










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
COVID-19 pandemic has caused heavy burden on countries around the world, forcing governments to take radical measures including lockdown, trade limitations, health emergency measures, and fiscal changes [1]. On January 17 2022, there were about 326,279,424 confirmed cases of COVID-19 globally with an estimated 5,536,609 deaths [2]. The WHO weekly epidemiological update of the 19th to the 25th January 2022 indicated that COVID-19 cases had increased by 5% globally, and that about 21 million new cases were reported across the six WHO regions with the largest increase in new cases in the Eastern Mediterranean Region (39%) [3]. Africa, with its limited resources, continues to depend on international intervention for vaccine and drug development as well as procurement. On January 12, 2022, the African continent had registered 10,201,488 cases of COVID-19, with a total death of 232,770 [4]. At the same date, the rate of vaccination on the continent was 60.50% of the supplied doses, with 14.92% of the population partially vaccinated and 10.09% of the African population fully vaccinated not counting booster shots [4]. Just like many other viruses, SARS-CoV-2 consists of a microscopic infectious agent in which the genetic code is enclosed by a coat essentially made of proteins, which cannot live outside the host cells that assure its survival and replication [5]. One of the best ways to prevent SARS-CoV-2 is through vaccination. Immunization helps the body to produce memory cells, which remember the infectious agent and how to fight it [6]. Hence, when the body is infected by the pathogenic agent, the immune system acts faster and vigorously, producing a secondary immune response instead of a primary response [7]. SARS-CoV-2 has on its surface a glycoprotein, which forms the spike protein essential for the virus' entry into living cells. So, the entry of the virus in human cells is made possible through the interaction between the virus receptor-binding motif (RBM) and the angiotensin converting enzyme 2 (ACE2) of human cells [8].
New vaccines including mRNA vaccine have revolutionized the field of vaccinology and has shown tremendous results in the fight against SARS-CoV-2. When infection by SARS-CoV-2 occurs, the immune system uses antibodies to block the virus' spike protein. The mRNA vaccine in this case contains the message to produce the spike protein, which in turn triggers the body to produce antibodies against the spike protein of SARS-CoV-2 [9]. Therefore, after immunization with the vaccine, a contact with the virus will cause naïve B-cells to quickly proliferate, differentiate, and produce a class of antibody that will block the spike protein of the SARS-CoV-2 and so prevent entry of the virus into host cells. This process is crucial in stopping the virus, reducing disease severity as well as viral mutation.
The abovementioned process puts into perspective the advantages procured by vaccines from the point of view of infection and disease prevention. Nevertheless, this advantage remains futile when vaccine efforts fail to cover a critical number of people in the population. For a vaccine to be effective against a pandemic such as COVID-19, vaccine rollout should be optimized globally and cover enough people to prevent the virus from breaking through the immunologic barrier built at the ecologic level [10]. In case of failure, the risk of facing new variants of SARS-Cov-2 resulting from viral mutation grows. This mutation undermines the energy put in vaccine development as well as the capacity of the vaccine to contain the pandemic. Such a situation explains the emergence of new variants of SARS-CoV-2 including the Delta variant, and the Omicron variant, which have made the headlines in past months. Unfortunately, many regions of the world fall through the cracks and fail to deploy an effective and large-scale vaccination program capable of stopping viral mutations. Africa is particularly faced with the challenge of low vaccine uptake, which feeds on several limitations ranging from inadequate capacities and resources, poor health systems, and more importantly the growing impact of vaccine hesitancy across the continent [11, 12]. As countries and subregions on the continent have different outcomes, it is important to evaluate those differences to improve orient vaccination program efforts, to increase setting-appropriate strategies for vaccine uptake, and to foster interregional and countries' collaboration. In this paper, we seek to fill this gap by providing an analysis of regional variations in COVID-19 death outcomes and vaccine status across Africa.
