










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.22 no.72 Murcia oct. 2023 Epub 04-Dic-2023
https://dx.doi.org/10.6018/eglobal.553931
Originals
Husbands' support synergistically with distance to vaccination centre associated with childhood immunization compliance during the COVID-19 pandemic in Indonesia
1Faculty of Nursing, Universitas Indonesia. Indonesia
2Faculty of Medicine and Health Science, Universitas Kristen Satya Wacana. Salatiga, Indonesia
3School of Health Sciences Widya Dharma Husada Tangerang. Indonesia
4The Chinese University of Hong Kong, Hong Kong SAR. Hong Kong
Introduction:
During the COVID-19 pandemic, compliance with childhood immunization in Indonesia declined.
Objective:
To determine the independent factors and the relation between the synergistic effect of husbands' support and distance to vaccination centres on compliance with childhood immunization during the pandemic.
Material and Methods:
A total of 506 mothers in Jambi Province, Indonesia, participated in a cross-sectional study from March until May 2021. The associations between the factors were analysed using logistic regression. From the most contributing variables, the researchers made dummy variables (2x2) to investigate the synergistic association on compliance with childhood immunization of husband support and the distance to vaccination centres.
Results:
Among the variables with positive correlations to childhood vaccination, supportive husbands and less distance to vaccination centres had a synergistic effect on compliance with immunization (AOR 95% CI = 4.10 [2-8.41]). Groups that was less supportive from husband and the distance <4km as well as the groups was husband's support but the distance >4km had less compliance (AOR 95% CI = 2.47 [1.22-4.97]; 2.83 [1.18-6.81]).
Conclusions:
Family support and accessibility to childhood immunization should be increased during vaccination campaigns.
Keywords: COVID-19; immunization; spouses support; synergistic association
INTRODUCTION
Global childhood vaccination continues to decrease during the COVID-19 pandemic(1). More than 60% of the 25 million children who were unvaccinated or under vaccinated in 2021 were in 10 countries, including Indonesia(2). During the COVID-19 pandemic, the Community Health Centers (CHCs) of Indonesia continued to provide complete basic immunizations. However, the services of the Integrated Health Centers (IHCs) - a community-based health service which also provides vaccination - were suspended(3). Overall immunization services were disrupted in more than 90% of IHCs in Indonesia(4). Consequently, compliance with childhood immunization declined.
Complete immunization coverage for children has been associated with various factors. One study in Indonesia showed that birth order, antenatal care, socioeconomic status, delivery place, residence, geography and labour helper were significant factors related to complete immunization(5,6). Moreover, maternal factors i.e. mothers' education, age, number of children, perception, knowledge and attitude were also found to be associated with the immunization completion(7-9). Fascinatingly, these maternal factors were also found to be associated with the support of husband(10,11).
It has been suggested that this phenomenon is stronger in countries with strong patriarchal systems, such as Indonesia(12). This was confirmed by a study in Indonesia that showed during the pandemic, maternal factors in immunization compliance were strongly related to the husband's support(10). Another study revealed that the increase in complete basic immunization was strongly related to the husbands' support itself(11). It suggested that the husband's support was essential to immunization compliance, particularly in Indonesia. However, not many studies have investigated the association between husbands' support and mothers' compliance with basic vaccinations for their children.
As noted earlier, geography is also a factor in compliance with immunization in Indonesia, including access to health services. Children living in the remote areas had the highest risk of being unvaccinated(6). Other researchers have confirmed that the availability of health facilities and the distance between home and vaccination centres were important in compliance with children's immunization(13-16).
The geographic factor or the distance from home to healthcare facilities in Indonesia is a major challenge(6). Moreover, its vigour culture includes a patriarchal system in which husbands are allowed to dominate their wives(12). The hypothesized synergy between those two components are strongly crucial in investigating the factors in fulfilling the basic immunization of children. However, to the best of the researchers knowledge, there has been no such research on the effect of the synergy between the husband's support and the distance to health facilities on compliance with children's immunization, particularly in Indonesia. Thus, this research aimed to analyse the relationship between the synergistic association of husbands' support and the distance from home to health facilities and compliance with children's immunizations.
