










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Self-medication is integral to community pharmacists' duties to promote self-care, as advocated by the World Health Organization. 1 Community pharmacy teams (CPTs) have a critical role in managing minor health problems, assisting self-medication and promoting the safe and effective use of non-prescription medicines. 2
In Portugal, CPTs comprise an average of 3.4 registered pharmacists, one technician, and 0.4 other staff per community pharmacy (2016 data), with pharmacists and technicians legally habilitated to dispense non-prescription medicines. 3 Pharmacies have been associated with greater client satisfaction for resolving minor health problems than emergency departments and general practice; they allow for convenient access, whilst avoiding prolonged waiting times and service fees. 2
Despite its many benefits, self-medication is not without risks, namely the inappropriate medication use, which can have serious consequences, such as hospitalisations. 4 Inappropriate use of medication comprises a range of situations, such as using non-prescription medicines beyond the recommended period and exceeding the approved doses. 5 , 6
Seasonality in medicines usage can contribute to its misuse. For instance, paracetamol, present in many non-prescription cold preparations, is more frequently misused during the winter, when there is a higher prevalence of flu and colds. 7 Nonsteroidal anti-inflammatory medicines are another example of misused non-prescription medicines; an American study showed that 11% of participants used daily doses of ibuprofen over the maximum recommended. 8 Analgesics, including non-steroidal anti-inflammatory medicines, are the drugs most frequently associated with inappropriate use and hospitalisations related to selfmedication. 4 , 6 , 8 , 9
In Portugal, self-medication is a well-established and regulated practice, regarding both the medications involved and the health conditions covered. 10 , 11 The percentage of clients from rural areas acquiring a medicine that is unprescribed or orally recommended by a physician reached 21.5%, while the prevalence in urban areas matched 26.2%. 12 , 13 The previous studies have found a responsible practice, although some concerns exist about the use of certain classes of prescription-only medication, such as antibiotics. 14 , 15
If interventions by CPTs in self-medication can avert emergency care and severe harm, it is also paramount to ensure practice standards and the quality in these consultations. 16 Quality in health care entails several dimensions; attempts to measure quality in self-medication consultations encompass both the technical work of CPTs and their interpersonal conduct. 3 Clients and patient-reported outcomes are also accepted as measures of quality of care. 17
Little is known about community pharmacy clients-reported outcomes concerning self-medication consultations and their relationship with the CPTs' work performance. This study aimed to describe CPTs' practice in self-medication consultations, client-reported outcomes and satisfaction. A secondary aim was to develop an explanatory model for client satisfaction with this service.
METHODS
A descriptive cross-sectional design was adopted. Data for this study were collected as part of a more extensive investigation on the development and testing of a Balanced Score Card (BSC) for quality management of non-prescription medicines dispensing in community pharmacies, using Design Science Research Methodology (DSRM). 18 DSRM addresses any phenomena created by humans, evaluating what has been projected or what is functioning, in a rigorous and systematic process of proposing artefacts to solve problems. 19 , 20 It has demonstrated its ability to study the connection between research and professional practices by designing, implementing and evaluating artefacts that address a specific need, applied to pharmacy practice. 21
Six sites were purposively selected in Portugal to obtain diversity in critical characteristics (e.g., revenue, team's size, location). Participating pharmacies (A – F) were asked to enrol eligible clients over six months, with the help of a study leaflet, which included a written informed consent to be signed and a space for recording the phone number for later contact. Eligibility comprised an interaction where a non-prescription medicine was dispensed, in the context of a symptom-based complaint or a product-based request. To minimise selection bias, CPTs were instructed to recruit potential participants from the first non-prescription medicine dispensing in the morning and the afternoon, as long as workload allowed, up to a limit of 100 clients during the overall study period.
As part of a previous larger study, monthly meetings were held with the CPTs, during which encouragement to improve client recruitment was given. E-mail reminders were sent where client recruitment was below the target (5 per week).
