation coefficients and their respective p-values. The correlation coefficients were interpreted according to the magnitude of their relations: weak magnitude (ρ <0.4); moderate magnitude (ρ > 0.4 to < 0.5) and strong magnitude (ρ > 0.5) 18.
Afterwards, all the relations that presented a p-value < 0.05 were included in the linear regression considering each QoL facet. We verified the model fit using the Durbin Watson test, and regression results were expressed with the standardized and unstandardized Beta (β) coefficients, confidence intervals, estimate standard error, p-value, and the determination coefficient (R2).
This study respected all ethical and bioethical principles related to the research development with human beings, as recommended by Resolution No. 466/2012 of the National Health Council. Thus, we obtained approval from the Research Ethics Committee (REC) from the Nursing School of Ribeirão Preto - Universidade de São Paulo (EERP/USP) in 2020, under number. 4,319,644 and Certificate of Presentation for Ethical Appreciation (CPEA): 32004820.0.0000.5393. After reading it thoroughly, the participants received the Informed Consent Form (ICF) via e-mail, accepting to participate in the study and knowing the research's objectives, risks, and benefits.
RESULTS
Among the 596 participants, there was a higher rate of males (n=394; 66.1%); aged between 60 and 64 years (n=295; 49.5%), married (n=358; 60.1%), living with their spouse for more than 20 years (n=339; 56.9%); not living with their children (n=382; 64.1%), Catholic (n=291; 48.8%), self-declared white (n=389; 65.3%), complete high school (n=220; 36.9%), followed by college education (n=218; 36.6%), heterosexual (n=515; 86.4%) and living in the Brazilian Southeast region (n=264; 44.3%).