MATERIAL AND METHOD
Study Design
The study was conducted in Jambi Province, Indonesia, from the beginning of March until the end of May 2021, when the COVID-19 pandemic happened. Jambi is one area in Indonesia where the immunization compliance rate has decreased. The percentage of basic immunizations in Jambi City declined by 7.1% points between 2019 and 2020 because of the COVID-19 pandemic(17). A cross-sectional study was conducted among children who received complete immunizations and those who did not.
Sample
A required sample size of 506 respondents was estimated using G-Power 3.1 software(18). The researchers considered potential confounding factors and reduced type 1 errors, with an alpha level (α) = 0.02 and a power (1 - ß) of 0.80 and 2.28 as the risk probability (19,20). Therefore, the researchers sampled 244 mothers who complied with basic immunizations and 262 mothers who did not comply. Both groups were randomly selected.
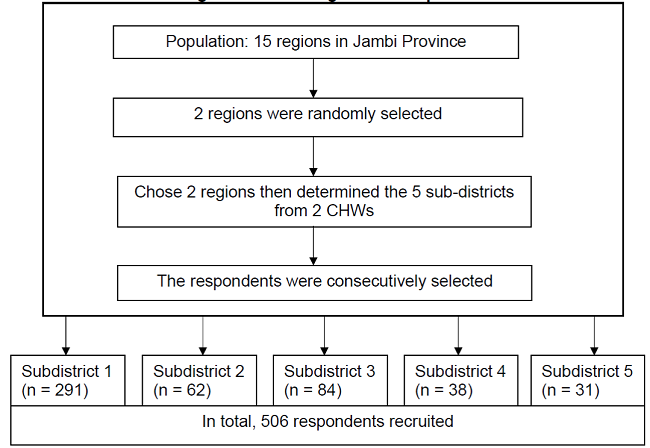
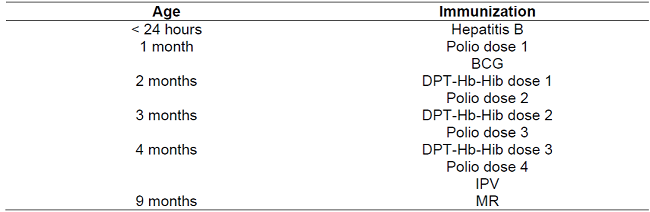
Stratified multistage cluster sampling was used to recruit mothers with children aged 9-24 months with complete or incomplete basic immunizations who could read and write and who had the ‘Mother and Child Health Book' (a small book kept by mothers that includes the vaccination records among many other essential children development records). Two of the 15 Jambi Province regions were randomly selected. From those two regions, the researchers chose five sub-districts, where 506 respondents were consecutively recruited (see Diagram 1). Mothers' compliance with childhood immunization refers to the mothers' behaviours to follow medical or health advice to have their children aged 0-11 months old receive all basic immunizations. This was determined by examining the written immunization records in the child health book. The schedule for complete basic immunization in Indonesia can be found in Table 1. Children who suffered from disorders (e.g., malignancy or HIV/AIDS) that contraindicated immunizations were excluded from this study.