A structured approach to self-medication consultations was discussed and agreed with CPTs, based on an earlier study ( Table 1 ), including quality criteria on evaluation and counselling. 3
Table 1. Approach to self-medication consultations agreed with community pharmacy teams
| Evaluation |
|---|
| Who is it for? |
| What are the symptoms? |
| How long ago did the complaint begin? |
| Action taken? |
| Medication being taken? |
| Counselling |
| Explain the action of the selected NPMs. |
| Explain the posology verbally. |
| Write the posology in the NPM package. |
| Verbally inform and/or write the treatment duration. |
| Provide supplementary information (for example, non-pharmacological measures). |
| Advise what the client should do if the symptoms persist. |
CPTs recorded pseudo-anonymised data on the client, non-prescription medicine(s) dispensed, and implemented quality criteria ( Table 1 items) in an electronic form. In cases where self-medication was deemed inappropriate, it was verified whether CPT members had referred the client for a medical consultation. These clients were excluded from the study. Self-reported criteria were tallied, receiving one point when met and zero if unmet. This classification yielded three scores: an evaluation quality score (maximum 5 points), a counselling quality score (maximum 6 points) and an overall quality score, ranging from 0 to 11.
The follow-up to ascertain client-reported outcomes and satisfaction was carried out through a telephone interview, between one week and one month after the consultation. To minimise memory bias, clients not successfully contacted up to one month were considered lost for follow-up. Telephone interviewing was used because of its potential to maximise the response rate and clarify any queries while avoiding relying on clients' next visit to the pharmacies. 22 Telephone interviews were conducted by the field researcher (a pharmacist) during the monthly visits to pharmacies A-F, after one call initiated by the pharmacy staff, with a second attempt when failing the first contact. The data collection instrument comprised a section with sociodemographic questions, followed by a section on self-reported health outcomes and a third section on satisfaction. Concerning the former, participants were inquired if they felt a little better, better, or not better at all after the self-medication consultation. Clients' satisfaction with the service was ascertained using an adapted version of the Armando et al . questionnaire, which encompasses ten items with a scale ranging from 1 (totally disagree) to 5 (strongly agree). 23 This instrument fitted the study objectives; no specific questionnaire on client satisfaction with the non-prescription medicines consultations in pharmacies was identified. Satisfaction data were converted into a composite score (“overall satisfaction”), ranging from 1 to 5, by summing items' scores and normalisation.
Data were analysed using SPSS v.18. Descriptive statistics and association tests (e.g., Chi-square) were calculated, as well as one-way ANOVA to test differences between variables. Study data was found not to be normally distributed (Kolmogorov-Smirnov Test p<0.05), but knowing one-way ANOVA is a robust test against normality violations, variables means and standard deviations (SD) are presented. To explore the possible association of several independent variables with clients' overall satisfaction (dependent variable), the SPSS linear regression function was used. This function allowed correlation and measurement of the degree of linear association between the independent (or explanatory) variables and the dependent variable. 24 The independent variables, chosen parsimoniously according to their associations with the outcome, were:
Clients' gender (dichotomous: 0 - male, 1 - female)
Age (continuous)
Level of education (categorical: 0 - no education, 1 – 1st basic cycle, 2 - 2nd basic cycle, 3 - secondary, 4 - higher)
Living alone (dichotomous: 0 - alone, 1 - not alone)
Customer loyalty, i.e., client regularly buying medicines at the specific pharmacy (ordinal: 0 - never, 1 - sometimes, 2 - always)
Evaluation score of the self-medication consultation (ordinal)
Overall quality score of the self-medication consultation (ordinal)
Typology of the self-medication consultation, i.e., symptom-based versus product-based (dichotomous)
Improvement after the self-medication interaction (dichotomous: 0 - no, 1 - yes)
Initially, univariate regressions were performed to determine a causal relationship between the chosen independent variables and the dependent variable ( Table 2 ).
