










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Small bowel capsule endoscopy (SBCE) is no longer an emerging diagnostic tool but rather part of routine clinical practice, with clearly defined indications 1. It was first approved in 2001 and since then several technical improvements have been made. PillCam(r) SB3 has a greater image resolution and adaptive frame rate technology compared with previous versions, which increases the frame rate from two frames/second to six frames/second when the capsule is moving faster.
Some studies found a greater diagnostic yield using SB3 (44% vs 62%, p < 0.05) and even recommend a repeat SBCE using SB3 in cases when SB2 was inconclusive 2. However, previous studies have reported that the SB2-extended 3 battery had a lower diagnostic yield (48.5% for SB2 vs 35% for SB2-ex, p = 0.01) compared to SB2. Thus, suggesting that not all technical improvements have provided a diagnostic advantage.
Bearing this in mind, this study compared the completion rate, findings and diagnostic yield of SB2 and SB3 considering not only the global examination but also tertile assessment in order to determine whether technological upgrades can overcome the identified pitfalls of this diagnostic tool.
METHODS
This was a retrospective study in the Gastroenterology Department of a university affiliated hospital that is highly experienced in SBCE. All videos of 357 consecutive SBCE, 173 SB2 and 184 SB3, which were performed between September 2012 and August 2015 were reviewed.
SBCE was performed with the PillCam(r) SB2 or SB3 (the former was substituted by the latter when it became commercially available) using the standard protocol within our center. The protocol was as follows: a clear liquid diet the day before the procedure and a 12h night-fast, patients were given 100 mg of Simethicone 30 minutes before capsule ingestion and 1h after ingestion they returned to our center for real time visualization. If the capsule remained in the stomach at this point, the patient was given 10 mg of oral domperidone. If the capsule remained in the stomach after pro kinetic administration, it was passed into the duodenum by upper gastrointestinal endoscopy 4) (5.
The complete video obtained during each SBCE procedure was reviewed by one experienced gastroenterologist (over 150 examinations). Videos were reviewed using the Rapid(r) Software at 8-12 frames per second rate; the FICE technology was also used when necessary 6) (7.
Data with regard to age, gender, capsule type (PillCam(r) SB2 or SB3), capsule indication, quality of bowel preparation, completion of the examination, gastric and small bowel transit time and the presence of findings in segments other than the small bowel were collected. The preparation was considered to be acceptable or adequate if > 50% or > 75%, respectively, of the mucosa was in a perfect cleansing condition 5. The reported findings in the small bowel were: active bleeding, angiectasia, varices, erosions, ulcers, stenosis, polyps/masses, diverticula, villous edema and villous atrophy. Both physicians were required to declare the relevance of the findings in the clinical setting. With regard to patients undergoing SBCE due to a suspicion/staging of inflammatory bowel disease, erosions, ulcers, stenosis and villous edema were considered as relevant. With regard to patients undergoing SBCE due to obscure gastrointestinal bleeding, active bleeding, angiectasia, varices, erosions, ulcers, polyps/masses and villous atrophy were considered as relevant. For patients undergoing SBCE due to unresponsive celiac disease, villous atrophy, ulcers and polyps/masses were considered as relevant. For patients undergoing SBCE for polyposis syndrome, polyps or masses were considered as relevant.
The presence/absence of findings in each tertile was also reported and for each examination and the detection of specific anatomical markers such as the Z line and papilla were also reported. The Lewis Score (LS) was calculated for patients with inflammatory lesions, who were categorized into three groups according to the defined and validated cut-off: non-significant inflammation if LS < 135, mild inflammation if LS 135-790 and moderate to severe inflammation if LS ≥ 790 8.
Statistical analysis was performed using SPSS v.21.0 and a two-tailed p value < 0.05 was considered as statistically significant. Categorical variables were presented as frequencies and percentages and compared using the Fisher's exact test or Chi-squared test as appropriate. Continuous variables were presented as means and standard deviations and compared using the Student's t test. A subgroup analysis of patients with suspicion/staging of IBD and patients with OGIB was also performed.
All patients signed an informed consent form and consensual contraindications for the SBCE procedure were respected as described elsewhere 9.
RESULTS
In this study, 357 SBCE, 173 SB2 and 184 SB3, were performed. The most frequent indications were suspicion/staging of inflammatory bowel disease (IBD) and obscure gastrointestinal bleeding (OGIB), (43.7% and 40.3%, respectively). The mean age of the patients was 47.7 ± 19.2 years and 66.9% were female. The median small-bowel transit time (SBTT) was 276.2 ± 107.6 minutes and the overall completion rate was 95% (339/357). With regard to bowel preparation, this was considered to be adequate in 62.7%, acceptable in 32.8% and poor in 4.5% of cases.