MATERIAL AND METHODS
DATA SOURCE AND VARIABLES
The data were extracted from the Johns Hopkins Coronavirus Resource Center (CRC) database, which is supported by Bloomberg Philanthropies and the Stavros Niarchos Foundation [13]. The data used in this analysis were collected between the periods of December 30, 2021, to January 2, 2022. The downloaded data included all relevant, accumulated data collected since the beginning of the pandemic. The variables collected were confirmed cases (the total number of confirmed cases since the beginning of the pandemic); doses administered (the total doses of vaccines administered); fully vaccinated (the total number of fully vaccinated people; fully vaccination being the number of doses required depending on the vaccine type), and total deaths (the total number of deaths attributed to COVID-19). Since we are interested in regional differences, these data are based on geographical location; hence countries are grouped by region (North, Central, West, East, and Southern) instead of population size or per capita. With 50 countries in Africa, a sample of 30 countries is enough to provide a trend regarding vaccine status on the continent and six countries per region is sufficient to make a comparison, especially given that some regions have just about six countries.
STUDY DESIGN
Given that the data present a snapshot of different variables at a certain point in time, a cross-sectional ecological study design was selected. Five regional groups were examined in the analysis: West Africa, Central Africa, East Africa, Southern Africa, and North Africa. Six countries were randomly chosen from each of these five regions. The data are grouped according to these five regions (Figure 1). All data (confirmed cases, doses administered, fully vaccinated, and total deaths) are sums of continuous variables. They are therefore treated in the analysis as continuous variables classified in five groups.
