










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
A healthy and well balanced diet has a significant impact on body health and could control various nutrition-related diseases such as obesity, diabetes, and cardiovascular diseases. Particularly, around 73 % of deaths in Saudi Arabia are related to non-communicable diseases (1). A study on the prevalence of the chronic disease among elderly Saudi men showed a high percentage of obesity (77.8 %), followed by hypertension (71.3 %), diabetes (27.3 %), heart disease (16.4 %), asthma (9.7 %), ulcer (8.9 %), and cancer (2.0 %), respectively (2). On the other hand, iron-deficiency anemia was highly prevalent in females (94 %) (3). The Saudi Food and Drug Authority (SFDA) is an “institution that oversees all matters related to foods including food laws and regulations, information and education activities for the consumers” (1). Recently, the SFDA had issued a law that requires bakeries, restaurants, cafes, and ice cream parlors to provide their consumers with calorie information on written menus and monitors (4). It is an approach to promote a healthier lifestyle by reducing salt, sugar, and saturated and trans fats in products. Since 2007, the SFDA has been implementing mandatory prepackaged food labeling containing nutritional information such as calorie counts, carbohydrates, fats (saturated fat, trans fat), proteins, and other components, along with production and expiration dates (5).
Since nutrition has been recognized as an effective factor in order to control chronic diseases, nutritional awareness increased among the people which makes them learn how to choose healthy food. Labeling is defined as “any words, particulars, trademarks, brand names, pictorial matter or symbol relating to a food stuff and placed on any packaging, document, notice, ring or collar accompanying or referring to such food stuff” (6). It includes any statement provided about the food product, explanation or description, whether it is illustrated, written, printed, glued, engraved, or connected to the food package. The main purpose for this label is to provide basic information related to the product, health safety, and nutritional information, as well as to facilitate promotion. According to Anastasiou et al. (7), food companies should specify the quantities and types of fats, total fat, saturated fat, cholesterol, sodium, total carbohydrates, dietary fiber, sugar, protein, vitamin A and C, calcium and iron in one serving of the product.
Reading the food label has many benefits for consumers, such as identifying the food item, understanding the contents of the package, avoiding unwanted foods, choosing a taste they like, knowing the internal components of the food, identifying food additives and knowing the nutrition value. Because of its importance as one of the most powerful mediums to convey information from manufacturers to consumers, it should be detailed but simple, accurate and unbiased, and it should provide evidence-based health claims to assist consumers in their decision-making process by encouraging them to choose healthy foods (7). According to Kretser's (8) study, consumers are more likely to purchase healthy foods and beverages by utilizing information provided on food labels to achieve their health goals. Furthermore, choosing healthy food depends on other factors, including how information is perceived and understood. But this perception and understanding can be influenced by other factors such as nutrition knowledge (9), nutrition labeling content (10), and even socioeconomic factors (11). Regulatory measures on food labels alone would be insufficient if they were not accompanied by an assessment of consumers awareness regarding healthy choices and nutrition labels, and choosing a healthy diet depends on understanding and interpreting food labels (12). Drichoutis et al. (13) found that personality traits and behavioral and attitudinal factors influenced the use of food labels. A study carried out in India concluded that around 66 % of adolescents believe that nutrition details on food stuff labels are complex and are difficult to understand (14).
A previous study by Washi (15) revealed that most Saudi consumers were not familiar with the serving size, the nutritional content of the food product, and the health claims mentioned on the labels. Another study by Al-Barqi et al. (1) on students in health colleges reported that food label use was low among the participants. Research shows that nutrition knowledge promotes food label use, while time constraints pose a serious obstruction. To our knowledge, no study has been found that assessed the knowledge and awareness of the Saudi consumers in the Al-Ahsa Governorate in Saudi Arabia about the use of food labels. Therefore, the objective of this study was to assess Saudi consumers' knowledge, awareness, and practices in relation to food labels. The results may provide valuable information for the SFDA in order to evaluate the impact of their efforts, policies and regulations associated with food labeling on Saudi consumer's behaviors through its frequent and effective use.
