










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versión On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.11 no.5 ago./sep. 2006
NECK AND FACIAL PATHOLOGY
Sebaceous adenoma of the parotid gland
Adenoma sebáceo de la glándula parótida
Juan Carlos de Vicente Rodríguez1, Manuel Florentino Fresno Forcelledo2, Manuel González García3, Carolina Aguilar Andrea4
(1) Professor of Oral and Maxillofacial Surgery, Faculty of Medicine and Dentistry, Clinical Head of Oral and Maxillofacial(2) Professor of Pathology, Faculty of Medicine, Head of Pathology
(3) Lecturer, Faculty of Medicine and Dentistry
(4) Trainee of Pathology, Hospital Universitario Central de Asturias (HUCA), Oviedo
ABSTRACT
Tumors of the salivary glands constitute an important field of oral and maxillofacial pathology. The majority of salivary gland neoplasms are benign, with malignant salivary tumors accounting for 15 to 32 percent. The most common site for salivary gland tumors is the parotid gland, accounting up to 80 percent of all cases. This article reports the pathologic picture in a case of sebaceous adenoma of the parotid gland. The tumor was composed of epithelial cells lining ducts and closely associated with broad areas of sebaceous differentiation. The growth pattern was predominantly cystic, with cavities filled with sebaceous material. Areas of oncocytic metaplasia were also seen. The presence of sebaceous glands in salivary neoplasms is frequent, however, and in spite of this, salivary neoplasms constituted partially or entirely of these cells are rarely observed. To the surgeon and pathologist, the major problem in dealing with sebaceous adenoma is the recognition of this rare entity, avoiding confusing with other more aggressive neoplasms. The treatment involves surgical excision. The addition of the current case to the previously published data brings the total number of parotid sebaceous adenoma to seven.
Key words: Salivary gland neoplasm, sebaceous adenoma.
RESUMEN
Los tumores de las glándulas salivales constituyen un área importante de la patología oral y maxilofacial. La mayor parte de las neoplasias glandulares salivales son benignas, representando las malignas entre el 15 y el 32% del total. La localización más común de estas entidades es la glándula parótida, en la que asientan hasta el 80% de todos los casos. En este artículo se presenta un caso de adenoma sebáceo salival, de localización parotídea. El tumor, formado por células epiteliales que tapizan conductos, exhibe amplias áreas de diferenciación sebácea y zonas con metaplasia oncocítica. El patrón histológico es predominantemente quístico, observándose cavidades rellenas con material sebáceo. Si bien la presencia de glándulas sebáceas en las glándulas salivales es frecuente, las neoplasias exclusivamente formadas por las mismas son muy infrecuentes. Dada su rareza, este tumor plantea problemas diagnósticos diferenciales con otras entidades benignas y malignas. Su tratamiento implica la extirpación de la lesión, lo que generalmente involucra la eliminación de la glándula en la que ha surgido. El presente caso constituye el séptimo publicado de esta entidad.
Palabras clave: Neoplasias glandulares salivales, adenoma sebáceo.
Introduction
Extracutaneous sebaceous glands in the head and neck are mainly found in the oral cavity as well as in the major salivary glands. Of these two locations, the later was initially described by Hamperl (1) in the submandibular and parotid glands. The presence of sebaceous glands in salivary neoplasms can take two forms (2): (i) as a part of otherwise benign or malignant salivary neoplasms, such as Warthin tumor, mucoepidermoid carcinoma, and pleomorphic adenoma (3); and (ii) as the sole or preponderant proliferating component. However, in spite of the high prevalence of sebaceous glands and cells in salivary glands, salivary neoplasms constituted partially or entirely of these cells are rarely observed. Nearly 80% of adults show sebaceous glands on the lips or buccal mucosa (Fordyces granules) and they are considered as a normal rather than a pathological condition (2). Due to this high prevalence, it is difficult to confirm the salivary origin of sebaceous adenomas in minor salivary glands (4), as opposed to in major glands.