Regarding depressive symptoms, there was a prevalence of elderly classified as absent (n=429; 72.0%), mild symptoms (n=114; 19.1%) and severe symptoms (n=53; 8.9%). Furthermore, the comparison of the bio-sociodemographic variables with depressive symptoms is described in Table 1, in which we observed that only gender had a statistically significant association (p=0.018).
Table 1. Bio-sociodemographic variables comparison according to depressive symptomatology - Ribeirão Preto, SP, Brazil, 2020.
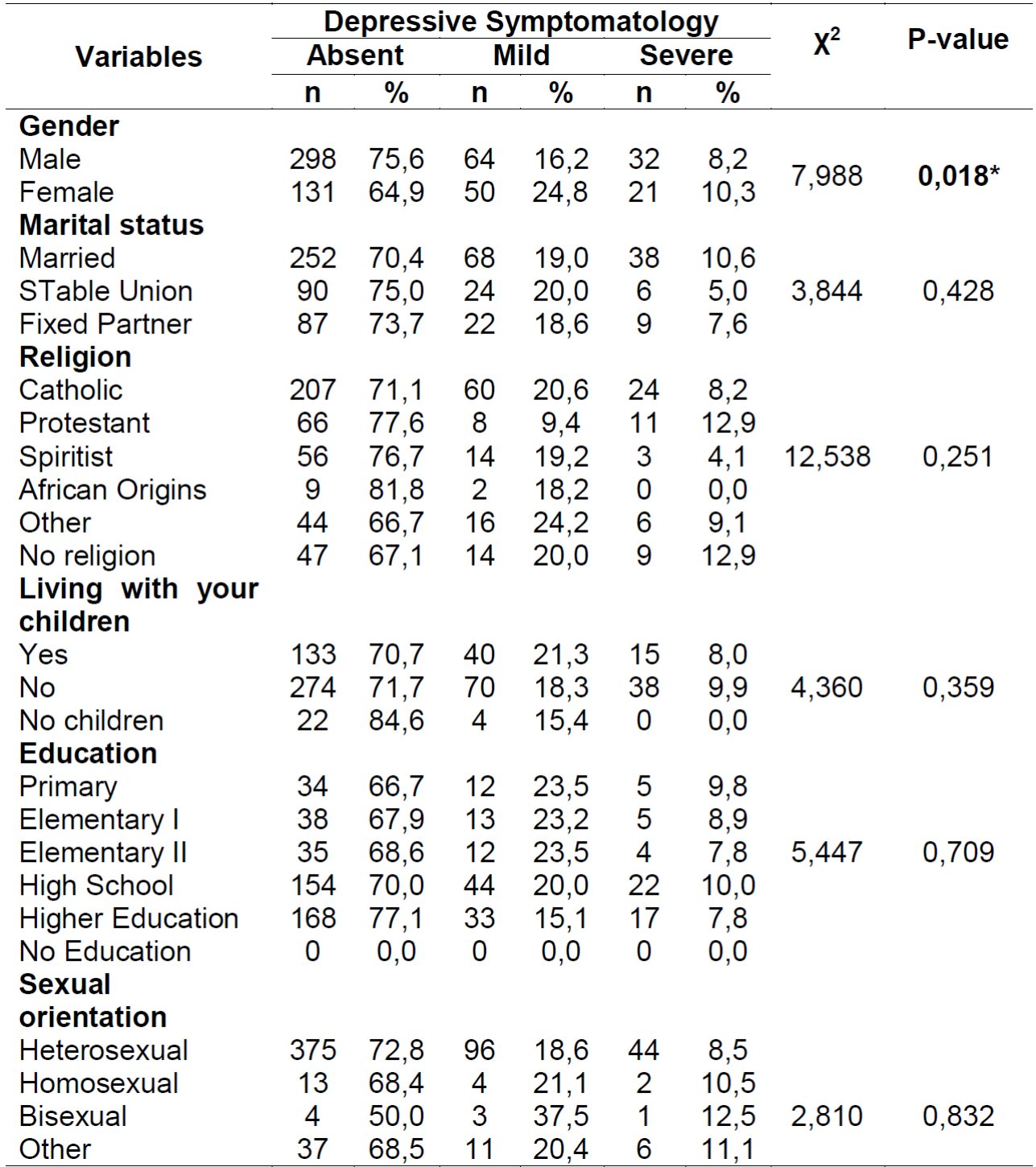
* Statistical significance for Chi-square test (p<0,05)
As shown in Table 2, older adults have a better QoL perception in the sensory abilities facet, regardless of depressive symptoms (p<0.001). Nevertheless, the Kruskal-Wallis H test showed that the differences between the groups are statistically significant, confirming that older adults without depressive symptoms have better QoL in all the facets evaluated. In contrast, when there is an increase in depressive symptoms, the QoL scores decrease, indicating a statistically significant QoL loss for the affected older adult.
Table 2. Comparison between QoL and depressive symptomatology - Ribeirão Preto, SP, Brazil, 2020.
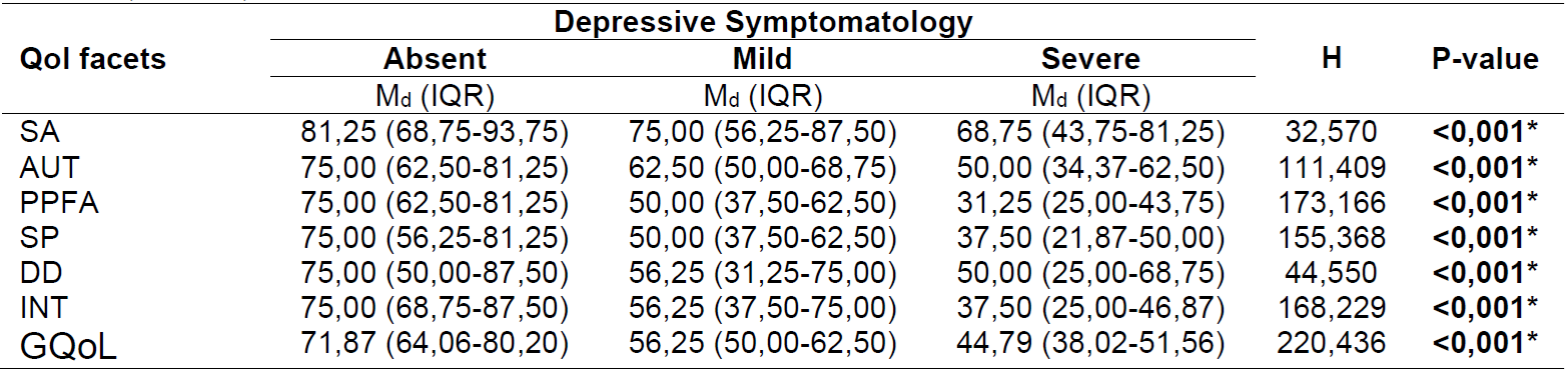
* Statistical significance by Kruskal-Wallis H-test (p<0,05)
SA: sensory abilities; AUT: autonomy; PPFA: past, present and future activities; SP: social participation; DD: death and dying; INT: intimacy; GQoL: general quality of life
When correlating depressive symptomatology with the QoL facets, we observed that all correlations were negative and statistically significant with different magnitudes (p<0.001), according to Table 3.