MATERIALS AND METHODS
STUDY DESIGN AND PARTICIPANTS
A cross-sectional study was carried out on 403 consumers (males and females ≥ 18 years) in Al-Ahsa, Saudi Arabia. Random sampling was used to recruit Saudi consumers in Al-Ahsa. All consumers participating in the study provided their informed consent, after their roles and responsibilities in the study were explained clearly. All participants signed their consent forms on a voluntary basis and were informed that they are free to withdraw at any time.
INSTITUTIONAL REVIEW BOARD STATEMENT
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of King Saud University (Ref. No. KSU-HE-20-407).
INSTRUMENTS
Empirical data on Saudi consumers' knowledge, awareness, and practices related to food label were collected through a self-reported instrument. An electronic questionnaire containing 43 items was created to collect data. It consisted of six sections. The questions were adapted from previous studies (1,16,17).
Section 1
Participants' sociodemographic and health characteristics included gender, age, height (cm), weight (kg), marital status, educational level, and health status.
Section 2
The aim of this section was to assess participants' nutritional knowledge. This section contains one question to assess the participants nutrition knowledge (self-assessment) on a 5-point Likert scale (5 = very high knowledge, 4 = high knowledge, 3 = moderate knowledge, 2 = little knowledge, 1 = very little knowledge). Based on the mean scored, participants were classified as follow: 1-2.33, 2.34-2.67 and 2.68-5 were indicative of low, moderate and high knowledge, respectively. The questions were adapted from previous studies (1,17). The other questions in this section were multiple-choice questions with only one correct answer to assess the nutrition knowledge of participants (Nutrition knowledge scoring). A 10-point score was used to assess their reply of multiple-choice questions. Based on the points scored, participants were grouped as follow: scores of 0-3, 4-7, and 8-10 were indicative of low, moderate and high, respectively.
Section 3
This section aimed to evaluate participants' awareness of the food label. The questions were related to participants' awareness of reading and understanding the food label. Frequency categories were yes and no for reading and understanding the food label, and the willingness to buy the product in case of having no food label. Then, on a 3-point Likert scale (1 = little important, 2 = moderately important, 3 = very important), participants were requested to answer questions related to their attitudes towards the importance of food label. In case of having difficulties in understanding the food label, participants were requested to identify the reasons for this difficulty on a yes/no scale. Four reasons were identified for such difficulty: language differences, the small print size and font, limitation in understanding and other difficulty.
Section 4
This section identifies participants' opinions about food labels. On a 5-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree and 5 = strongly agree), participants were asked to answer the questions associated with their opinions about the significance of the food label to consumers and their health, food label's accuracy and honesty, as well as their keenness to buy the unhealthy products.
Section 5
This section aimed to measure the practices regarding food label by participants. The participants were requested to answer the questions associated with their practices regarding food labels in terms of using these labels, reading the production and expiration date, checking calorie, fats and sugar contents, checking and monitoring warning information, checking the product's price before purchasing and manufacturer's name, and reading storage conditions. All answers were made on a 5-point Likert scale (1 = never, 2 = rarely, 3 = often, 4 = frequently and 5 = always).
Section 6
This last section focused on some general areas regarding food label use. It contained questions related to barriers that hinder the use of labels and health worries if the participant does not read the food label. Options were provided and the participants were supposed to choose the best option.
STATISTICAL ANALYSIS
Data was analyzed using IBM SPSS statistics software version 21. Results were presented as percentage or mean ± standard deviation (SD). Pearson's correlation test was performed to estimate the correlation between the participants' knowledge, awareness and practices in relation to food labels. One-sample t test was used to test whether the sample mean is statistically different from a known or hypothesized population mean (= 3). Independent-samples t test and one-way ANOVA were performed to determine the difference of participants' knowledge, awareness and practices regarding food labels according to certain variables: sex, body mass index (BMI), age, educational level, marital status and health status. Statistical significance level was set at p-value ≤ 0.05.