Table 2. Univariate linear regressions between independent variables and the dependent variable (overall clients' satisfaction)
| Independent variable | R | Adj R 2 | F | p-value | Sth beta | t-student | p-value |
|---|---|---|---|---|---|---|---|
| Symptom complaint / NPMs request | 0.010 | -0.008 | 0.013 | 0.909 | 0.010 | 0.115 | 0.909 |
| Evaluation score of the interaction | 0.175 | 0.024 | 4.400 | 0.038 | 0.175 | 2.098 | 0.038 |
| Overall quality score | 0.023 | -0.007 | 0.072 | 0.788 | -0.023 | -0.269 | 0.788 |
| Gender | 0.170 | 0.022 | 4.184 | 0.043 | 0.170 | 2.045 | 0.043 |
| Age | 0.021 | -0.007 | 0.063 | 0.802 | -0.021 | -0.251 | 0.802 |
| If the client improved after the interaction | 0.078 | -0.002 | 0.782 | 0.378 | 0.078 | 0.884 | 0.378 |
| Educational qualifications | 0.014 | -0.007 | 0.029 | 0.865 | -0.014 | -0.171 | 0.865 |
| If the client lives alone | 0.105 | 0.004 | 1.560 | 0.214 | -0.105 | -1.249 | 0.214 |
| If the client regularly buys medicines at the pharmacy | 0.299 | 0.083 | 13.813 | < 0.001 | 0.299 | 3.717 | <0.001 |
Adj: adjusted; Std: standardized
Relevant univariate models are reported in Table 2 with (*) in the p-value column. Independent variables that did not obtain regression coefficients p-values less than 0.20 were excluded from the next step. A multiple linear regression was performed with a stepwise selection of variables to ascertain the three selected predictors' importance in explaining the overall satisfaction.
This approach yielded a model with clients' satisfaction and significant explanatory independent variables without aiming to establish predictive estimations. Thus, a set of assumptions regarding the model quality, such as residuals analysis or the orthogonality between independent variables, were not fully validated. Nonetheless, the Durbin & Watson statistic (describing the non-autocorrelation of residues), as well as their mean (which should be near to 0) and their standard deviation (ideally close to 1), were calculated. A multicollinearity diagnosis was performed using the variance inflation factor (VIF), considering the value should be less than 5. Outlier observations with a studentised residual greater than 3 standard deviations were excluded. For all analyses, a type I error probability (α) of 0.05 was considered. 24
The study was approved by the Instituto de Higiene e Medicina Tropical (IHMT) Institutional Ethics Committee, under the reference n.º 14-2016.
RESULTS
The six pharmacies recruited a total of 215 clients, of whom 135 were interviewed in a follow-up call. The distribution was as follows:
Pharmacy A: 47 clients (21.9%), 35 in the follow-up (25.9%).
Pharmacy B: 23 clients (10.7%), 7 in the follow-up (5.2%).
Pharmacy C: 45 clients (20.9%), 36 in the follow-up (26.7%).
Pharmacy D: 20 clients (9.3%), 11 in the follow-up (8.1%).
Pharmacy E: 41 clients (19.1%), 26 in the follow-up (19.3%).
Pharmacy F: 39 clients (18.1%), 20 in the follow-up (14.8%).
Clients' and CPTs' background data
Clients' mean age was 51.41 years (SD=16.76) and most were women (66.2%; n=100). Four respondents did not have any schooling (2.63%), 41 completed the 1 st basic cycle (26.97%), 35 completed the 2 nd basic cycle (23.03%), 40 completed the secondary education (26.32%), and 32 finished college education (21.05%). There were no significant differences regarding age groups and clients' gender distribution between the six pharmacies. Clients' level of education was significantly different (p=0.018) between pharmacy B and C (lower and higher education levels, respectively). Pharmacy C had the highest number of respondents with a completed college education (50%; n=16). Respondents in pharmacies A, D, E, and F had similar levels of schooling.
Overall, CPTs were comprised of 28 pharmacists (70%) and 12 other professional categories. Pharmacists were predominant in all CPT, while pharmacy A was only staffed by pharmacists. There was a significant difference among pharmacies (F=5.91; p<0,001) for the typology of self-medication consultations (symptom-based versus product-based). As depicted in Table 3 , pharmacy C had the most product-based requests, while in pharmacy F almost all consultations registered were symptom-based complaints (36 out of 39).