Table 3. Correlation between depressive symptomatology and QoL facets - Ribeirão Preto, SP, Brazil, 2020.

* Statistical significance for Spearman's correlation (ρ) (p<0,001)
†Weak correlation; ‡Moderate correlation; §Strong correlation
SA: sensory abilities; AUT: autonomy; PPFA: past, present and future activities; SP: social participation; DD: death and dying; INT: intimacy; GQoL: general quality of life
In the linear regression analysis for each QoL facet, we found that depressive symptomatology remained associated, but all associations were negative. These results indicate that the increase in the geriatric depression scale implies a reduction of different magnitudes in their QoL (p<0.001) since the model explained 51.8% of the variation in the elderly's overall QoL data, according to Table 4.
DISCUSSION
In the present study, there was an overall 28% prevalence of depressive symptoms, with 19.1% older adults classified as having mild symptoms and 8.9% as having severe symptoms. It is estimated that the average Brazilian prevalence of depressive symptoms in community-dwelling the aged is 21% (95% CI: 18.0-25.0), according to the meta-analysis study results 7.
According to a Brazilian study 19 developed with 972 senior citizens that used the same assessment scale and cut-off point, depressive symptoms among the participants was 14.2%, where 11.2% referred to mild symptoms and 3% to severe symptoms. Likewise, another similar study 2 developed in Brazil identified a 22% predominance of depressive symptoms among 100 older adults investigated. Nevertheless, when we checked the international literature, a 26.8% prevalence was found among 213 Portuguese older adults, according to a study developed with a methodological approach, which is different from ours 20.
It is worth mentioning that these differences can be explained due to regional dissimilarities and the samples specificities studied 2, citing, for example, studies 2,20, in which older adults with only primary education predominated, diverging from our sample. However, we warn to the fact that depressive symptoms are related to cancer development and several chronic pathologies, such as stroke and Parkinson (6), besides, other undesirable impacts in the older adult's life, being associated with more negative repercussions in the physical, social and functional aspects (4.
In this regard, it is important to highlight that depressive symptomatology were also associated with a 39% increase in the risk of developing cardiovascular diseases, according to a cohort study carried out with 12,417 older adults and middle-aged adults (21). Furthermore, the mutual presence of depression and cardiovascular diseases increases the impacts on public health, promoting unsatisfactory outcomes in the individual's health; besides this, psychic suffering is associated with morbidity and mortality (9.
From this perspective, a greater attention from health professionals for the screening and early depression diagnosis among this population is necessary, especially in Primary Care Centers. Some quick and easy-to-apply instruments can be adopted as an initial screening strategy, such as the EDG in the 10-item version 14 or even the 4-item version 22. Both versions showed good screening capacity, justifying their implementation in the health care context because their sensibility and specificity were, respectively, 100% and 45.7% for the 10-item version 14 and 84.2% and 74.7% for the 4-item version 22. However, we noted that, even though these quick, easy and low-cost instruments exist, they are rarely incorporated into the assessment of the aged4.
It was observed in this study that the aged females were the most prevalent in the mild (24.8%) and severe (10.3%) symptoms, corroborating similar studies 19,20 and even those developed with different instruments and/or cut-off points 23,24. It should be emphasized that, indeed, women present a greater susceptibility to developing depression, and the causal explanations for this reality are still inconsistent 2. Thus, according to a population-based study 6 of 103,595 Chinese men and women, women are twice as likely as men to develop depressive symptoms.