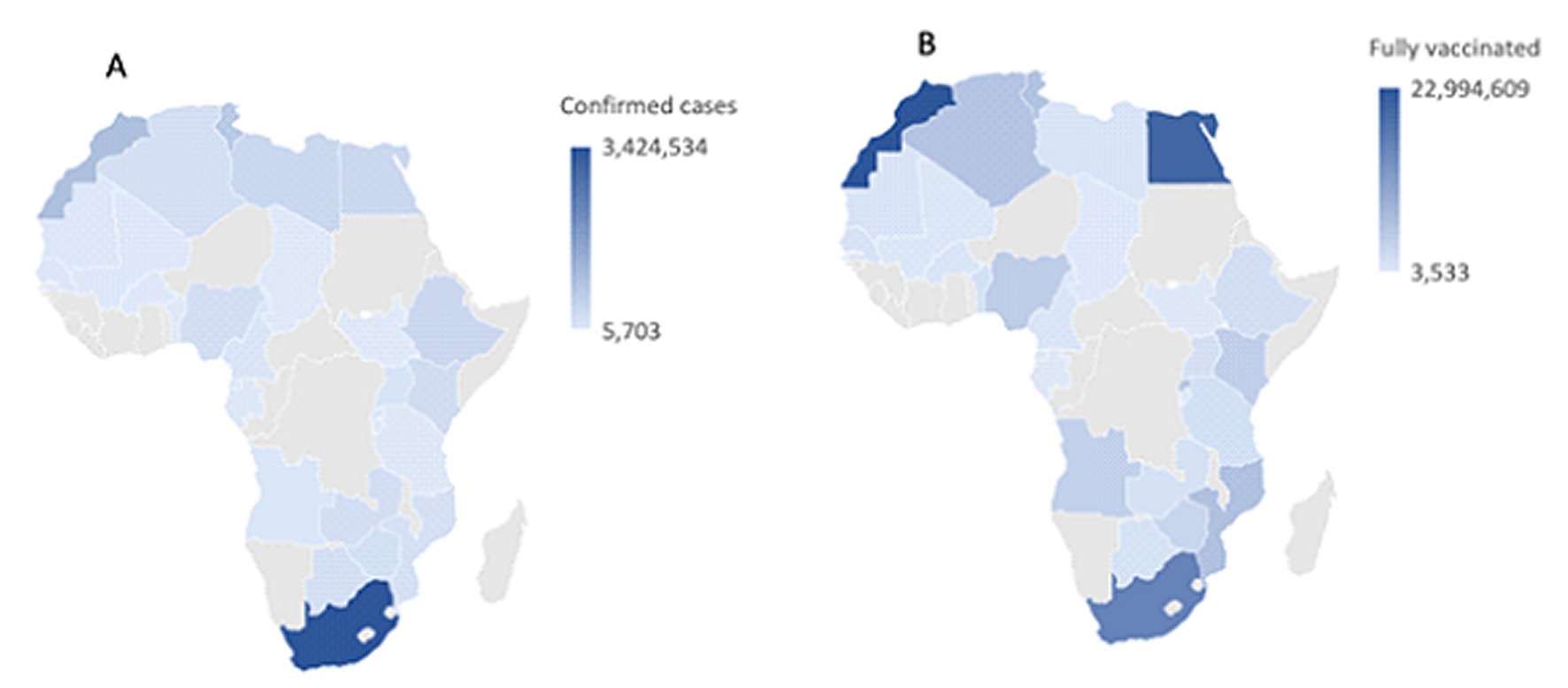
Figure 1 A: Geographical distribution of total number of confirmed cases across the African countries randomly selected. B: Geographical distribution of the total number of fully vaccinated people across the African countries randomly selected.The maps were generated using Microsoft Excel Workbook (.xlsx).
STUDY SETTING
The CRC is a repository of global data on COVID-19 pandemic. Its focus on cases, deaths, tests, hospitalizations, and vaccines offers an opportunity to evaluate how different parts of the world are faring, to provide the best response. This study examines the effect of the pandemic on the African continent regarding cases, death toll, and vaccination status. These data provide an opportunity to evaluate and compare the geographical regions that often form political entities. Such a study provides information about the pandemic in Africa, casting light on which regions of the continent need more attention. It also provides some directions in terms of regional collaboration to curb the pandemic.
STATISTICAL ANALYSIS
Data on confirmed cases, doses administered, number of fully vaccinated individuals, and total deaths were extracted from the CRC website [13]. Each variable represented an accumulation of data grouped by country. To visualize the distribution of total doses administered, and the total of fully vaccinated people by country grouped in subregions, we generated a histogram (Figure 2) using Microsoft Excel Workbook (.xlsx). For the total sample of 30 countries, we calculated the total for each of the four variables and grouped them by geographical regions (Table 1). We carried out ANOVA