Table 3. Frequencies of symptom-based complaints vs. product-based requests in participating pharmacies
| Pharmacy | Symptom complaints | NPM request |
|---|---|---|
| Pharmacy A | 22 | 5 |
| Pharmacy B | 13 | 10 |
| Pharmacy C | 22 | 23 |
| Pharmacy D | 16 | 4 |
| Pharmacy E | 33 | 8 |
| Pharmacy F | 36 | 3 |
NPM: non-prescription medicines
Living alone and reporting visiting a single pharmacy (used as a proxy for loyalty) were not related with the consultation typology (p=0.224 e chi-square=1.476 and p=0.209 e chi-square=3.127). Similarly, there was no association with statistical significance between clients' gender and the typology of consultation. There was, however, a significant association between the level of education and consultation typology (p=0.001 e chi-square=15.971) i.e., clients who completed the 9th grade (basic education today) were more likely to make a product-based request and clients with high school education were more likely to present a symptom-based complaint. No significant trend was discerned for clients who completed the 4 th grade and college education.
Consultations quality
The overall results of the evaluation performed by the six pharmacies to the 215 clients were positive i.e., the five criteria were fulfilled in almost all the consultations (n=202). The exceptions were “Action taken?” not fulfilled in three consultations and “Medication being taken?” not fulfilled on thirteen occasions. Presenting a symptom-based complaint or a product-based request was not related to compliance in these five criteria.
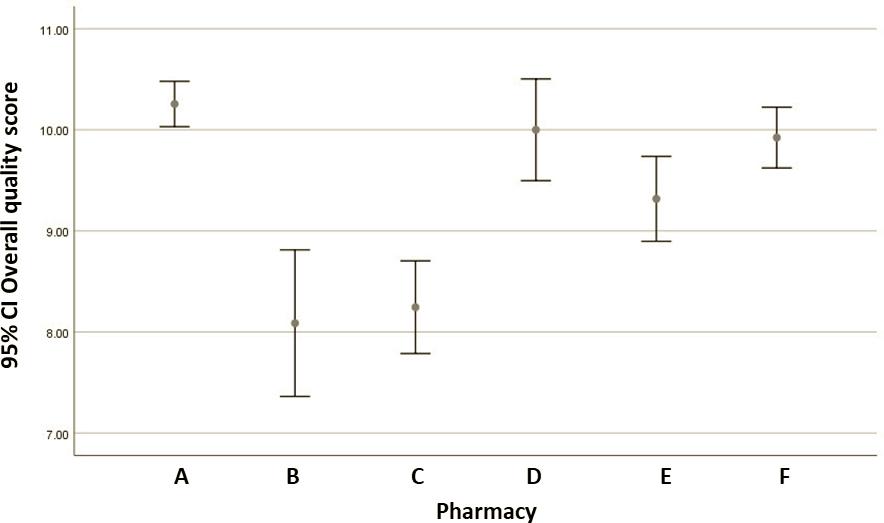
The overall quality score of the consultation differed between sites: pharmacies A, D, E, and F had significantly higher scores than pharmacies B and C ( Figure 1 ). The clients' gender, loyalty to the pharmacy and living alone were not related to the overall quality of the self-medication consultation.
Most clients (135 or 93%) reported improvement in their conditions after the consultation. Self-reported health outcomes do not appear to be significantly associated with study site, clients' loyalty, and gender, albeit all reported cases of non-improvement occurred with female clients (Table 4 ).
Table 4. Clients' self-reported outcomes
| Improved | ||
|---|---|---|
| Yes | No | |
| Pharmacy where the interaction took place | ||
| Pharmacy A | 33 | 2 |
| Pharmacy B | 14 | 3 |
| Pharmacy C | 31 | 3 |
| Pharmacy D | 11 | 0 |
| Pharmacy E | 25 | 1 |
| Pharmacy F | 18 | 1 |
| Gender | ||
| Female | 91 | 9 |
| Male | 51 | 0 |
| If the client regularly buys medicines at the pharmacy where s/he was enrolled? | ||
| Never | 7 | 1 |
| Sometimes | 57 | 1 |
| Always | 78 | 7 |
Predictors of clients' satisfaction
The mean value for clients' overall satisfaction was 4.70 (out of 5): pharmacy A=4.64, B=4.65, C=4.64, D=4.72, E=4.69, F=4.87. The initial univariate calculations with the clients' overall satisfaction as the dependent variable showed three significant independent variables: loyalty, evaluation score and gender. Although not significant, the clients' age presented a negative regression coefficient (beta= -0.250). The variables overall quality score (beta= -0.023), educational level (beta= -0.014), and living alone (beta= -0.105) correlated negatively with clients' overall satisfaction.