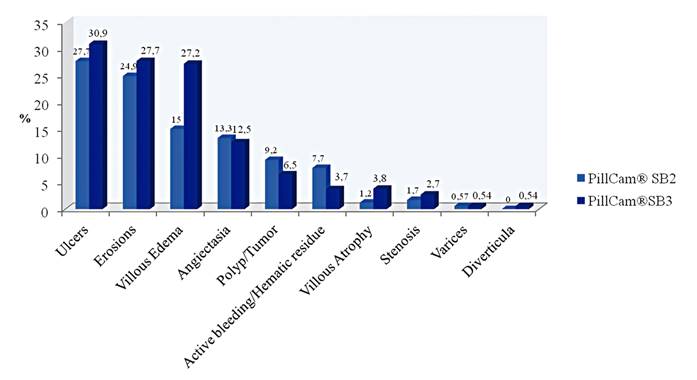
Endoscopic findings were reported in 76.2% (272/357) of the examinations and relevant findings were present in 53.5% (191/357) of procedures. The most frequently reported finding in the small bowel (SB) were ulcers and erosions in 29.4% and 26.3% of patients, respectively (Fig. 1). With regard to tertile findings, 46.5% of patients had findings in the first tertile, 30.3% in the second and 42% in the third. Findings in gastrointestinal segments other than the SB were reported in 20.4% of SBCE and these were most frequently in the stomach (16.8%) and less frequently in the esophagus and colon (0.3% and 3.4%, respectively).

There were no significant differences with regard to age (47.5 ± 20.2 vs 47.8 ± 18.3 years, p = 0.89) and gender (females in 65.9% vs 67.9%, p = 0.68) in patients that underwent SB2 and SB3 PillCam(r). No significant differences were found between SB2 and SB3 with regard to completion rate (93.6% vs 96.2%, p = 0.27), overall endoscopic findings (73.4% vs 78.8%, p = 0.23), relevant findings (54.3% vs 52.7%, p = 0.76), first, second and third tertile findings (43.9% vs 48.9%, p = 0.35; 31.2% vs 29.3%, p = 0.70; 37.6% vs 46.2%, p = 0.99), extra-SB findings (23.7% vs 17.4%, p = 0.14) and the Z line and papilla detection rate (35.9% vs 35.7%, p = 0.97 and 27.2% vs 32.6%, p = 0.26, respectively). With regard to specific findings, SB3 detected a greater proportion of villous edema (15.0% vs 27.7%, p = 0.005) but no differences were found between the two capsules for the detection of other findings (Fig. 2).
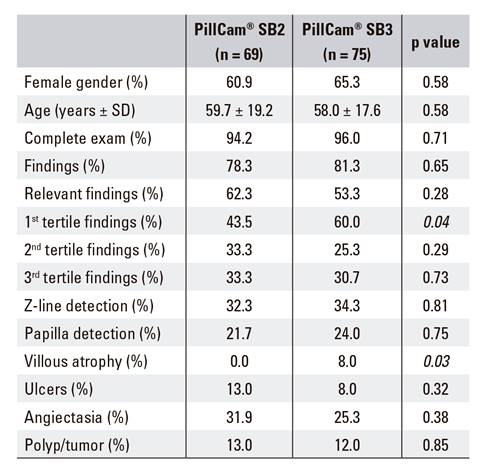
There were no significant differences in the subgroup analysis of patients with a suspicion/staging of IBD for the detection of villous edema and third tertile findings, thus favoring SB3 (26.3% vs 43.8%, p = 0.02 and 47.4% vs 66.3%, p = 0.02, respectively). No differences were found with regard to the detection of ulcers and stenosis (46.1% vs 55.0%, p = 0.26 and 2.6% vs 3.8%, p = 0.38, respectively) or the Lewis score classification (LS > 135 in 52.0% vs 63.9%, p = 0.15). No differences were found between the two groups with regard to other specific findings (Table 1).

A subgroup analysis of patients with OGIB, including both obscure and manifested, showed that villous atrophy was significantly more frequently reported with the PillCam(r) SB3 (0% vs 8%, p = 0.03) and first tertile findings were also significantly more frequently reported with the latest PillCam(r) version (43.5% vs 60.0%, p = 0.047). No differences were found between the two groups regarding other specific findings (Table 2).