tests to evaluate the effects of subregion and confirmed cases on deaths, subregion and fully vaccinated on deaths, and subregion and doses administered on deaths. The Bonferroni correction helped evaluate the means difference between subregions with the three variables combined in the model. The results a represented in Table 2.
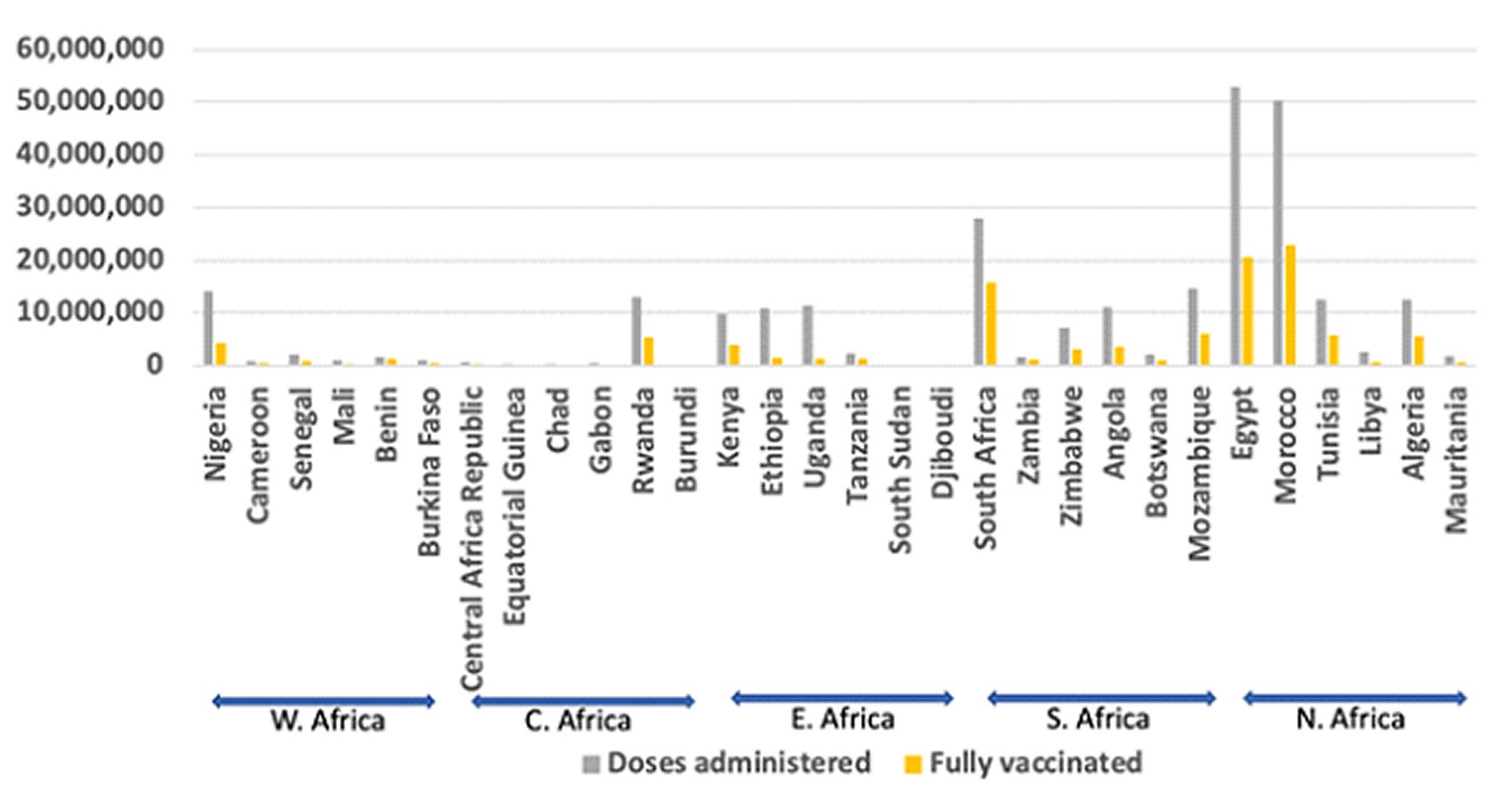
Figure 2 A: Distribution of total doses administered and total number of fully vaccinated persons across the five regions. From left to right each group of six countries correspond to a region, West Africa, Central Africa, East Africa, Southern Africa, and North Africa, respectively.
Table 1. Proportions of total confirmed cases, total doses of vaccine administered, total number of fully vaccinated people, and total number of deaths by region
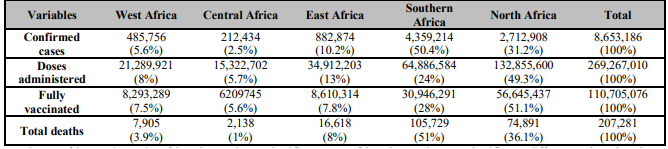
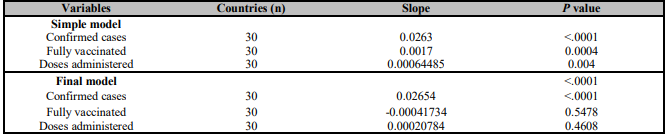
Table 2. Student and ANOVA tests to evaluate the effects of subregion and confirmed cases on deaths, subregion and fully vaccinated on deaths, subregion and doses administered on deaths. ANOVA evaluates the effects of subregions and the three other variables combined on deaths

We assessed the relationship between total deaths and confirmed cases, doses administered, and the number of fully vaccinated individuals. This was done through a correlation test with the results summarized in Table 3. A multiple linear regression further estimated this relation captured in Table 4. The multiple regression formula is specified as follow:
Where Y is the outcome of death, the model intercept, the total doses of vaccines administered, the total number of fully vaccinated people, the total number of confirmed cases, and the model deviation. We used SAS® OnDemand for Academics to perform all statistical tests.