RESULTS
SOCIODEMOGRAPHIC AND HEALTH CHARACTERISTICS OF PARTICIPANTS AND NUTRITION KNOWLEDGE ASSESSMENT AND SCORING OF THE PARTICIPANTS
The data obtained on sociodemographic and health characteristics of the participants (n = 403) is summarized in table I. The majority of participants (74.2 %) were female and 51.1 % were between 19 and 30 years old. About 59 % of the participants were married and 72 % of them held a university degree. The BMI of almost 50 % of them was normal while almost 47 % were either overweight or obese. The majority of participants (82.9 %) did not have any chronic diseases. The most common chronic disease reported by the participants was blood pressure, followed by diabetes.
Table I. Sociodemographic, health characteristics, nutrition knowledge assessment and scoring of the participants characteristics.
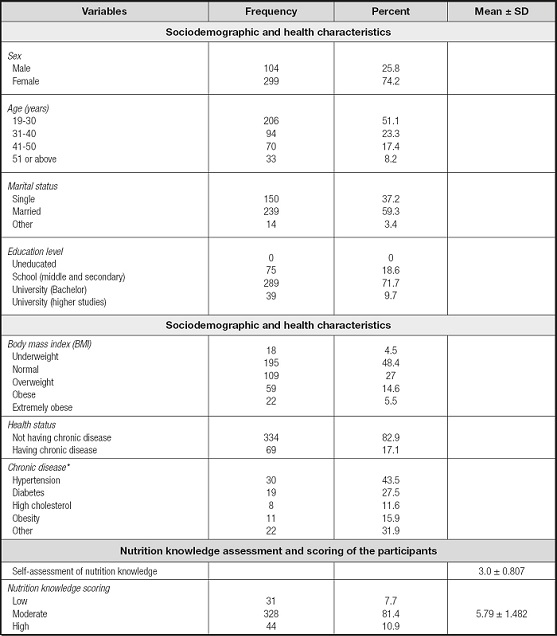
*Some participants may have two or more chronic diseases at the same time. Data has been represented as frequency and percentage or mean + standard deviation.
Participants' self-assessment of nutrition knowledge was at a moderate level (3.0 ± 0.807). The majority of participants (81.4 %) had moderate knowledge about general nutrition and the mean score (5.79 over 10) also indicated that participants' nutrition knowledge was at moderate level (Table I).
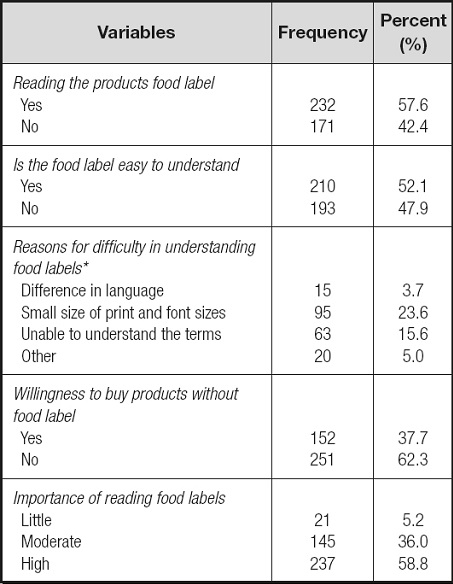
PARTICIPANTS' AWARENESS OF FOOD LABEL
According to our results, 57.6 % of participants read the products food label and 52.1 % confirmed that food label was easy to understand (Table II). On the other hand, some participants struggled in understanding these labels due to their small size and font of print (23.6 %). The majority of participants (62.3 %) do not like to buy products without food label. Around 58.8 % of participants indicate that it is very important to read the food label.
