










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.109 no.1 Madrid ene. 2017
https://dx.doi.org/10.17235/reed.2016.4393/2016
LETTERS TO THE EDITOR
Anisakiasis and intestinal endometriosis: under-recognized conditions in the differential diagnosis of acute abdomen
Anisakiasis y endometriosis intestinal, entidades infravaloradas en el diagnóstico diferencial de abdomen agudo
Key words: Intestinal anisakiasis. Intestinal endometriosis. Intestinal perforation. Intestinal obstruction. Acute abdomen.
Palabras clave: Anisakiasis intestinal. Endometriosis intestinal. Perforación intestinal. Obstrucción intestinal. Abdomen agudo.
Dear Editor,
We report the case of a 39-year-old woman who presented at the Emergency Room with intestinal sub-occlusion.
Physical exploration found tenderness in right iliac fossa (RIF), distension, and tympanism. Lab tests revealed elevated C-reactive protein (CRP) levels in the absence of leukocytosis.
She had a similar episode two months before, with uncertain ileal biopsy results (inflammatory bowel disease [IBD] vs infectious ileitis). Computerized tomography (CT) showed ileal wall thickening with dilated loops, associated with stenosis at 7 cm from the ileocecal valve, which led to a differential diagnosis between ileitis and IBD (Fig. 1).

Following conservative management failure an urgent laparoscopy was performed, which found free-flowing fecaloid fluid and ileal perforation. Ileocecal resection via laparotomy was performed.
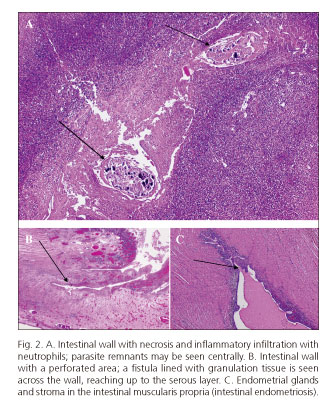
Pathology revealed a whitish lesion, 1.0 x 0.5 cm in size, with anisakid remnants and ileal endometriosis (Fig. 2). The definitive diagnosis was intestinal endometriosis and anisakiasis with ileal perforation.
Discussion
The pathogenesis of anisakis develops in two ways: allergic disease and direct damage to the organ wall (1).
Anisakiasis usually involves the stomach and intestinal damage is rare, hence definitive diagnosis is challenging and typically occurs after surgery for complications (2).
Treatment includes the endoscopic removal of larvae (for gastric involvement) or surgery when intestinal complications develop (3).
Endometriosis is a condition that affects up to 15% of fertile women. Intestinal involvement ranges from 3% to 37%. Small bowel involvement occurs less frequently, in 5-7% of cases (4), and diagnosis is challenging due to the location, as the condition mimics a number of bowel diseases, including IBD.
We highlight the relevance of the present case because of its challenging differential diagnosis. It was initially thought to be IBD; however, after the procedure and the subsequent pathology analysis, endometriosis and anisakiasis were diagnosed.
Carlos Sánchez-Justicia1, Lucía Granero-Peiró1 and Jorge Ali Árabe-Paredes2
1Departaments of General and Digestive Surgery, and
2Anatomic Pathology. Clínica Universidad de Navarra. Pamplona, Spain
References
1. López-Serrano MC, Gómez AA, Daschner A, et al. Gastroallergic anisakiasis: Findings in 22 patients. J Gastroenterol Hepatol 2000;15(5):503-6. DOI: 10.1046/j.1440-1746.2000.02153.x. [ Links ]
2. Sasaki T, Fukumori D, Matsumoto H, et al. Small bowel obstruction caused by anisakis of the small intestine: Report of a case. Surg Today 2003;33:123-5. DOI: 10.1007/s005950300027. [ Links ]
3. Olveira A, Sánchez Rancano S, Conde Gacho P, et al. Gastrointestinal anisakiasis. Seven cases in three months. Rev Esp Enferm Dig 1999;91(1):70-2. [ Links ]
4. MaCafee CH, Greer HL. Intestinal endometriosis. A report of 29 cases and a survey of the literature. J Obstet Gynecol Br Emp 1960;67:539-55. DOI: 10.1111/j.1471-0528.1960.tb09211.x. [ Links ]