The stepwise multiple linear regression model confirmed the three significant predictors of the client's overall satisfaction i.e., loyalty (0-1), evaluation score (1 to 5), and gender (0-1). This model presented a multiple correlation coefficient R=0.410 and an adjusted coefficient of determination adjusted R 2 =0.150. Consequently, only 15% of the total variance in the overall satisfaction is explained by the independent variables included in this regression model. Our final adjusted model can be described as: 
where, SRCS=self-reported client satisfaction, L=Loyalty, ES=Evaluation score, G=Gender.
This means for instance that being loyal increases in about 32% the possibility of improving 1 point in overall satisfaction, while a 1-point increase in the evaluation score increases in 20% client's overall satisfaction. The model, although significant, presents a low F value (F=9.087, p<0.001) and explains a limited proportion of the overall client satisfaction. Finally, the residues were not auto-correlated (Durbin Watson=2.083) and the independent variables were not collinear (VIF=1.018). After the first model estimation, cases 7 and 130 were excluded based on their studentised residues, while the absolute mean of the residues was very close to 0.
DISCUSSION
This exploratory study indicates that CPTs'-reported compliance with quality criteria for self-medication consultations was overall high. Most clients reported a health improvement after the consultation and were overall satisfied with the service. The variables that appear to better explain overall satisfaction are pharmacy loyalty, the client evaluation score and clients' gender.
The documented self-medication consultations addressed mostly symptom-based complaints (n=142). In agreement with the literature, pharmacies that presented the highest percentage of product requests (i.e., Pharmacies B and C), scored lower in the overall quality of the consultations. 25 - 27 Although possible to confirm in other contexts, the poorer practice quality in pharmacies responding to products requests reflects the long-standing conflict between clinical and business roles. The clinical role is for long defended by national and international pharmacy organisations, contributing to a safer use of commonly taken medications, e.g., non-steroid anti-inflammatory drugs. 1 , 28 However, additional policy and educational efforts are needed to assure a valuable orientation to patient care. 29
On a positive side, the typology of the self-medication consultation i.e. product or symptom-based requests did not influence compliance with evaluation criteria, which contrasts with earlier findings. 25 - 27 The study results also contrast with a recent systematic review of CPTs diagnostic assessment and work on client consultations. 28 Sixty-three out of the 68 studies included in this review used simulated patients to assess CPTs' practice. The performance was reported as poor by study authors, regardless of geography, the scenario used, or assessment framework adopted. A possible explanation for the differences between the literature and the current findings might be a tendency to report in a manner that is viewed favourably in light of commonly accepted professional standards. A way to at least partly overcome this limitation is employing simulated patients to ascertain the validity of self-reported consultation data, an approach that is resource intensive. 4 Another possibility is checking reported practice data against videotaped consultations; however, this approach raises acceptability issues for pharmacies. Direct observation could potentially overcome the pitfalls of self-reported behaviour, but is not without limitations (e.g. Hawthorne effect).
A significant association between the level of clients' education and consultation typology was found, i.e., clients who completed the 2 nd basic cycle (basic education today) were more likely to make a product-based request and clients with high school education were more likely to present a symptom-based complaint. This could raise the hypothesis that less educated clients tend to make product-based requests while more educated clients seek advice from the CPT. The fact that no significant trend was discerned for clients who completed the 1 st basic cycle and college education may indicate this is a spurious association. Although a larger study is needed to clarify this aspect, the association between self-medication and higher education and/or professional status is well established and self-medication risks prevail. 29 - 32 Thus, independently from the type of self-medication request and the actual education level, the relevance of adequate medication-related functional literacy stands along with other essential resources for everyday life, such as informatic and economic literacy skills. 33
Most clients' (93%) reported improvement after the self-medication consultation and only 10 clients reported not being better at all. This accords with earlier findings from an observational study to ascertain the impact of pharmaceutical counselling in minor health problems in a single rural pharmacy in Portugal. 34 About 90% of the 298 participants had their minor health problems solved after one week. Nonetheless, caution is needed in interpreting our results; minor health problems may progress favourably regardless of the use of non-prescription medicines, supplementary treatments or the use of other non-prescription medicines than those suggested by CPTs, which could concur to a favourable outcome; these were not explored, and the study was not designed to establish causality. It is challenging to research the effect of self-medication consultations on health outcomes using an experimental design due to its ubiquity as standard care.