The literature points out some factors that can significantly contribute to this event, such as women's greater longevity, which consequently increases their exposure to stressful events 2,8 with a greater tendency for women to internalize these events 20. Furthermore, there is gender typification, in which women are more allowed to express depressive symptoms 20, hormonal variations during the life cycle phases 25, work overload; status and power inequalities, among other factors 6.
Regarding QoL, it was evidenced in this study that the aged perceived better QoL in the sensory abilities facet, despite depressive symptoms (p<0.001), confirming the results of some investigations 26,27 and diverging from others 28,29, in which the best QoL perception was observed in the death and dying facet 28 and in the intimacy facet 29. The sensory abilities facet assesses the impact that the loss of the sensory functions promotes in the aged QoL, such as hearing, smell, touch and vision 30.
Thus, it can be inferred that, in some way, the sensory abilities investigated are maintained enough to experience with quality the auditory, tactile, olfactory and visual events of their daily lives. Moreover, the sample characteristic as to the high educational level may have influenced this aspect, given that the better socioeconomic conditions provided by high education may have positively influenced the self-care practices and health promotion among older adults, especially with regard to access to the Internet and quick obtaining information.
Another relevant result was that older adults without depressive symptoms have better QoL in all the facets evaluated, while when this symptomatology increases, the QoL scores decrease, indicating a statistically significant QoL loss in the affected older adult.
The big problem is that both depression and depressive symptoms are underdiagnosed in this population, being confused, many times, as ageing process effects or with other pathologies 4. This evidence is worrisome since our results showed that depressive symptoms correlated negatively with QoL, i.e., as these symptoms increase, there is a different magnitude reduction in their QoL, thus, requiring interventions in this area.
Thus, it is essential that Primary Care professionals, in addition to incorporating the depression symptoms tracking to their care practices, also implement scientifically proven actions that reduce these symptoms and/or even prevent them. It should be mentioned as actions that help in the reduction: creating group activities as a tool to operationalize the care to the aged with these symptoms and implementing the physical exercise practice 4.
We emphasize that our results should be interpreted and used with caution because, due to the non-probabilistic design, the generalizability of the results is weakened. In addition, the study participants have their own characteristics, especially regarding the high educational level identified in 73.5%, being 36.9% (n=220) high school graduates and 36.6% (n=218) college graduates, characteristics that do not represent the Brazilian elderly majority 3.
Despite such limitations, this study contributes to understanding the relationship between depressive symptoms and elderly QoL, which may be significant in the future due to the increase in undergraduate and postgraduate courses in Brazil and, consequently, the increase in the young people's education level, who will go into old age with this characteristic. Thus, it is expected that health professionals working in primary care begin an awareness, training and self-criticism process to create and implement strategies that could prevent depressive symptoms and improve the QoL for the aged.
Financing:
This work was carried out with the support of the Coordination of Higher Education Personnel - Brazil (CAPES) - Financing Code 001