PARTICIPANTS' OPINION AND PRACTICES IN RELATION TO FOOD LABELS
Results showed that the opinions of participants about some aspects of food label were significantly high (p ≤ 0.01) in the score (mean = 4.13, SD = 0.587) (Table III). Participants strongly (p ≤ 0.01) believed that reading and understanding food labels is important and beneficial to the consumer (mean = 4.56, SD = 0.634) and it may prevent some diseases (mean = 4.5, SD = 0.67). In addition, participants believed that the nutritional warnings on food labels are honest (mean = 3.89, SD = 0.958), and the information mentioned on the food labels was accurate (mean = 3.57, SD = 0.996). All t values were significant (p ≤ 0.01), indicating that the means of the sample were significantly (p ≤ 0.01) different from the proposed value of three.
Table III. Participants' opinion and practices in relation to food labels.
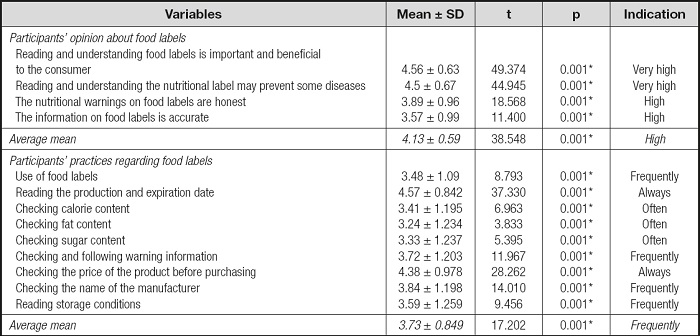
One-sample t test was used to test whether the sample mean is statistically different from a known or hypothesized population mean (= 3).
*Significant at p ≤ 0.01.
Results in table III revealed that participants practiced some of the food label uses on a “frequent” basis (mean = 3.73, SD = 0.849). Participants “always” read the production and expiration date (mean = 4.57, SD = 0.842) and checked the price of the product before purchasing (mean = 4.38, SD = 0.978). However, the results indicated some “frequently” practices regarding food labels such as checking the name of the manufacturer and warning information. Some practices fall into the category of “often”, such as checking calorie, sugar and fat contents. All t values were significant (p ≤ 0.01), indicating that the means of the sample were significantly (p ≤ 0.01) different from the proposed value of three.
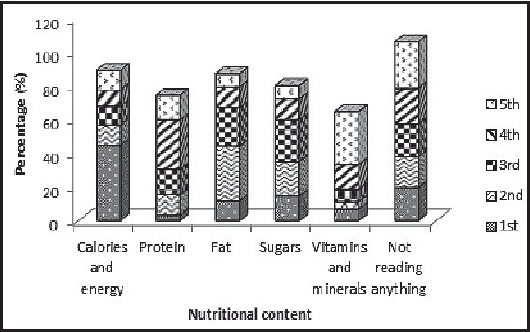
PARTICIPANTS' ORDERING OF FOOD LABEL'S INFORMATION
The study demonstrated that 44.4 % of participants read first the “calories and energy” contents and 31.3 % of them read the “vitamins and minerals” contents at the end (Fig. 1). The results showed a significant variation between participants selections in the order of the information checked while using the food label.
PARTICIPANTS' GENERAL AREAS OF INTEREST FOR FOOD LABEL USE
Results demonstrated that obesity (40.2 %) was the participant's main health worry in case they did not check the food label, followed by diabetes (25.1 %) (Fig. 2A), while high blood lipids (12.7 %), heart diseases (7.9 %) and hypertension (5 %) were the least common health worries. The investigation revealed that around 27 % of participants agreed that lack of time was the main barrier for not using food label information (Fig. 2B), followed by the difference in language (23.6 %). Among the 403 participants, only 2.7 % stated that food label has no use and 46.6 % of them stated that some other barriers are responsible for not using the food label information (Fig. 2B).
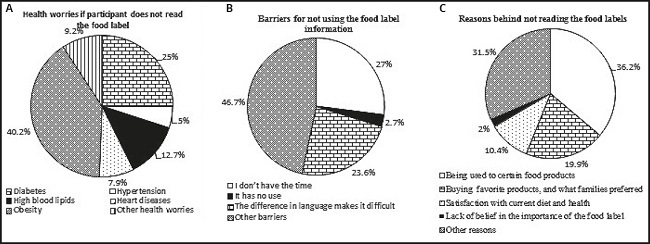
Figure 2. Participants' general areas of interest for food label use. Results have been expressed in percentages. A. Health worries if the participant does not read food labels. B. Barriers for not using food labels information. C. Reasons behind not reading food labels.
