










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista de Osteoporosis y Metabolismo Mineral
versión On-line ISSN 2173-2345versión impresa ISSN 1889-836X
Rev Osteoporos Metab Miner vol.13 no.2 Madrid jun. 2021 Epub 16-Ago-2021
https://dx.doi.org/10.4321/s1889-836x2021000200008
IMAGES IN OSTEOLOGY
Maxillary metastasis due to pulmonary myofibroblastic tumor detected in study [18-F] FDG PET/CT
1 Nuclear Medicine Service. Virgen Macarena University Hospital. Seville (Spain)
2Oral and Maxillofacial Surgery Service. Virgen Macarena University Hospital. Seville (Spain)
We present the case of a 62-year-old woman with a history of a fibrohistiocytic variant of a pulmonary inflammatory myofibroblastic tumor treated by a lobectomy of the right lower lobe and lymphadenectomy of the intrapulmonary area and pulmonary ligament, and a history of tooth extraction 11 due to a vestibular fistula torpid.
In a control [18-F] FDG PET/CT study, a solitary hypermetabolic lesion suggestive of malignancy was observed in the gingival area of the upper jaw (Figure1 A-C) and 3D reconstruction (Figure 2).
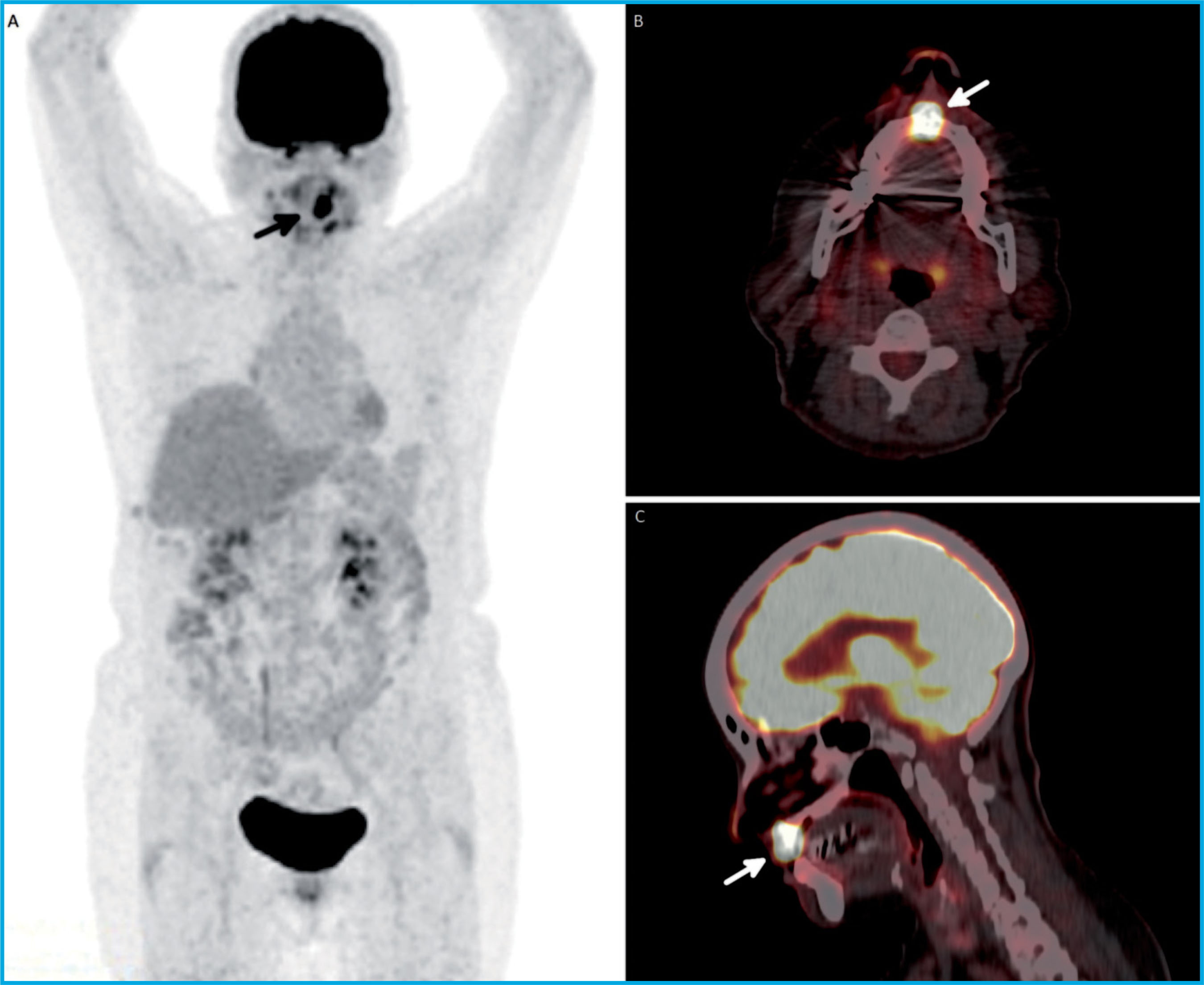
Figure 1. Study [18-F] FDG PET/CT in which a solitary hypermetabolic lesion is observed in the gingival area of the upper jaw (SUVmax 27), which corresponds in the morphological image to an exophytic lesion located on the extraction of the tooth 11 in the maximum intensity projection (MIP). (Figure 1A, arrow), axial section (Figure 1B, arrow) and sagittal section (Figure 1C, arrow)

Figure 2. 3D reconstruction of study [18F] FDG PET/CT that identified a hyper-metabolic lesion on an exophytic lesion located on the extraction of tooth 11 (arrow)
Given the suspicion of malignancy, a partial maxillectomy of teeth 13-23 was carried out with placement of an obturator prosthesis. Analysis confirmed the metastatic etiology by observing hypercellular areas with a fasciculate pattern and broader sarcomatoid areas. Immunohistochemical analysis showed strong ALK expression, higher FLI1 expression, and lower CD10 and TLE1 expression. At present, the patient remains asymptomatic.
