



![Metástasis maxilar por tumor miofibroblástico pulmonar detectada en estudio [18F]FDG PET/TC](/img/es/prev.gif)






Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista de Osteoporosis y Metabolismo Mineral
versión On-line ISSN 2173-2345versión impresa ISSN 1889-836X
Rev Osteoporos Metab Miner vol.13 no.2 Madrid jun. 2021 Epub 16-Ago-2021
https://dx.doi.org/10.4321/s1889-836x2021000200009
IMAGES IN OSTEOLOGY
Multidisciplinary approach to diagnostic imaging in melorheostosis
2Nuclear Medicine Clinical Management Unit, Virgen Macarena University Hospital. Sevilla (Spain)
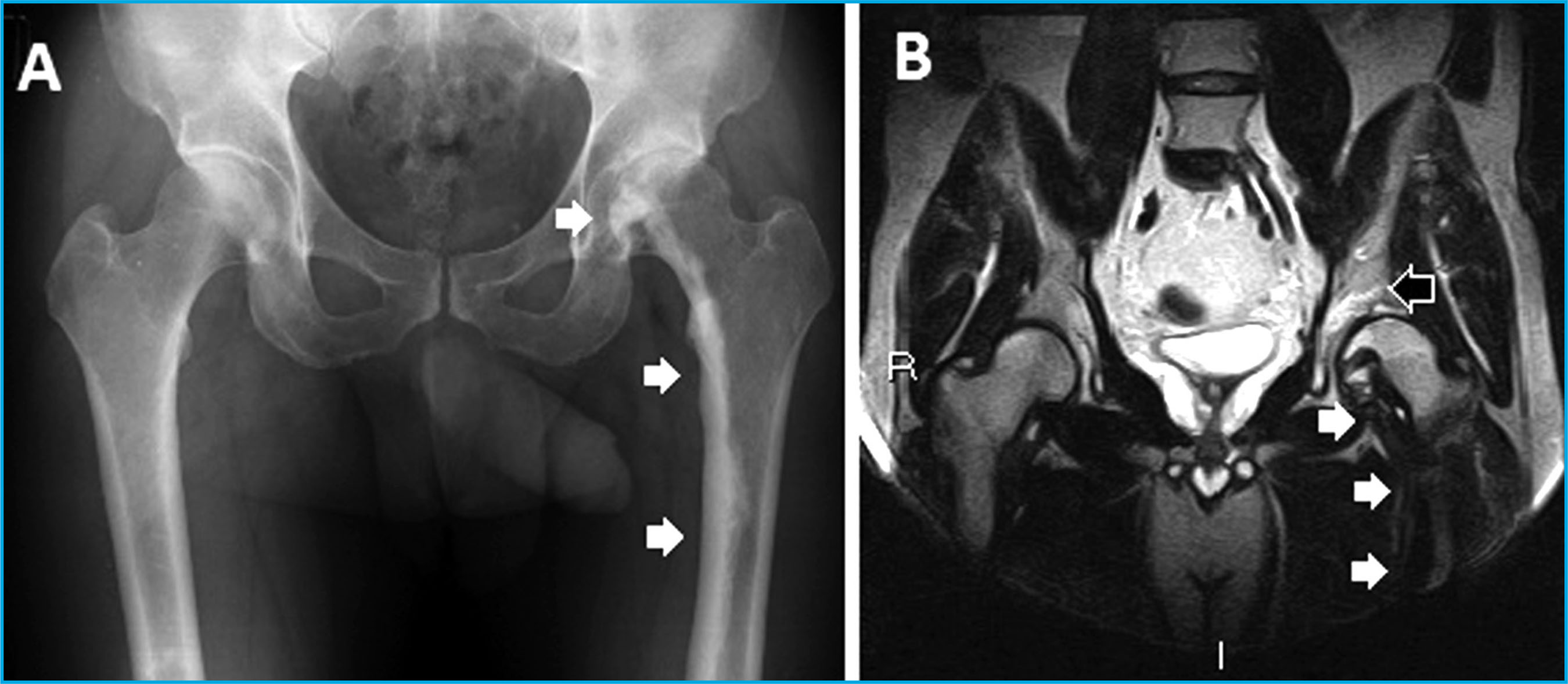
We present a 44-year-old man with a history of multiple trauma in childhood and trauma to the left hip eight months before the consultation, who consulted for pain of short duration (5 days) in the left hip, presenting limited range of movement on physical examination in the extreme degrees of the left hip, without signs of local infection or laboratory abnormalities. The x-ray of the hips (Figure 1A) showed periosteal hyperostosis along the inner cortex of the left femur (white arrows), giving rise to a characteristic image of "molten wax dripping down the side of a candle". (Figure 1B) Cortical thickening appeared as hypointense in all image sequences (white arrows), in addition to showing bone edema of the femoral head related to degenerative joint disease (black arrow). A bone gamma scan study was requested.
The early phases of the bone gamma scan study with 28 mCi (1036 MBq) of Tc99m-MDP (Figure 2) showed increased vascularity in the left hip (black arrows). The late full-body image highlighted the focal uptake of the radiotracer in the upper region of the femoroacetabular joint (black arrow), corresponding in the SPECT/CT fusion images with an area of sclerosis and degenerative joint disease. In addition, another deposit of less intensity was identified in the left femoral shaft (white arrows), in relation to the radiological thickening of the inner edge of the cortex seen in the fused images.