DISCUSSION
SBCE is currently a widely accepted diagnostic tool with an increasingly recognized value for the study of small bowel pathology. Technological improvement of this technique is expected to overcome the limitations and provide an even better diagnostic accuracy. However, few studies have been published regarding the diagnostic performance of SB3 and, to our knowledge, this is the largest series comparing PillCam(r) SB2 and SB3.
The technical improvement may render capsule endoscopy more efficient for several reasons. First, since some small bowel diseases may present with villi alterations such as edema, distortion and atrophy, a greater image resolution may allow an increased detection frequency. Secondly, several studies have reported that the SBCE diagnostic yield is related with SBTT, with a positive correlation between the diagnostic yield and SBTT. Thus, suggesting that the longer the SBTT, the higher the diagnostic yield 10),(11. In fact, one of the main concerns regarding the SBCE diagnostic yield (DY) is related with proximal small bowel lesion detection. This segment has a faster transit time and therefore, SBCE has a higher rate of missed lesions within this segment 12) (13. Since SB3 has an adaptive frame rate according to capsule velocity, this limitation could theoretically be surpassed. Considering that the major duodenal papilla is present in all individuals who have not undergone surgery and is located in the proximal small bowel, its detection may be used as an indirect marker of a possible missed lesion in the proximal small bowel during capsule endoscopy studies. Previous reports indicate that the papilla is observed in under half of SBCE procedures 14. Therefore, theoretically, a greater papilla detection rate could be used as a surrogate for a better visualization of the proximal small bowel.
In our cohort, no statistically significant differences in the completion rate between the two capsules were found and both techniques had over 93% of complete examinations. This high completion rate is probably attributable to the small bowel capsule protocol applied in our center, in which real time view and, if needed, prokinetics are used to accelerate the capsule entrance into the small bowel, without interfering with the SBTT 4.
It was also verified that there were no statistically significant differences in the detection of small bowel lesions between the two capsules with regard to global findings, diagnostic yield, specific findings or tertile findings. These results are in contrast to the previously reported findings by Dunn et al. 2. This study found PillCam(r) SB3 to have a greater diagnostic yield than SB2 (44% vs 62%, p < 0.05) and even recommended a repeat capsule enteroscopy in cases for which SB2 capsule was equivocal.
As described above, the papilla can be used as a surrogate for missed lesions within the proximal small bowel and a higher detection rate could imply that PillCam(r) SB3 with an adaptable frame rate provides a better visualization of the proximal small bowel. In the current study, even though the papilla was detected in a higher percentage of PillCam SB3(r) studies, this difference did not reach statistical significance (27.2% vs 32.6%, p = 0.26). This finding is in agreement with the study of Dunn et al. 2, who also found no statistically significant differences in the detection of the papilla using SB2 and SB3 (14% vs 18%, p > 0.05). Selby et al. evaluated the papilla detection rate using several capsules, not only with different frame rates but also with different fields of view and even different numbers of capturing heads (PillCam(r) SB1, SB2, ESO1 and ESO2). This study found that all the capsules had a suboptimal detection of the papilla (0%, 18%, 0% and 8%, respectively), particularly those with narrower fields of view 15.
In our cohort, PillCam SB3 had a significantly higher detection rate of villous edema for all the examinations and also when considering only patients with a suspicion/staging of IBD. Villous edema is a particularly important finding in this setting, since its characteristics and distribution are part of a validated inflammation score, the Lewis score 16. This is available in the PillCam(r) capsule reading software (RAPID(r)). This score takes into account villous edema, ulcers and stenosis, considering their extent and severity in the different SB tertiles. However, despite the higher detection rate of villous edema, no significant differences were found with regard to the Lewis score between SB2 and SB3 in this subset of patients. This could mean that the higher detection rate of these villi alterations does not translate into a greater capacity to obtain a more accurate diagnosis, nor to provide more precise stratification of the inflammatory activity.
In addition, when considering patients undergoing SBCE in the setting of OGIB (both obscure and overt), a greater detection rate of villous atrophy was observed. Interestingly, studies performed with celiac disease cases showed that capsule endoscopy had a greater diagnostic accuracy than conventional upper endoscopy for the detection of villous atrophy, with a moderate concordance with histology 17. This outperformance of capsule endoscopy over conventional endoscopy is probably due to a greater image magnification. Therefore, we hypothesize that, in our cohort, the higher villous atrophy detection precision provided by PillCam SB3 is related to the increased image resolution.
In conclusion, the PillCam(r) SB3 did not improve the overall diagnostic yield nor the completion rate compared to SB2. Nevertheless, when particular indications were analyzed, significant differences with regard to the detection of villi alteration such as atrophy and segmental villous edema were found, which may be attributable to the better image resolution of SB3.