In addition, the reasons given by participants behind not reading the food labels (Fig. 2C) included buying certain food products they used to buy (36.2 %), buying favorite products, and buying what families preferred (19.9 %). On the other hand, 10.4 % of the participants claimed they are satisfied with their current diet and health, and only 2 % did not believe the food label is important.
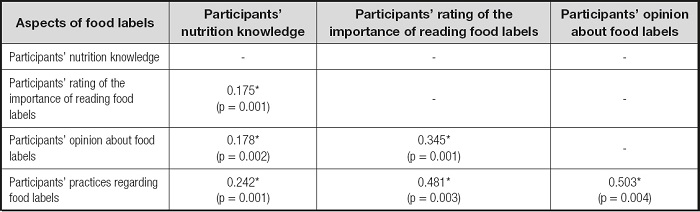
CORRELATIONS BETWEEN THE MAIN ASPECTS OF FOOD LABEL
Pearson correlations were calculated to investigate the associations between participants' nutrition knowledge, their rating of the importance of reading food labels, their opinions about food labels and their practices in relation to food labels (Table IV). A significant positive correlation (p ≤ 0.01) was found between participants' nutrition knowledge and their rating of the importance of reading the food labels (r = 0.175), their opinion about food labels (r = 0.178) and their practices in relation to food labels (r = 0.242). In addition, participants' rating of the importance of reading the food label was positively correlated with participants' opinion about food labels (r = 0.345) and participants' practices regarding food labels (r = 0.481). The correlation between participants' opinion about food labels and participants' practices regarding food labels was the strongest, with a Pearson correlation of 0.503.
PARTICIPANTS' DIFFERENCES IN THE MAIN ASPECTS OF FOOD LABEL BASED ON SEX AND HEALTH STATUS
Results in table V revealed a highly significant (p ≤ 0.01) difference between male and female participants in nutrition knowledge (t = -3.851, p = 0.000), rating of the importance of reading the food labels (t = -4.045, p = 0.001), opinions about food labels (t = -2.694, p = 0.007) and practices regarding food labels (t = -6.467, p = 0.000). Moreover, participants who have chronic diseases are more aware of practicing food labels than participants with non-chronic diseases (t = 3.926, p = 0.002). Other aspects of food labels were not affected by health status.
Table V. Participants' differences in the main aspects of food labels based on sex and health status.
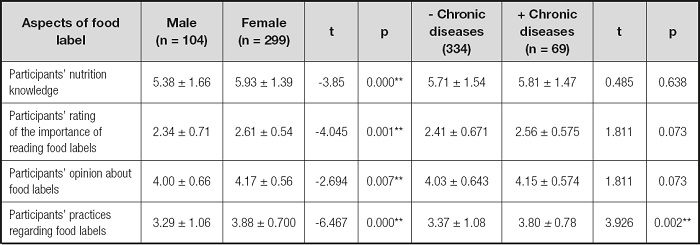
Independent-samples t test was used to investigate the difference of participants' knowledge, awareness and practices regarding food labels according to variables of sex and health status.
*Significant at p ≤ 0.5.