Data Collection and Measurement
Demographic characteristics of the participants
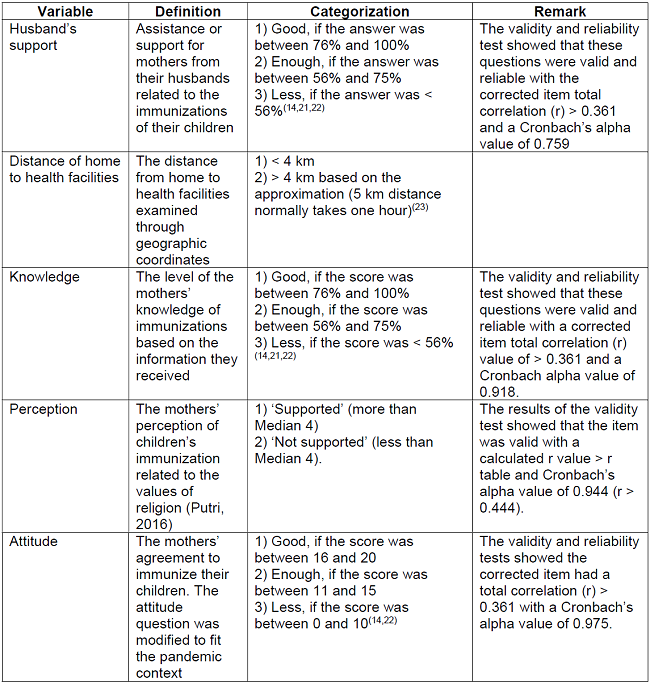
The demographic data including the number of children, family income, health insurance, health protection protocol during the COVID-19 pandemic, data on support from health professionals, mother's experience with children's basic immunization, and transportation access to the health facilities were collected. In addition, support from the husband, the distance to health facilities, mothers' knowledge of childhood immunizations, mothers' perceptions of childhood immunizations, and mothers' attitudes towards children's immunizations were also examined. The complete description of these variables is presented in Table 2.
Data analysis
Continuous data variables were checked for normality. Some variables that were not normally distributed were categorized using the median as the cut-off point. For the distribution of respondents' characteristics, the X2 test was used. The variables that were significant in the univariate analysis (total number of children and education level) were used as the covariates in the final model. A logistic regression was used to examine the associations between husband support, distance to health facilities, knowledge, perception and attitude with basic vaccination compliance to obtain the unadjusted and adjusted odds ratios (ORs, AORs) with 95% confidence intervals (CIs).
Then, the synergistic effect between a husbands' support and the distance from home to health facilities was estimated after creating four dummy variables for the following four (2 × 2) conditions: (1) less supportive husband and distance > 4km (the reference condition or β00); (2) less supportive husband and distance < 4km (β01); (3) supportive husband and distance > 4km (β10) and (4) supportive husband and distance < 4km (β11). The researchers calculated the additive interaction or synergistic effect using the following categories: (1) if β11 = β01 + β10, no interaction; (2) if β11 > β01 + β10, a positive interaction revealing a synergistic effect as a result of more than additivity; and (3) if β11 < β01 + β10, a negative interaction(24). Statistics were deemed significant at p < 0.05. The data were entered and analysed using the stastistical software.
RESULTS
A total of 506 respondents participated in the study. This sample was divided into two groups: 244 mothers who complied with basic immunizations and 262 mothers who did not comply with basic immunizations. The sociodemographic characteristics of the respondents and the differences between two groups are presented in Table 3. Most respondents in both group were Muslim, went to college, had a health insurance, had a health protocol of the facility, had an easy access of transportation, had experiences to comply with children basic immunization, and had a good health professional support. In the group of mothers who did comply with basic immunization, the majority of the respondents had more than 2 children, while in the group of mothers who did not comply with basic immunization, the majority of the respondents had 1 children. Among those sociodemographic characteristics, significant differences were only found in the educational level and total number of children.
Table 3. Demographic characteristics of mothers who did not comply with basic vaccination and mother who did comply with basic vaccination (N = 506).
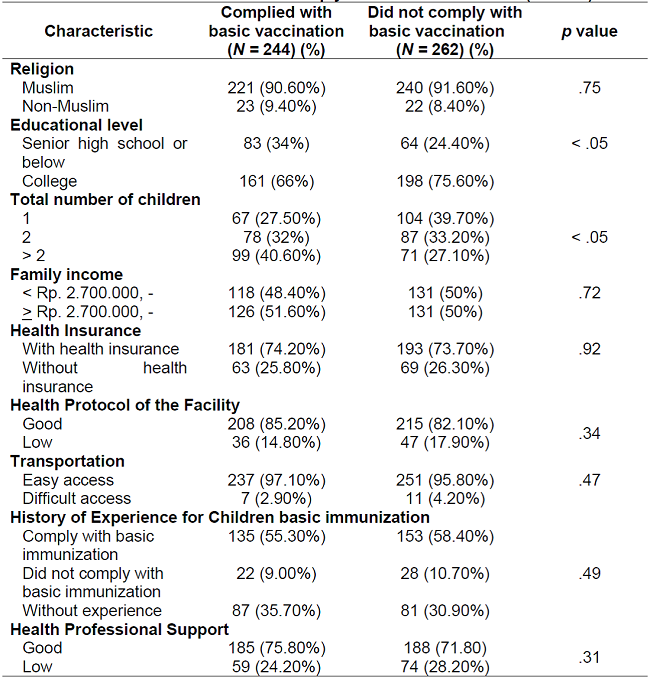
Note.X2 test was used to compare groups.