REFERENCES
1. Melo LA, Andrade L, Silva HRO, Zazzetta MS, Santos-Orlandi AA, Orlandi FS. Frailty, depressive symptoms, and quality of life: A study with institutionalized older people. Rev Baiana Enferm. 2018;32(e26340). Doi: http://dx.doi.org/10.18471/rbe.v32.26340 [ Links ]
2. Uchoa VS, Chaves LL, Botelho EP, Polaro SHI, Oliveira M de FV. Factors associated with depressive symptoms and functional capacity in elderly*. Cogitare Enferm. 2019;24(0):e60868. Doi: http://dx.doi.org/10.5380/ce.v24i0.60868 [ Links ]
3. Instituto Brasileiro de Geografia e Estatística. Idosos indicam caminhos para uma melhor idade [Internet]. 2019 [cited 2021 Feb 11]. Available from: https://censo2021.ibge.gov.br/2012-agencia-de-noticias/noticias/24036-idosos-indicam-caminhos-para-uma-melhor-idade.html [ Links ]
4. Moreira LB, Silva SLA, Castro AEF, Lima SS, Estevam DO, Freitas FAS, et al. Factors associated with functional capacity in the elderly enrolled in the family health strategy. Ciênc Saúde Coletiva. 2020;25(6):2041-50. Doi: https://doi.org/10.1590/1413-81232020256.26092018 [ Links ]
5. Sousa KA, Freitas FFQ, Castro AP, Oliveira CDB, Almeida AAB, Sousa KA. Prevalence of depression symptoms in elderly people assisted by the family health strategy. Rev Min Enferm. 2017;21:e1018. Doi: https://doi.org/10.5935/1415-2762.20170028 [ Links ]
6. Liu Q, Cai H, Yang LH, Xiang YB, Yang G, Li H, et al. Depressive symptoms and their association with social determinants and chronic diseases in middle-aged and elderly Chinese people. Sci Rep. 2018;8:3841. Doi: https://doi.org/10.1038/s41598-018-22175-2 [ Links ]
7. Meneguci J, Meneguci CAG, Moreira MM, Pereira KR, Tribess S, Sasaki JE, et al. Prevalence of depressive symptoms among Brazilian older adults: A systematic review with meta-analysis. J Bras Psiquiatr. 2019;68(4):221-30. Doi: https://doi.org/10.1590/0047-2085000000250 [ Links ]
8. Lampert CDT, Ferreira VRT. Factors associated with depressive symptomatology in the elderly. Aval Psicol. 2018;17(2):205-12. Doi: http://dx.doi.org/10.15689/ap.2018.1702.14022.06 [ Links ]
9. Zhang Y, Chen Y, Ma L. Depression and cardiovascular disease in elderly: Current understanding. J Clin Neurosci. 2018;47:1-5. Doi: https://doi.org/10.1016/j.jocn.2017.09.022 [ Links ]
10. Teston EF, Marcon SS. Comparative study of quality of life of elderly living in condominiums versus community dwellers. 2015 [cited 2020 Nov 6];33(1):53-62. Available from: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0120-53072015000100007&lng=en&tlng=pt [ Links ]
11. Lima S, Teixeira L, Esteves R, Ribeiro F, Pereira F, Teixeira A, et al. Spirituality and quality of life in older adults: A path analysis model. BMC Geriatr. 2020;20:259. Doi: https://doi.org/10.1186/s12877-020-01646-0 [ Links ]
12. The Whoqol Group. The World Health Organization Quality of Life Assessment (WHOQOL): development and general psychometric properties. Soc Sci Med. 1998;46(12):1569-85. Doi: http://dx.doi.org/10.1016/s0277-9536(98)00009-4 [ Links ]
13. Almeida OP, Almeida SA. Reliability of the Brazilian version of the geriatric depression scale (GDS) short form. Arq Neuropsiquiatr. 1999;57(2B):421-6. Doi: https://doi.org/10.1590/S0004-282X1999000300013 [ Links ]
14. Apóstolo J, Bobrowicz-Campos E, Reis I, Henriques S, Correia C. Capacidade de rastreio da Escala de Depressão Geriátrica com 10 e 5 itens. Rev Enferm Ref. 2018;IV Série(16):29-40. Doi: https://doi.org/10.12707/RIV17062 [ Links ]
15. Fleck MP, Chachamovich E, Trentini C. Development and validation of the Portuguese version of the WHOQOL-OLD module. Rev Saúde Pública. 2006;40(5):785-91. Doi: https://doi.org/10.1590/S0034-89102006000600007 [ Links ]
16. Scherrer Júnior G, Okuno MFP, Oliveira LM, Barbosa DA, Alonso AC, Fram DS, et al. Quality of life of institutionalized aged with and without symptoms of depression. Rev Bras Enferm. 2019;72(2):127-33. Doi: https://doi.org/10.1590/0034-7167-2018-0316 [ Links ]