As in other studies on client satisfaction with pharmacy services, participants in the present study were overall satisfied. 35 , 36 For example, a face-to-face survey in a nationwide Portuguese representative sample of 1,114 subjects, conducted in 2015, indicated that 36% of respondents used the pharmacy as a first port-of-call to treat a minor ailment. Of those visiting a pharmacy at least once in the previous year, 94% were overall satisfied. 36 Some authors suggest these high satisfaction levels may be linked with low expectations of clients, which may evolve as they are exposed to better quality services. 35 , 37 , 38 It is, however, debatable whether clients have low expectations. A qualitative study on 21 patients enrolled in pharmaceutical care programs indicated that their expectations concerning the service were not well developed in terms of the pharmacist's role or expected outcomes, but not necessarily low, as a technical input was expected from the pharmacist. 39
The concept of client satisfaction is difficult to measure objectively, as it results from personal judgement. It is accepted that the measurement of client satisfaction reflects three important variables: personal preference, expectations about the service, and the comparison with what the service delivers (e.g., waiting times). 37 In the present study, such measurement may have reflected not only the service provided but also clients' cultural traits and expectations formed in the context of the Portuguese healthcare system. Although not significant, the negative regression coefficients of clients' age, overall quality score, educational level and living alone suggest a complex explanatory frame for satisfaction with the pharmacy services. One possible explanation relates a structured and longer interaction (i.e., with assumed higher professional quality) not to be expected or accepted by older and single living, as well as more educated clients. Further studies are needed to assess this line of reasoning.
Limitations
Community pharmacies participating in this study are not necessarily representative of Portuguese community pharmacies; these took part in a larger study and therefore could be more motivated. Also, it has been highlighted that pharmacists have better performance in self-medication consultations compared to other pharmacy staff, and they were predominant in this sample (70%). These limitations may have biased findings upwards. 2
As previously mentioned, CPTs' self-reporting is a limitation, which may have biased evaluation scores upwards. A study comparing data reported by pharmacy staff and simulated patients to researcher-assessment from audio recordings of 270 encounters indicated that staff tended to score themselves higher than the researcher. 40
In this study, instruments for measuring participants reported outcomes and their satisfaction were self-developed, based on items from various previously published papers. Limitations in instruments to measure satisfaction, such as the absence of a theoretical underpinning and psychometric assessment, were pointed out more than a decade ago and remain current. 35 The development and testing of such instruments are outside the scope of most studies attempting to measure satisfaction with community pharmacy services but represent undoubtedly an area for future research. Resorting to validated versions of international instruments internationally appears particularly promising, as it enables comparability.
Another area meriting attention is the development of core outcomes specific to self-medication consultations and a validated methodology for their measurement. 41 This would foster better evidence by those embarking on investigations of client-reported outcomes and may contribute to shift the management of minor health problems from emergency departments and general practices to community pharmacy. 41
It was not conceivable to reach direct access to the participating clients' mobile phone number, so there was a variation between one week and one month in contacting those clients. As such, clients who were contacted later after receiving the service may have suffered from memory bias. 42 Also, due to the sample characteristics (e.g. small size and non-normally distributed) and regression model parameters (e.g. small amount of explained variance), caution should be taken when interpreting or extrapolating results.
CONCLUSIONS
CPTs reported high performance concerning quality criteria for self-medication consultations. Clients reported a high rate of improvement and high satisfaction with these consultations. Assisting clients in self-medication appears to determine overall satisfaction, as well as pharmacy loyalty and clients' gender. However, these variables are limited in explaining satisfaction. A future study is warranted, with a larger sample, a standardised method for measuring client-reported outcomes and more variables as potential predictors. Studying the weights clients may assign to different variables is also essential to yielding a valid and reliable prediction model of clients' satisfaction.