This article presents an extremely rare case of sebaceous adenoma located in the left parotid gland.
Case report
A 59-year-old white woman was admitted to the hospital with a slowly growing mass of the left parotid gland, which had first been seen four years earlier. Her medical history was uneventful and no details could be obtained from the anamnesis. Physical examination of the left parotid gland disclosed a mass of 3.5 cm in diameter that was not tender to palpation. The tumor was covered by a normal-appearing skin that was not attached to the deeper tissues. The remainder of the head and neck examination was normal, and there was no evidence of cervical lymphadenopathy. Radiograms of the chest and the laboratory findings were within normal limits. The mass was excised by a left superficial parotidectomy.
Macroscopic examination of the surgical specimen disclosed a yellowish gray mass, which was surrounded by normal-appearing salivary gland tissue.
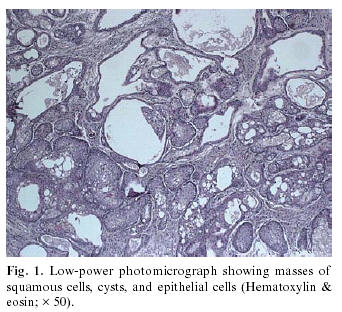
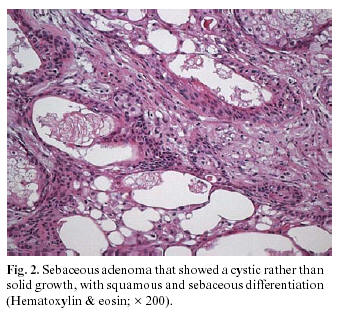
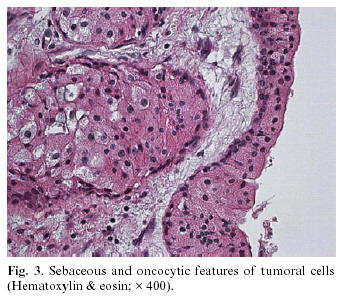
Microscopically, paraffin sections stained with hematoxylin and eosin showed a pseudoencapsulated tumor, consisting of solid masses of epithelial cells closely associated with ducts lined by two layers of cells, and broad areas of sebaceous differentiation. Occasionally, the ducts were associated with cyst-like proliferations (Figure 1) filled with a sebaceous material (Figure 2). Areas of oncocytic metaplasia were also seen (Figure 3).
A 5 year follow-up revealed no recurrence.
Discussion
Sebaceous glands can be found between 11% and 40% of all adult parotid glands (2, 5), more rarely in submandibular glands and very rarely in sublingual ones (5). The parotid gland develops from a tubular outgrowth of the mucosa that lines the oral cavity which appears at about the 45th day of the fetal life (6).
The proximal portion of this outgrowth persists as the parotid duct while the proliferation at the distal end forms the glandular parenchyma. The origin of sebaceous cells or glands within salivary gland tissue is unknown and is not attributable to an ectopia. Gnepp and Brannon (3) stated that sebaceous foci could be congenital in origin, naturally develop later in life or be due to a metaplastic process secondary to ductal obstruction. Thus, sebaceous cells represent another potential differentiation of the pluripotential salivary gland duct epithelium. Although sebaceous foci can be found in neonatal glands, their prevalence in children is lower than in later life (2) which argues against their congenital presence. Moreover, the presence of sebaceous glands and cells in major salivary glands seems to increase its incidence after puberty (5). Gnepp and Brannon (3) believe that possibly the same factors that "activate" sebaceous glands in the skin during puberty also activate those in the salivary glands.