17. World Health Organization. The WHOQOL-OLD module-manual [Internet]. 2006 [cited 2021 Jan 19]. Available from: https://www.who.int/mental_health/evidence/WHOQOL_OLD_Manual.pdf?ua=1 [ Links ]
18. Hulley SB, Cummings SR, Browner WS, Grady D, Hearst N, Newman TB. Delineando a pesquisa clínica: uma abordagem epidemiológica. 2ª Ed. Porto Alegre: Editora Artmed; 2003. [ Links ]
19. Mendes-Chiloff CL, Lima MCP, Torres AR, Santos JLF, Duarte YO, Lebrão ML, et al. Depressive symptoms among the elderly in são paulo city, Brazil: Prevalence and associated factors (SABE study). Rev Bras Epidemiol. 2018;21(supl.2):E180014.SUPL.2. Doi: https://doi.org/10.1590/1980-549720180014.supl.2 [ Links ]
20. Faísca LR, Afonso RM, Pereira H, Patto MAV. Loneliness and depressive symptomatology in elderly people. Anal Psicol. 2019;37(2):209-22. Doi: http://dx.doi.org/10.14417/ap.1549 [ Links ]
21. Li H, Zheng D, Li Z, Wu Z, Feng W, Cao X, et al. Association of Depressive Symptoms With Incident Cardiovascular Diseases in Middle-Aged and Older Chinese Adults. JAMA Netw open. 2019;2(12):e1916591. Doi: https://doi.org/10.1001/jamanetworkopen.2019.16591 [ Links ]
22. Castelo MS, Coelho Filho JM, Siqueira Neto JI, Noleto JCS, Lima JWO. Escala de Depressão Geriátrica com quatro itens: um instrumento válido para rastrear depressão em idosos em nível primário de saúde. Geriatr Gerontol [Internet]. 2007 [cited 2021 Feb 10];1(1):28-33. Available from: https://cdn.publisher.gn1.link/ggaging.com/pdf/v1n1a05.pdf [ Links ]
23. Rahman MS, Rahman MA, Ali M, Rahman MS, Maniruzzaman M, Yeasmin MA, et al. Determinants of depressive symptoms among older people in Bangladesh. J Affect. 2020;264:157-62. Doi: https://doi.org/10.1016/j.jad.2019.12.025 [ Links ]
24. Zhong BL, Ruan YF, Xu YM, Chen WC, Liu LF. Prevalence and recognition of depressive disorders among Chinese older adults receiving primary care: A multi-center cross-sectional study. J Affect Disord. 2020;260:26-31. Doi: https://doi.org/10.1016/j.jad.2019.09.011 [ Links ]
25. Didoné LS, Jesus ITM, Santos-Orlandi AA, Pavarini SCI, Orlandi FS, Costa-Guarisco LP, et al. Factors associated with depressive symptoms in older adults in context of social vulnerability. Rev Bras Enferm. 2020;73(supl.1):e20190107. Doi:http://dx.doi.org/10.1590/0034-7167-2019-0107 [ Links ]
26. Almeida BL, Souza MEBF, Rocha FC, Fernandes TF, Evangelista CB, Ribeiro KSMA. Quality of life of elderly people who practice physical activities. Rev Fun Care Online. 2020;12(0):432-6. Doi: http://dx.doi.org/10.9789/2175-5361.rpcfo.v12.845 [ Links ]
27. Manso MEG, Maresti LTP, Oliveira HSB. Analysis of quality of life and associated factors in a group of elderly persons with supplemental health plans in the city of São Paulo, Brazil. Rev Bras Geriatr Gerontol. 2019;22(4):e190013. Doi: http://dx.doi.org/10.1590/1981-22562019022.190013 [ Links ]
28. Tavares DMS, Matias TGC, Ferreira PCS, Pegorari MS, Nascimento JS, Paiva MM. Quality of life and self-esteem among the elderly in the community. Ciênc Saúde Coletiva. 2016;21(11):3557-64. Doi: https://doi.org/10.1590/1413-812320152111.03032016 [ Links ]
29. Molina NPFM, Tavares DMS, Haas VJ, Rodrigues LR. Religiousity, spirituality and quality of life of elderly according to structural equation modeling. Texto Context - Enferm. 2020;29:e20180468. Doi: http://dx.doi.org/10.1590/1980-265X-TCE-2018-0468 [ Links ]
30. Costa FR, Rodrigues FM, Prudente COM, Souza IF. Quality of life of participants and non-participants of public physical exercise programs. Rev Bras Geriatr Gerontol. 2018;21(1):24-34. Doi: https://doi.org/10.1590/1981-22562018021.170136 [ Links ]
Received: July 10, 2021; Accepted: September 28, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