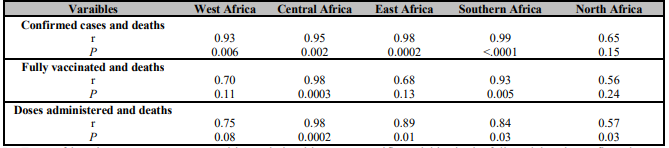
Table 3. Correlation test to evaluate the existence of a relationship between the total number of deaths and total number of confirmed cases, total number of fully vaccinated individuals, and total doses of vaccine administered in the five regions (r = correlation coefficient)
RESULTS
North African countries tended to do better in terms of doses of vaccines administered and fully vaccinated people (49.3% and 51.1% respectively) (Figure 1). They are followed by Southern Africa (24% and 28.8%) and East Africa (13% and 7.8%). West Africa (8% and 7.5%) and Central Africa (5.7% and 5.6%) have the lowest proportions of doses administered and fully vaccinated people. However, the highest death toll was in Southern Africa (51%) and the lowest in Central Africa (1%).
To determine regional differences and the vaccination effects on deaths, we used Student test and ANOVA test with Bonferroni correction. The effect of the number of confirmed cases on deaths across regions is a statistically significant (P<.0001). There was a regional difference in the effect of confirmed cases on deaths. The same was true for fully vaccinated (P=0.01). The effect of doses administered and subregion on deaths was not significant, but the overall model (with the three variables and subregions effect on deaths) was significant (P<.0001) (Table 2).
Southern Africa and North Africa do not have significant difference in means of confirmed cases. Likewise, Central Africa, West Africa, and East Africa do not have significant difference in means of confirmed cases, but there is a difference between Southern Africa and North Africa when compared to Central Africa, West Africa, and East Africa. There is no significant means difference in fully vaccinated among the five regions. Southern Africa and North Africa do not have significant difference in means of doses administered. Likewise, Central Africa, West Africa, and East Africa do not have significant difference in doses administered, but there is a difference between Southern Africa and North Africa when compared to Central Africa, West Africa, and East Africa. The overall model evaluating the effect of the three variables and subregions on deaths is significant as shown in Table 2. Southern Africa and North Africa do not have a significant difference, but they have worse outcomes in terms of death toll with higher means deaths. Central Africa, West Africa, and East Africa are not significantly different, but there is a difference when comparing Southern Africa and North Africa with Central Africa, West Africa, and East Africa.
The effects of the three variables on deaths were further evaluated through correlation tests (Table 3). The results showed that we could not be confident in saying that a relationship exists between confirmed cases and deaths, number of fully vaccinated individuals and deaths, or doses administered and deaths in the North African group. In the Southern African group, a strong positive relation exists between confirmed cases and deaths (P<.0001, r=0.99), fully vaccinated and deaths (P=0.005, r=0.93), and doses administered and deaths (P=0.03, r=0.84).
In East Africa there was a strong positive relationship between confirmed cases and deaths (P=0.0002, r=0.98), and doses administered and deaths (P=0.01, r=0.89). In Central Africa a strong positive relationship was also found between confirmed cases and deaths (P=0.002, r=0.95), fully vaccinated individuals and deaths (P=0.0003, r=0.98), and doses administered and deaths (P=0.0002, r=0.98). The same was not true in West Africa where a strong positive relationship only exists between confirmed cases and deaths (P=0.006, r=0.93).