Sebaceous adenomas are typically circumscribed and devoid of a lymphoid component. In cases in which this is present, the tumor is characterized as a different entity called sebaceous lymphadenoma, which may be solid or cystic. Sebaceous adenoma is a very uncommon salivary tumor (accounts for 0.1 percent of all salivary gland neoplasms and slightly less than 0.5 percent of all salivary adenomas) (7) and is given little attention in most pathology texts (8, 9). Foote and Frazell (10) found one parotid sebaceous adenoma in 877 tumors of the major salivary glands. Bab and Ulmansky (11) reported two cases of two different tumors of the salivary tissue occurring simultaneously in the same gland. One of these two cases corresponds to a 57-year-old woman that suffered from an adenoid cystic carcinoma and a simultaneous sebaceous cell adenoma in her right parotid gland. Pieterse and Seymour (6) reviewed 183 parotid resections. Among them, they found one case of sebaceous adenoma composed by cysts lined by multiple layers of the sebaceous-like cells. Gnepp and Brannon (3) reviewed the files of the Armed Forces Institute of Pathology which yielded 21 cases of primary salivary gland sebaceous tumors. Five of these 21 cases were sebaceous adenomas, three located at the parotid gland, one more in the submandibular gland, and the remaining case into the buccal mucosa. Of the three parotid cases, two showed a multicystic growth pattern, and the third presented an oncocytic metaplasia. Thus, as far as we know, the current case is the seventh case reported of a sebaceous adenoma located in the parotid gland. Our case showed a predominantly cystic pattern and oncocytic metaplasia. Differential diagnosis should include sebaceous lymphadenoma, sebaceous carcinoma, sebaceous lymphadenocarcinoma, and sebaceous differentiation in other tumors. Sebaceous adenomas are benign tumors that will not recur if they are adequately excised. Thus, treatment involves surgical excision.
![]() Address for correspondence:
Address for correspondence:
Prof. Dr. Juan Carlos de Vicente.
Facultad de Medicina/Odontología,
c/ Catedrático José Serrano s/n. 33006.
Oviedo. España.
E-mail: jvicente@.uniovi.es
Received: 8-03-2006
Accepted: 5-07-2006
References
1. Hamperl H. Beitrage zur normalen und pathologischen histologie menschlicher speicheldrusen. Zeit fur Mikroskopisch Anat Forschung 1931;27:1-22. [ Links ]
2. Batsakis JG, El-Naggar AK. Sebaceous lesions of salivary glands and oral cavity. Ann Otol Rhinol Laryngol 1990;99:416-8. [ Links ]
3. Gnepp DR, Brannon R. Sebaceous neoplasms of salivary gland origin. Report of 21 cases. Cancer 1984;53:2155-70. [ Links ]
4. Iezzi G, Rubini C, Fioroni M, Piatelli A. Sebaceous adenoma of the cheek. Oral Oncol 2002;38:111-3. [ Links ]
5. Linhartová A. Sebaceous glands in salivary gland tissue. Arch Pathol 1974;98:320-4. [ Links ]
6. Pieterse AS, Seymour AE. Parotid cysts. An analysis of 16 cases and suggested classification. Pathol 1981;13:225-34. [ Links ]
7. Auclair PL, Ellis GL, Gnepp DR. Other benign epithelial neoplasms. En: Ellis GL, Auclair PL, Gnepp DR, eds. Surgical pathology of the salivary glands. Philadelphia: WB Saunders Co; 1991. p. 252-68. [ Links ]
8. deBurgh Norman JE, McGurk M, eds. Color atlas and text of salivary gland diseases, disorders and surgery. London: Mosby-Wolfe; 1995. [ Links ]
9. Luna MA. Pathology of tumors of the salivary glands. In: Thawley SE, Panje WR, Batsakis JG, Lindberg RD, eds. Comprehensive management of head and neck tumors. Philadelphia: WB Saunders Co; 1999. p. 1106-46. [ Links ]
10. Foote FW, Frazell EL. Tumors of the salivary glands. Cancer 1953;6:1065-133. [ Links ]
11. Bab IA, Ulmansky M. Simultaneously occurring salivary gland tumors of different types. J Oral Surg 1979;37:826-8. [ Links ]