**Significant at p ≤ 0.01.
PARTICIPANT DIFFERENCES IN THE MAIN ASPECTS OF FOOD LABEL BASED ON AGE, BMI, MARITAL STATUS, AND EDUCATIONAL LEVEL
Our study indicated that the age of participants (Table VI) significantly affected their nutrition knowledge (F = 4.443, p = 0.004), their opinions about food labels (F = 2.596, p = 0.04) and their practices regarding food labels (F = 6.090, p = 0.000). All these significant (p ≤ 0.05/0.01) differences were on behalf of the age category (31-40) as indicated by the Scheffe test. However, participants' rating of the significance of reading the food labels was not affected by participants' age and participants BMI, and they have an insignificant effect on their nutrition knowledge, rating of the importance of reading food labels and their practices in relation to food labels. This variable only affected significantly (p ≤ 0.05) participants' opinion about food labels (F = 2.483, p = 0.043). This significant (p ≤ 0.05) difference was on behalf of the “underweight” category as indicated by the Scheffe test. Marital status has an insignificant effect on participants' nutrition knowledge, rating of the importance of reading food labels, opinions about food labels and practices in relation to food labels. However, results also indicated that the participants' educational level significantly (p ≤ 0.05/0.01) affected their nutrition knowledge (F = 2.721, p = 0.044), the rating of the importance of reading food labels (F = 3.627, p = 0.013), their opinions about food labels (F = 6.582, p = 0.000) and their practices regarding food labels (F = 7.800, p = 0.000). All these significant differences were on behalf of the “higher studies” category.
Table VI. Participant differences in the main aspects of food label according to age, BMI, marital status and educational level.
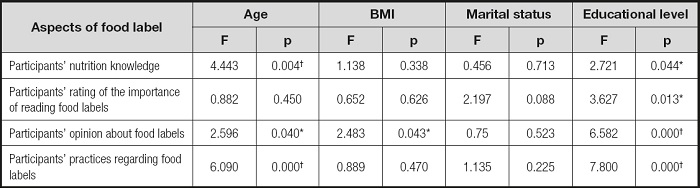
One-way ANOVA was used to investigate the difference of participants' knowledge, awareness and practices regarding food labels due to variables of age, body mass index (BMI), marital status, educational level and health status.
*Significant at p ≤ 0.05.
†Significant at p ≤ 0.01.
DISCUSSION
This study was aimed to evaluate Saudi consumers' knowledge, awareness, and practices as regards food labels, as well as to explore the effect of sociodemographic characteristics on various aspects of food labels. SFDA exerted extensive efforts in regulating the food labeling in Saudi Arabia, to enhance health awareness among Saudi consumers and to reduce nutrition-related diseases through healthier food choices. This study showed that most participants had moderate knowledge about general nutrition, which is in line with the results of a previous study carried out on Saudi female university students in Riyadh (1). The nutritional label provides information to customers about the available choices and inspires the consumption and production of healthy products. The result recorded around 57.6 % participants read the food labels. Other studies conducted in different parts of the world showed different percentages in reading food labels, for example, in China (28.7 %) (18), South Africa (70 %) (12) and US adolescents (9-16 %) (19). The Ministry of Health of Saudi Arabia has expended considerable effort in delivering public health programs and raising awareness about healthy diet, chronic disease prevention (obesity, diabetes) and the promotion of physical activity, which may be the reason for moderate knowledge about nutrition and reasonable use of food labels in the country (20,21).
Apart from this, positive and significant correlation between participants' nutrition knowledge and consumers' rating of the importance of reading the food label, their opinion about food labels and their practices in relation to food label has been found. Thus, it can be concluded that the knowledge of nutrition motivates the use of food labels. This finding is in agreement with previous studies (1,22). However, this study is contrary to the study performed on undergraduate student in Malaysia, by Nurliyana et al. (23). This inconsistency could be due to variants in the sample size, study time, ethnicity of the examined population, and participants characteristics. The cognitive processing model recommends that consumers with preceding knowledge tend towards using label information more efficiently than those without knowledge (24). So, in order to promote a positive attitude towards the nutrition label, it is immensely vital to upsurge consumers' awareness about health and the importance of nutrition to prevent diseases and promote health. Along with nutrition knowledge, consumers' attitudes toward other aspects related to food products such as taste and economic condition could also affect their use of food labels during the buying process.