The multiple linear regression helped estimate the relationship between deaths and the three variables. The simple regression models showed that a linear relationship exists between deaths and confirmed cases (P<.0001) in the 30 countries taken together (Table 4), as would be expected. Similarly, in the simple regression models, there is a positive linear relationship between the number of fully vaccinated individuals and deaths (P=0.0004), and between doses of vaccines administered and deaths (P=0.004). The multiple regression overall model is statistically significant for all the 30 countries combined (P<.0001). However, when looking at specific variables in the full model, only confirmed cases had a significant linear relationship with deaths (P<.0001).
DISCUSSION
Many obstacles in Africa have hampered COVID-19 vaccine campaigns. Many African countries have been unable to procure vaccines in a timely fashion. The failures of COVAX, and vaccine procurement arrangements by high-income countries, which gobbled up existing supply, are the main reasons [14, 15]. There are also significant country-specific variations in terms of government interest in acquiring vaccines, and in terms of fiscal capacity to do so [16]. Vaccine hesitancy has also slowed down vaccine uptake in Africa. Although the movement has been more explicit in developed countries, a similar tendency has been seen in African countries and factors including miscommunication, lack of trust, past experiences with health services, family histories, and rumours, might have nurtured the current trend [17]. The continent continues to lag in terms of vaccine rollout [18], and that remains a concern because areas with low vaccination rollout represent the bedrock for new viral mutations leading to the rise of new COVID-19 strains. The differences in vaccine rollout performances observed among African regions provides an idea about where the continent struggles the most. North African countries and Southern Africa countries have better performances in terms of doses of vaccines administered as well as number of fully vaccinated people [13]. Western and Central African countries have the poorest performances. This suggests that continental and global efforts for vaccine uptake should focused more on these latter regions.
As shown in Table 2, the effect of total doses of vaccine administered, total fully vaccinated people, total confirmed cases, and total deaths show that there is a difference in means among regions. This indicates that some regions do better than others do. North Africa and Southern Africa are particularly different from Central, West, and East Africa. With higher means deaths, North Africa and Southern Africa have worse outcomes when compared to West Africa, Central Africa, and East Africa. This indicates that, despite their higher vaccine rollout, North and Sothern Africa have not made a significant difference in preventing deaths when compared to the other regions. This might be an indication that more efforts should be put in prevention measures in the hot spots of these two regions. This is crucial in the context of the B.1.1.529 variant, which has several mutations capable of conferring high infectivity on it as well as immune evasion capacity [19]. The difference in death outcomes increases the need for better surveillance and testing across regions since these factors can confound the results. Difference in population demography, comorbidities, and preventive measures can also explain the differences. As indicated in Table 3, the positive relationship and the lack of negative relationship found between deaths and confirmed cases, deaths and doses administered, and deaths and the fully vaccinated implies that the vaccine effort is not yet sufficient to curb the death toll. This might suggest that all the regions on the continent still need renewed vaccination efforts to reduce COVID-19-related morbidity and mortality. This is consistent with the positive linear trend found between total deaths and the three variables under consideration in Table 4. Vaccine rollout is a time sensitive race. Vaccination significantly reduces the risk of hospitalization, disease progression, and infectivity [20]. However, these benefits are only meaningful when enough people are immunized within the appropriate timeframe. That is why more programs geared at scaling up vaccine rollout in Africa should be considered.