1 US$= Rp. 15.177
The potential factors for mothers' compliance with basic vaccination are depicted in Table 4. Most respondents who did not comply with basic vaccination for their children had less supportive husband (64.10%), lived in less than 4 km distance from the place of immunization (77.5%), had good knowledge of childhood immunization (63.7%), supported basic vaccination compliance (63.40%), and had positive attitude towards vaccination (54.60%). The differences between the compliant and non-compliant groups were all statistically significant.
Table 4. Potential factors for mothers' compliance with basic vaccination (N = 506).
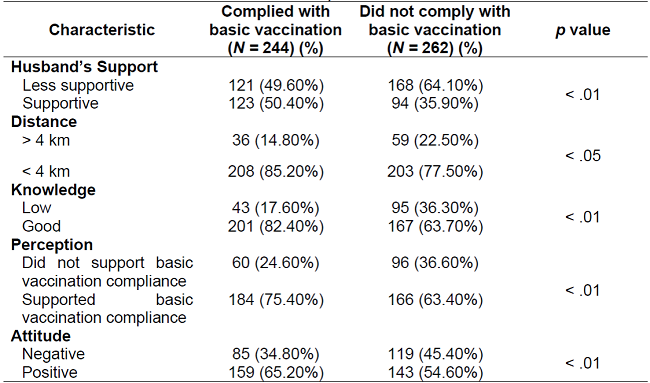
Note.The X2 test was used to compare groups.
Table 5 shows that mothers who lived less than 4 km from health facilities were more likely to comply with basic vaccinations (AORs = 1.80; 95% CI = 1.12~2.89) compared to mothers who lived more than 4 km from health facilities. Moreover, mothers whose perceptions supported basic vaccination were more likely to comply with basic vaccinations (AORs = 1.70; 95% CI = 1.15~2.52) compared with those whose perception did not support basic vaccinations. In addition, mothers with good knowledge of vaccinations were 2.4 times more likely to comply with basic vaccinations (95% CI = 1.57~3.67) compared to those with a low level of knowledge of vaccinations. Mothers with a positive attitude and husband support were also more likely to comply with basic vaccinations (AORs = 1.54; 95% CI = 1.07~2.22 and AORs = 1.78; 95% CI = 1.24~2.56, respectively). All the AORs were computed after adjusting for confounding factors.
Table 5. Odds ratio (OR) and adjusted odds ratio (AOR) of the basic vaccination compliance factors (N = 506).
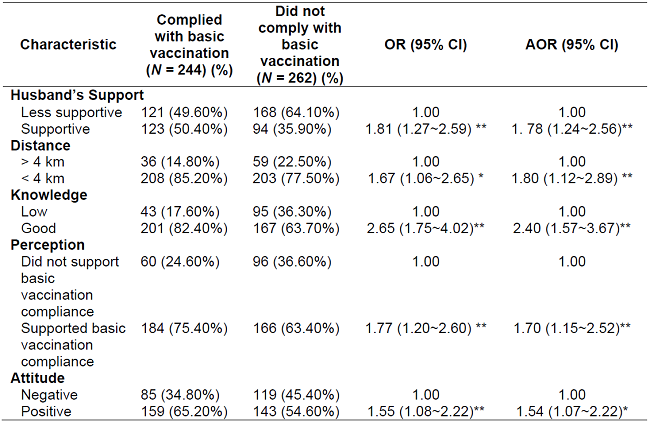
Notes:The OR was calculated with a binary logistic regression test. The AOR was calculated by a multiple logistic regression test and adjusted for total number of their children and educational level.