It has been observed that participants with high ratings of the significance of reading food labels were more involved in having positive opinions/attitude and good practices regarding food labels. The results of this study showed that the majority of participants preferred to read the food products labels and they were not willing to buy the product without the label. Also, they were aware of the significance of food labels. It became a routine for Indian consumers to purchase prepackaged food after reading the label, so they were familiar with most of the products (25). Participants who find difficulties in understanding food labels mentioned that the causing agent behind this difficulty was the tiny size and font of print and shortage of time, as well as differences in language. This result obtained in the present study is in agreement with Al Barqi et al. (2020) (1) and Jacobs et al. (26). Moreover, Heidarinejad et al. (27) reported that the major causes for not paying attention to food labels include tiny printing of labels, ignorance, and lack of time, interest and motivation. Schupp et al. (28) reported that scarcity of time and interest and availability of previous information about food were the main reasons behind not paying attention to food labels among Americans. Another study revealed that dearth of knowledge and scarcity of interest in nutrition, along with lack of faith on information provided on the labels, small print size, checking the nutrition information only at first instance and scarcity of time were ranked in order of priority as reasons for lack of attention to food labels (29). Graham and Laska (30) reported that clear and colored fonts used on the nutrition label could be more appealing to consumers to read the nutrition label. Participants in the present study firmly believe that reading and understanding the food label is important for the consumer to avoid diseases. Additionally, participants strongly believe that food labels provide accurate nutrition information and the nutritional warnings were honest. These findings indicate that participants have positive attitudes toward using food labels, which in turns positively affects their practices regarding food labels. Al-Barqi's et al. (1) have confirmed similar findings where participants with positive attitudes toward food labels were more likely to use them compared with those with negative attitudes. Ng et al. (31) reported that attitude plays an important role on the customer's decision on food products and purchase. By educating the customer about the concept, importance, and application of food labels, it is possible to influence their desire to choose a healthier food product.
Mahgoub et al. (32) reported that half of the consumers worldwide understand only “partially” the nutritional label available on food packages. They found that lack of understanding was most prevalent among members of Asia Pacific (60 %), followed by Europeans (50 %) and Latin Americans (45 %), while North Americans, followed by Portugueses, Cannadians, and the consumers from New Zealand and Spain were most conversant with food labellings.
In the present study, manufacturing and expiration date, as well as the cost of the product, were read on a regular basis (always) before purchasing, while the manufacturing company name and warning information were frequently checked. Ganbari et al. (33) reported that maximum participants were more interested in production and expiration date of products, while fewer were concerned with the product's nutritional information and information related to additives. Similar findings have been reported earlier in other countries (27,34). A study carried out in Malawi stated that price was the foremost determinant factor to purchase (35). On the contrary, a study in Lesotho (32) showed that instead of price, nutrition information was the major element that influenced consumer's choice to purchase the product. On the other hand, food expiry dates on labels are easy to check and understand, which is very important to ensure food safety (36). Interestingly, calorie, sugar and fat contents were often checked, which reflects a little interest of participants toward these contents. Wahab (16) observed in his study on Bahraini customers that when buying food for the first time, fat content was the most commonly observed nutrient, followed by sugar and calories. The level of participants' nutrition knowledge, their opinions and the importance of checking food labels may affect their checking of nutrient contents such as calorie, sugar and fat contents. Thus, we can conclude that participants' practices in relation to food labels was positively correlated with these three variables.
However, other factors might affect some aspects of food label usage. Our results indicated that participants' sex affects their nutrition knowledge, rating of the importance of checking food labels, opinions about food labels and practices regarding food labels. Several studies agreed with this finding (16,32) and indicated that sex has a role in persuading food label use. In this study, the highest values recorded in females may be due to the chief role and responsibility of women in grocery shopping for household needs. But it could be also due to females being more concerned about their appearance and fitness than men, which makes them selective and in a mindset to prepare healthy meals (10,32). Nagya (37) reported that many males do not believe that nutritional information is valuable, or that it can help in food choices, or even think about to what extent health is important. By contrast, Aryee et al. (38) demonstrated that males were more likely to understand nutrition labels while other socio-demographic characteristics such as age, educational level, occupation and income were insignificant predictors. Simultaneously, they reported an insignificant connotation between the use of food labels, income and gender. Participants' age has an effect on their nutrition knowledge, opinions about food labels and practices when using food labels. This can be attributed to the restricted diets that their health advisers recommend to prevent them from developing chronic diseases at this age (13). However, BMI was found to have a significant effect on their opinion of food label. This indicates that BMI influences participants attitudes with little impact on their practices and other uses of food label.