The fact that some countries on the continent do better than others in terms of COVID-19 management opens doors for international collaboration especially with vaccine programs, social media handling and communication, physicians, and other health professionals and their input. It is well known that countries are always geared to seeking their own interests by putting their people first; and without an international government, the world is in a constant state of chaos particularly in times of crisis [21, 22]. Furthermore, states always tend to increase their power, relative to other states [23]. Nevertheless, in the context of a pandemic such as COVID-19, there is a need for better collaboration and exchange. The fact that some countries on the continent do better than others opens the door for international collaboration, especially with vaccine programs, public communication, health professionals, and other stakeholders' inputs. The South African government has used several tactics in their communication campaign that helped vaccine rollout a great deal. South Africa's incorporation of partners that are not part of the pharmaceutical and health sector, including businesspersons, labour and civil society contributed to the success of the vaccine campaign [24]. By December 13, 2021, South Africa had administered 82% of vaccine doses that they had procured; a rate substantially higher than Egypt (52%), Nigeria (48%), Cameroon (23%) and DR Congo (5%) at the same date [25]. Those experiences can be shared at the regional and continental level to help poor performing countries while taking into consideration the socio-cultural setting of each country. Collaboration among African countries, as well as sharing of resources, information and technology can represent a decisive element in scaling up vaccine uptake. There is also a need to have a global rhetoric on vaccines, which is context sensitive, innovative in terms of technology, and driven by the socio-ecologic model [26]. The African experience of vaccination is sharply different from the European's, North American's, and even Asian's. Hence, a global rhetoric that seriously considers the African lived experience can win the battle over mistrust, misinformation, myths, conspiracy theories, and vaccine hesitancy [27]. COVID-19 vaccines received an unprecedented opposition among many populations. The rapidity with which COVID-19 vaccines were developed is one of the causes of mistrust even among qualified health professionals [28]. The recent findings showing evidence of intracellular reverse transcription of Pfizer BioNTech COVID-19 mRNA vaccine BNT162b2 in vitro in human liver cell line [29] is an indication that more and better communication is needed from the biotech and pharmaceutical companies. The effort to scale up vaccine rollout must be multi-sectorial. The input of international organizations and a country's government should be coupled with the contribution of health professionals, civil society, the business community, scholars, researchers, and community leaders, to mention the most obvious.
The study has some limitations as the data used may include mistakes through the process by which they were collected. In the context of a pandemic, many cases go unreported and unaccounted for; hence, these data can only provide an approximation about the ongoing trends and cannot infer a causal relationship. The data on deaths were considered from around the beginning of the pandemic and not after the beginning of vaccine rollout. This might affect the degree of relationship between deaths and vaccination status, given the effects of preventive measures including face masking, hand hygiene, and physical distancing. However, since most of these measures continued even after the beginning of vaccine rollout, we considered that these effects are most likely levelled up. Moreover, many African countries did not particularly succeed with these measures especially physical distancing, masking, and contact tracing [30]. The effects of these measures are accounted for by the standard error in the regression model. The social context, including unrest, political strife, variations in infrastructures can affect vaccine rollout from one country to another. This study is also limited in the sense that it does not take into consideration the ratio of each variable to each country general population and total subregional populations. Nevertheless, the study provides an insight into the difference in vaccine status, confirmed cases, and their relation to death outcome due to COVID-19 in the African subregions investigated. This study focused on regional and geographical based differences. Next steps can evaluate differences through grouping countries by factors including per capita income, population size, and similarities in health systems.
CONCLUSIONS
Vaccination offers one of the best ways to battle infectious diseases and remains efficient in the context of a pandemic such as COVID-19. Widespread vaccination coverage is also pivotal in suppressing the emergence of new strains of the pathogen. Hence, vaccination is crucial in the fight against COVID-19, especially in the African context, which is characterized by weak health systems and limited resources that make treating large numbers of individuals in pandemic surges challenging. This study indicates that African regions have performed differently in terms of vaccine rollout, with the best performances observed in North and Southern Africa. West and Central Africa present the lowest performances. The study also indicates a relationship between total doses of vaccine administered and the total number of deaths, the number of total fully vaccinated people and the total number of deaths. However, vaccination is not yet adequate to reduce total deaths to the point of producing a significant negative linear relationship. These suggest that increasing vaccination coverage can positively change the trend of the pandemic in Africa, by reducing deaths as well as severe forms of the disease.