*Indicates a significant difference in values between groups at p < 0.05.
**Indicates a significant difference in values between groups at p < 0.01
The synergistic effect of husband support and the distance from health facilities with compliance with basic vaccinations presented in Table 6. Mothers with more supportive husbands who lived within 4 km of health facilities had synergistically increased basic vaccination compliance compared with those with less supportive husbands and a distance from health facilities of more than 4 km. The adjusted OR of vaccination compliance was 4.10 95% CI (2-8.41).
Table 6. Odds ratio (OR) and adjusted odds ratio (AOR) of the synergistic effect of husband's support and distance from health services center on basic vaccination compliance (N = 506).
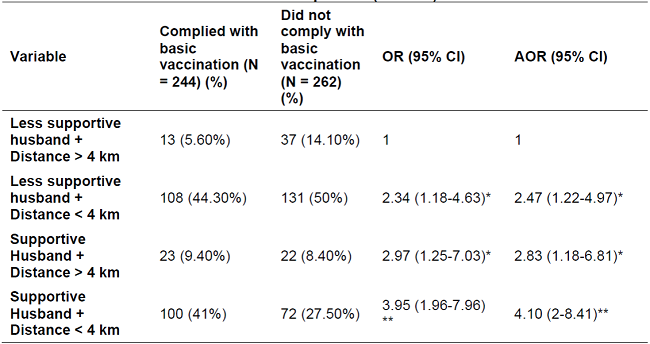
Notes:The OR was calculated with a binary logistic regression test. The AOR was calculated by a multiple logistic regression test and adjusted for total number of their children and educational level.
*Indicates a significant difference in values between groups at p < 0.05.
**Indicates a significant difference in values between groups at p < 0.01.
DISCUSSION
This study discovered that husbands' support and distance from home to health facilities were the strongest factors affecting mothers' compliance with childhood immunizations. To the best of authors' knowledge, this is the first study documenting that these two factors have a strong relationship with immunization coverage for children in Indonesia. During the COVID 19 pandemic, immunization of children remained a priority, and it was vital to protect children from various infectious diseases. The complete basic immunization coverage rate for children in Indonesia was 91.52%(25). During the COVID-19 pandemic, complete basic immunization coverage declined in one year from 52.57% to 50.44%(4). This also occurred in Riyadh, Saudi Arabia, where, since the COVID-19 pandemic began, the number of children receiving immunizations has declined(8). Thus, the support system includes husbands' support and considering the distance from the healthcare facility was important.
The action of husbands' support in health behaviour was to take their wives to a healthcare center(26). Researchers have shown that husbands' support for their wives affects the wives' health behaviours(27,28). This is because the husband's support leads to motivation, encouraging behaviours, providing information, showing empathy, and providing assistance to the wife so that the wife feels more comforTable and safer(28). Husbands' support is especially important during the pandemic, which has made everyday life more difficult for many people, including mothers.
This study has shown that the distance from home to health facilities influences immunization coverage in children. The shorter the distance to health services, the higher the immunization compliance rate. This may be due to the geographical conditions of Indonesia. This finding is consistent with the result of a study in Brazil, which showed that when a location is difficult to reach, it is one factor explaining the high proportion of children not receiving a full dose of immunizations(15). It performed that distance to the health services significantly contribute in the immunization compliance rate.
Remarkably, in Indonesia, remote locations are often accompanied by inadequate infrastructure and transportation facilities, including in Jambi province. Studies have shown that the difficulty of accessing health facilities, long distances from health services, difficulties related to transportation, a long distance from home to health facilities, insufficient finances, and poor infrastructure are obstacles to fulfilling immunizations in Indonesia(29))((30))((31). In line with research in Saudi Arabia, easy access to receive immunizations is a factor that supports parents in providing immunizations for their children(32). Parents are unable to bring their children for vaccines due to access issues. In addition, the pandemic prevented parents from immunizing their children for fear of contracting the virus while taking public transportation to the health facilities(15). Hence, this study confirmed that distance combined with the COVID-19 pandemic circumstances led to uncomplete immunization among children in Indonesia.