Inflammatory myofibroblastic tumor (IMT), also known as inflammatory pseudotumor, xanthoma, plasma cell granuloma, pseudosarcoma, lymphoid hematoma, myxoid hamartoma and inflammatory myofibrohistiocytic proliferation1,2, is an uncommon neoplastic growth of mesenchymal proliferation and myofibroblast line at the expense of myofibroblasts. an obvious inflammatory infiltrate composed of plasma cells, lymphocytes, and eosinophils1-4. This has generally been considered a benign tumor. At present, it is considered a neoplasm of intermediate malignancy, however, as it has a tendency to local aggressiveness and recurrences and, on rare occasions, may trigger distant metastases1-4. The etiology is unknown at this point in time, although inflammation, autoimmunity and previous infections are suggested as possible causes1-4. IMT may be found in a wide variety of locations, the most common being the pulmonary location, followed by the abdominal, skin, soft tissue, genital, and mediastinum. It is typical of pediatric age and young adults2.
Normally, IMT presents asymptomatically, being detected as an incidental finding in a radiological test, although it can occasionally produce symptoms secondary to mass effect and nonspecific symptoms such as weight loss, anemia or fever secondary to the production of cytokines (mainly IL-1)3. It is necessary to perform a differential diagnosis against other non-neoplastic entities such as reparative, autoimmune or postinfection processes2,4.
The [18-F] FDG PET/CT study is a very useful diagnostic test in the evaluation of the cancer patient. [18-F] FDG is a glucose analog that accumulates in body cells in proportion to glucose utilization. The accumulation of [18-F] FDG in most tumor cells by over-expression of the GLUT-1 transporter is characteristic, although active inflammatory processes can also present a physiological increase in [18F] FDG in granulocytes and mononuclear cells. IMT can show a heterogeneous uptake of [18F] FDG that can be explained by the variability of cellularity, the rate of cell proliferation and nuclear atypia of tumor cells, as well as the composition, proportion and activation of inflammatory cells1,3,4. The treatment of choice is complete surgical resection, being curative in 90% of cases. It has been shown that previous steroidal or non-steroidal anti-inflammatory treatment can be useful to reduce tumor size, in local recurrences or in unresectable tumors1-4.
In conclusion, we present the detection by an [18-F] FDG PET/CT study of a metastasis in the head and neck region due to a tumor that rarely presents distant metastatic involvement.
Bibliografía
1 Ma C, Lu J, Chen G, Wang W, Su F, Su X. Inflammatory myofibroblastic tumor mimicking lymphoma on 18F-FDG PET/CT Report of a case and review of the literature. Hell J Nucl Med. 2018;21(1):77-80. [ Links ]
2 Alshammari HK, Alzamami HF, Ashoor M, Almarzouq WF, Kussaibi H. A Rare presentation of inflammatory myofibro-blastic tumor in the nasolabial fold. Case Rep Otolaryngol. 2019; 2019:3257697. [ Links ]
3 Díaz Silván A, Allende Riera A, Cabello García D, Vilahomat Hernández O, Martínez Gimeno E. Inflammatory myofibro-blastic tumor 18F-FDG PET/CT findings. Rev Esp Med Nucl Imagen Mol. 2019; 2019;38(3):190-191. [ Links ]
4 Dong A, Wang Y, Dong H, Gong J, Cheng C, Zuo C, et al. Inflammatory myofibro-blastic tumor: FDG PET/CT findings with pathologic correlation. Clin Nucl Med. 2014;39(2):113-121. [ Links ]
Received: March 10, 2021; Accepted: April 10, 2021
 Este es un artículo publicado en acceso (Open Access) abierto bajo la licencia Creative Commons Attribution Non-Commercial, que permite su uso, distribución y reproducción en cualquier medio, sin restricciones siempre que sin fines comerciales y que el trabajo original sea debidamente citado.
Este es un artículo publicado en acceso (Open Access) abierto bajo la licencia Creative Commons Attribution Non-Commercial, que permite su uso, distribución y reproducción en cualquier medio, sin restricciones siempre que sin fines comerciales y que el trabajo original sea debidamente citado.