Melorrheostosis is a benign bone dysplasia that predominantly affects the appendicular skeleton and adjacent soft tissues1. The bone distribution is usually asymmetric2 and can be monostotic or polyostotic. It is caused by an abnormality of embryonic development Diagnosis is often made by conventional radiography, by with a sclerotome distribution3. There is no standard identifying cortical hyperostosis with a "candle wax" treatment, so it must be planned individually. The effi-image6,7. Since laboratory tests are normal, the bone cacy of bisphosphonates on pain has been described4,5, scan pattern is crucial for the differential diagnosis of but in some cases corrective surgery for bone deformi-other infiltrative diseases and other osteodysplastic ties and osteodegenerative sequelae may be necessary. syndromes8,9.
Bibliografía
1 Ashish G, Shashikant J, Ajay P, Subhash D. Melorheostosis of the foot: A case report of a rare entity with a review of multimodality imaging emphasizing the importance of conventional radiography in diagnosis. J Orthop Case Rep. 2016;6:79-81. [ Links ]
2 Sonoda LI, Halim MY, Balan KK. Detection of extensive melorheostosis on bone scintigram performed for suspected metastases. Clin Nucl Med. 2011;36:240-241. [ Links ]
3 Murray RO, McCredie J. Melorheostosis and the sclerotomes: a radiological correlation. Skeletal Radiol. 1979;4:57-71. [ Links ]
4 Ben Hamida KS, Ksontini I, Rahali H, Mourali S, Fejraoui N, Bouhaouala H, et al. Révélation atypique d'une melorhe-ostose améliorée par du pamidronate. La tunisie Medicale. 2009;87:204-206. [ Links ]
5 Donath J, Poor G, Kiss C, Fornet B, Ge-nant H. Atypical form of active melorheostosis and its treatment with bisphosphonate. Skeletal Radiol. 2002; 1:709-713. [ Links ]
6 Campbell CJ, Papademetriou T, Bonfi-glio M. Melorheostosis: a report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am. 1968;50:1281-1304. [ Links ]
7 Slimani S, Nezzar A, Makhloufi H. Successful treatment of pain in me-lorheostosis with zoledronate, with improvement on bone scintigraphy. BMJ Case Rep. 2013 Jun 21;2013:bcr 2013009820. [ Links ]
8 Janousek J, Preston DF, Martin NL, Robinson RG. Bone scan in melorheosto-sis. J Nucl Med. 1976.12:1106-1108. [ Links ]
9 Elsheikh AA, Pinto RS, Mistry A, Fros-tick SP. A unique case of melorheosto-sis presenting with two radiologically distinct lesions in the shoulder. Case Reports in Orthopedics. 2017;2017: 9307259. [ Links ]
Received: March 18, 2021; Accepted: April 18, 2021
 Este es un artículo publicado en acceso (Open Access) abierto bajo la licencia Creative Commons Attribution Non-Commercial, que permite su uso, distribución y reproducción en cualquier medio, sin restricciones siempre que sin fines comerciales y que el trabajo original sea debidamente citado.
Este es un artículo publicado en acceso (Open Access) abierto bajo la licencia Creative Commons Attribution Non-Commercial, que permite su uso, distribución y reproducción en cualquier medio, sin restricciones siempre que sin fines comerciales y que el trabajo original sea debidamente citado.