The combination of proximity to health facilities and support from the husband is the strongest factor in the successful immunization of children during the COVID-19 pandemic. Due to the pandemic, there has been a decrease in immunization coverage for children, both in Indonesia and in other parts of the world, such as Brazil(15,25). However, immunizing children still occurs when couples support each other(11). To address the distance barrier, one solution would be to administer immunizations during home visits. Suggestions for health workers at primary health care should make home visits to children who have immunization schedules, especially those whose homes are far from healthcare facilities. Home visits would be an effective intervention for children to receive immunizations(15,30).
This research has some limitations. First, in terms of data collection, this research is the result of a self-reported study. Although quality control has been carried out, the possibility of bias from the research subjects cannot be avoided. Furthermore, this study did not compare the coverage of immunizations when the number of COVID-19 cases peaked and declined. Therefore, the factors that directly contributed to the pandemic, such as the fear of giving children immunizations due to the fear of leaving the house and the rules for staying at home, could not be assessed. However, along with its limitations, this study also had some strengths. This study is the first to assess novel issues regarding key related factors and their interaction with adherence to the basic childhood vaccination programme. This was a community-based study with stratified multistage cluster sampling. Thus, the findings might be relevant to similar contexts in all of Indonesia.
CONCLUSION
The presence of husband support, knowledge, attitude, perception and distance have positive correlations to compliance with basic vaccination in the paediatric population. This dummy modelling showed that higher husband support, together with shorter distances to vaccination centres, was four times as likely to adhere to basic childhood immunization than those whose mothers were without husband support and had long distances. Mothers who had husband support or less distance alone performed around half as much compliance as those who had those two factors. Thus, it is important for the government and society to improve access to the facilities for childhood basic immunizations, such as providing mobile health facilities and home visits. In addition, it is important to improve health promotion to increase family support for the success of basic immunization.
REFERENCES
1. UNICEF, The Indonesian Ministry of Health. Imunisasi rutin pada anak selama pandemi COVID-19 di Indonesia: Persepsi orang tua dan pengasuh [Internet]. 2020. Available from: www.unicef.org/indonesia/reports/rapid-assessment-immunization-services-indonesia [ Links ]
2. UNICEF. Immunizations [Internet]. 2022. Available from: https://www.unicef.org/immunization [ Links ]
3. The Indonesian Ministry of Health. Petunjuk teknis: Pelayanan imunisasi pada masa pandemi Covid-19. 2020. Available from: https://covid19.kemkes.go.id/protokol-covid-19/petunjuk-teknis-pelayanan-imunisasi-pada-masa-pandemi-covid-19 [ Links ]
4. UNICEF, The Indonesian Ministry of Health. Penilaian cepat: Dampak pandemi COVID-19 terhadap layanan imunisasi di Indonesia [Internet]. 2020 [cited 2022 Sep 8]. Available from: https://www.unicef.org/indonesia/media/4871/file/Penilaian%20Cepat:%20Dampak%20Pandemi%20COVID-19%20terhadap%20Layanan%20Imunisasi%20di%20Indonesia.pdf [ Links ]
5. Efendi F, Pradiptasiwi DR, Krisnana I, Kusumaningrum T, Kurniati A, Sampurna MTA, et al. Factors associated with complete immunizations coverage among Indonesian children aged 12-23 months. Child Youth Serv Rev. 2020 Jan;108:104651. DOI: 10.1016/j.childyouth.2019.104651 [ Links ]