Furthermore, results revealed that participants' educational level significantly affects their nutrition knowledge, the rating of the importance of reading food labels, their opinions about food label and their practices when using food labels on behalf of the “higher studies” category. Therefore, highly educated participants are more interested in some aspects of food labels than low educated ones. This is probably because educated consumers read academic journals and academic papers more regularly, so they have more exposure to health-related news and are aware of the connection between diet and health. This finding agrees with Mahgoub's et al. (32), who observed that educational levels have a role in the use of food labels. An educated person can interpret the nutritional information and incorporate it into a healthier diet. Researchers in the United Arab Emirates found a statistical correlation between consumer interest in reading and using food labels and levels of education (39).
The study recorded that most of the participants perceive obesity followed by diabetes, high blood lipid, heart disease and hypertension as the most significant health concerns related to not reading food labels. Similar results have been reported by Wahab (16) in the study carried out on consumers in Bahrain. In addition, results show that participants who have chronic diseases are more aware of checking food labels than participants who do not suffer from chronic diseases. This is a logical finding since individuals with chronic diseases are always at risk and trying to prevent some negative effects of foods contents such as salt, sugar, calories, etc. on their health. Choice the healthy food is acted by an individual to consume food with less sugar and fat and high content of fibers, fruits and vegetables. Nutrition plays a significant role in a healthier life. Since the public is trying to choose healthier food items, so, the health system and food department have a responsibility to provide the public with clear information about food. Finally, marital status has been found to have an insignificant effect on participants' nutrition knowledge, rating of the importance of reading food labels, opinions about food labels and practices in relation to food labels. Arfaoui et al. (40) reported that knowledge about nutrition facts labels and NHC is higher among participants without children and those shopping with their families because respondents have more time available to read food labels than parents and child-care giving parents shopping for household needs.
LIMITATIONS
This study used a valid questionnaire and a substantial sample size (n = 403), representative of the Saudi consumers in Al-Ahsa. However, due to this restriction (Saudi consumers in Al-Ahsa), the current study results cannot be generalized and may not reveal the reality of other Saudi population groups. Thus, further investigation including other Saudi population groups are needed to generalize these results. Moreover, it is crucial to emphasize the significance of nutrition knowledge to instill positive attitudes in Saudi consumers in Al-Ahsa to read the labels on their food products and practice this during purchase, which may reduce the occurrence of diet-related diseases in the Kingdom of Saudi Arabia.
CONCLUSIONS
This study assessed the knowledge, awareness, and practices regarding food labels during purchasing among Saudi consumers in Al-Ahsa. In Al-Ahsa, Saudi consumers' positive attitudes and practices toward food labels, and their emphasis on reading them seem to be influenced by nutrition knowledge, while shortage of time and language differences posed significant barriers. Hence, emphasis on increasing knowledge, awareness, and practices regarding food labels during purchasing among Saudi consumers in Al-Ahsa is required to meet the desired outcomes of the SFDA's policies and regulations. In order to prevent the phenomenon of random food shopping, it is suggested that the SFDA and other Saudi stakeholders develop a policy which should emphasize predetermined health food needs. Also, it needs to be publicized in every setting of the Saudi community (e.g., schools, universities, etc.). Schools and universities curricula should have nutrition basics, as nutrition knowledge has an impact on some food label aspects. Television, radio and internet programs can significantly improve consumers' knowledge, awareness and practices regarding food labels during purchasing. As such, consumers will learn more about food labels, which will lead to healthier dietary options. And consequently, this will reduce the deterioration in public health, morbidity and the occurrence of multiple diseases.
In contrast, more attention should be paid to barriers such as the difference in languages, print size, and the font used on food labels. So, the goal should be to ensure food labels are easier for consumers to read and comprehend.