6. Herliana P, Douiri A. Determinants of immunisation coverage of children aged 12-59 months in Indonesia: a cross-sectional study. BMJ Open. 2017 Dec 22;7(12):e015790. Available from: https://bmjopen.bmj.com/content/7/12/e015790 [ Links ]
7. Adenike OB, Adejumoke J, Olufunmi O, Ridwan O. Maternal characteristics and immunization status of children in north central of Nigeria. Pan African Medical Journal [Internet]. 2017;26:1-15. Available from: https://dx.doi.org/10.11604%2Fpamj.2017.26.159.11530 [ Links ]
8. Aldakhil H, Albedah N, Alturaiki N, Alajlan R, Abusalih H. Vaccine hesitancy towards childhood immunizations as a predictor of mothers' intention to vaccinate their children against COVID-19 in Saudi Arabia. J Infect Public Health [Internet]. 2021 Oct 1;14(10):1497-504. Available from: https://pubmed.ncbi.nlm.nih.gov/34481723/ [ Links ]
9. Tanjung ICD, Rohmawati L, Sofyani S. Complete basic immunization coverage in children and the factors influencing it. Sari Pediatri [Internet]. 2017;19(2):86. Available from: https://dx.doi.org/10.14238/sp19.2.2017.86-90 [ Links ]
10. Carolina AR, Efendi D, Kurniasari MD. Determinant factor of childhood basic immunization compliance during the COVID-19 pandemic in Jambi City, Jambi Province, Indonesia. Journal of Nursing Practice [Internet]. 2021 [cited 2021 Nov 24];5(1):77-88. Available from: https://doi.org/10.30994/jnp.v5i1.154 [ Links ]
11. Ilhami I, Afif M. The Influence of family support on providing complete primary immunizations. Jurnal PROMKES: The Indonesian Journal of Health Promotion and Health Education. 2020 Sep 24;8(2):198. Available from: https://e-journal.unair.ac.id/PROMKES/article/view/16282 [ Links ]
12. Vaezghasemi M, Öhman A, Ng N, Hakimi M, Eriksson M. Concerned and conscious, but defenceless - the intersection of gender and generation in child malnutrition in Indonesia: a qualitative grounded theory study. Glob Health Action. 2020 Dec 31;13(1):1744214. Available from: https://www.tandfonline.com/doi/full/10.1080/16549716.2020.1744214 [ Links ]
13. Bangura JB, Xiao S, Qiu D, Ouyang F, Chen L. Barriers to childhood immunization in sub-Saharan Africa: A systematic review. Vol. 20, BMC Public Health. BioMed Central; 2020. Available from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-020-09169-4 [ Links ]
14. Erynda RF, Sulaeman ES, Pamungkasari EP. Contextual effect of the integrated health post and other determinants on completeness of basic child immunization: A multilevel analysis evidence from Jember, East Java. Journal of Maternal and Child Health [Internet]. 2020;5(2):154-66. Available from: https://thejmch.com/index.php?journal=thejmch&page=article&op=view&path%5B%5D=375&path%5B%5D=pdf [ Links ]
15. Silveira MF, Tonial CT, Goretti K. Maranhão A, Teixeira AMS, Hallal PC, Maria B. Menezes A, et al. Missed childhood immunizations during the COVID-19 pandemic in Brazil: Analyses of routine statistics and of a national household survey. Vaccine [Internet]. 2021 Jun 8;39(25):3404-9. Available from: https://pubmed.ncbi.nlm.nih.gov/33941406/ [ Links ]
16. Yunusa U, Irinoye O, Bello UL, Timothy G. Determinants of parental compliance with routine childhood immunization schedule in Nassarawa State, Nigeria. International Journal of Nursing & Care. 2017 Aug 30;1(3):1-7. DOI: 10.33425/2639-9474.1017 [ Links ]
17. Jambi Public Health Office. Laporan Akuntabilitas Kinerja Instansi Pemerintah (LAKIP) Program Pencegahan dan Pengendalian Penyakit Satker Dekonsentrasi 05 [Internet]. 2020. Available from: https://e-renggar.kemkes.go.id/file2018/e-performance/1-109002-2tahunan-619.pdf [ Links ]
18. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: Test for correlation and regression analyses. Behav Res Method [Internet]. 2009;41(4):1149-60. Available from: https://link.springer.com/content/pdf/10.3758/BRM.41.4.1149.pdf [ Links ]
19. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. New York: Lawrence Erlbaum Associates; 1988. [ Links ]
20. Oyesigye F. Factors affecting compliance of childhood routine immunization and dropout rate in KABUYANDA Town Council-ISINGIRO District. Int J Innov Sci Res Technol [Internet]. 2018;3(2). Available from: www.ijisrt.com [ Links ]
21. Arikunto S. Prosedur Penelitian: Suatu Pendekatan Praktik. Rinek Cipta; 2013. [ Links ]
22. Zuliani. Pengaruh peran suami dan Puskesmas terhadap pengetahuan dan sikap ibu dalam pemberian imunisasi dasar di wilayah kerja Puskesmas Langsa Lama Kota Langsa Aceh Tahun 2016 [Internet]. S2 Ilmu Kesehatan Masyarakat, Fakultas Kesehatan Masyarakat, Universitas Sumatera Utara; 2016 [cited 2021 Nov 28]. Available from: ttps://repositori.usu.ac.id/handle/123456789/19622 [ Links ]
23. Waroux OLP de, Schellenberg JRA, Manzi F, Mrisho M, Shirima K, Mshinda H, et al. Timeliness and completeness of vaccination and risk factors for low and late vaccine uptake in young children living in rural southern Tanzania. Int Health [Internet]. 2013;5(2):139-47. Available from: https://doi.org/10.1093/inthealth/iht006 [ Links ]
24. Kurniasari MD, Karwur FF, Rayanti RE, Dharmana E, Rias YA, Chou KR, et al. Second-hand smoke and its synergistic effect with a Body-Mass Index of >24.9 kg/m2 increase the risk of Gout Arthritis in Indonesia. Int J Environ Res Public Health. 2021 Apr 19;18(8):4324. Available from: https://www.mdpi.com/1660-4601/18/8/4324 [ Links ]
25. The Indonesian Ministry of Health. Profil direktorat surveilans dan karantina kesehatan tahun 2016. 2016. [ Links ]
26. Sodik MA, Simon MMN. Relations role of health promotion and support husband with attitude of couples childbearing age in following family planning program in health. Journal of Global Research in Public Health [Internet]. 2017;2(2):82-9. Available from: https://www.neliti.com/id/publications/225038/the-role-of-health-promotion-and-family-support-with-attitude-of-couples-childbe [ Links ]
27. Ayuningtiyas I, Ropitasari R. The correlation between the support husband with attitude of wife on early detection cervical cancer used iva test in Public Healthy Center of Jaten II Karanganyar. PLACENTUM Jurnal Ilmiah Kesehatan dan Aplikasinya [Internet]. 2018;6(2):33-40. Available from: https://jurnal.uns.ac.id/placentum/article/view/22854/16954 [ Links ]
28. Susanti S, Ningrum WM, Sulistiyoningsih H. Description of factors of husband and health workers' support towards cervical cancer detection behaviour in the child-bearing age at Singaparna Health Centre, Tasikmalaya Sub-District. Healthy and Active Ageing [Internet]. 2019;798-805. Available from: http://prosiding.respati.ac.id/index.php/PIC/article/view/156 [ Links ]
29. Glatman-Freedman A, Nichols K. The effect of social determinants on immunization programs. Hum Vaccin Immunother [Internet]. 2012 Jul;8(7):916-20. Available from: https://pubmed.ncbi.nlm.nih.gov/22327490/ [ Links ]
30. Hardhantyo M, Chuang YC. Urban-rural differences in factors associated with incomplete basic immunization among children in Indonesia: A nationwide multilevel study. Pediatr Neonatol. 2021 Jan 1;62(1):80-9. Available from: https://www.sciencedirect.com/science/article/pii/S1875957220301443 [ Links ]
31. Moïsi JC, Kabuka J, Mitingi D, Levine OS, Scott JAG. Spatial and socio-demographic predictors of time-to-immunization in a rural area in Kenya: Is equity attainable? Vaccine [Internet]. 2010 Aug;28(35):5725-30. Available from: https://pubmed.ncbi.nlm.nih.gov/20600489/ [ Links ]
32. Alshammari TM, Subaiea GM, Hussain T, Moin A, Yusuff KB. Parental perceptions, attitudes and acceptance of childhood immunization in Saudi Arabia: A cross sectional study. Vaccine [Internet]. 2018 Jan 2;36(1):23-8. Available from: https://pubmed.ncbi.nlm.nih.gov/29174681/ [ Links ]
Received: January 13, 2023; Accepted: May 24, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
