










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Stroke is defined as a rapidly developed clinical signs of focal disturbance of cerebral function, lasting more than 24 hours (or) leading to death with no apparent cause other than that of vascular origin [1]. Stroke is one of the third leading causes of death. It makes an important contribution to morbidity, mortality and disability in developed as well as developing countries [2]. Although the prevalence of stroke appears to be comparatively less in India than in developed countries, it is likely to increase proportionally with the increase in life expectancy [3]. The proportion of strokes in the young is significantly more in India than in developed countries [13]. Recent survey estimates that stroke mortality rate in India is 7 people suffering in 1 lakh population affected in stroke [4]. Stroke is an acute severe manifestation of cerebro-vascular disease [14]. Into the cerebro-vascular diseases, stroke is one of the most acute severe manifestations. The disturbance of cerebral function is caused by 3 morphological abnormalities: stenosis, occlusion or rupture of the arteries [15]. Dysfunction of the brain (neurological deficit) manifests itself by various neurological signs and symptoms that are related to the extent of lesion area involved [5]. The clinical manifestations include coma, hemiplegia, monoplegia, speech disturbances, cranial nerve paresis, etc [6].
A variety of mechanisms can account the possible improvements that follow cerebral injuries [7]:
TYPES OF STROKE
Types of ischemic stroke: The most common type of stroke accounting for almost 80% of all strokes is caused by a clot or other blockage within an artery leading to the brain. It can further be divided into two main types [8]: Thrombotic and embolic.
Hemorrhagic stroke: Intracerebral hemorrhage is less common than cerebral ischemia, but has a worse prognosis. It occurs when a diseased blood vessel within the brain bursts, allowing blood to leak inside the brain [9]. The sudden increase in pressure within the brain can cause damage to the brain cells surrounding the blood. If the amount of blood increases rapidly, the sudden build up in pressure can lead to unconsciousness or death. Intracerebral hemorrhage usually occurs in selected parts of the brain including the basal ganglia, cerebellum, brainstem or cortex [10].
Bobath considered abnormal co-ordination of movement patterns and abnormal tone to be the main problems in hemiplegia. Bobath's concept believes that abnormal tone which can be lower or higher than normal influences the patient's movement patterns adversely [11]. The Bobath concept uses techniques aimed at the normalization of muscle and postural tone, facilitation of more normal movement patterns in the trunk, pelvis and limbs, and facilitation of the act of walking.
In my study I have chosen, Bobath Intervention and Functional Task Intervention as treatment technique for stroke patients and Timed Up and Go Test as a parameter to determine the efficiency of techniques.
Objective of the study
To compare the effectiveness of Functional task intervention and Bobath intervention on patients with impaired gait function in stroke patients with Timed and go test.
MATERIAL AND METHODS
MATERIALS
Arm rest Chairs.
Stop watch.
Balance beam.
Tape.
Tape measure.
Marking tools.
Timed up and go chart.
Knee gaiter & Ankle Foot Orthosis.
METHODOLOGY
Study Design: Experimental -comparative study.
Study settings: Physiotherapy center, NIMHANS, Bangalore, Karnataka, India
Study Sampling: A total of 10 patients selected by simple purposive random sampling methods after giving due consideration to inclusion/exclusion criteria were equally divided into two groups as A and B.
Study Duration: 8 weeks.
-
Inclusion criteria:
-
Exclusion criteria:
PARAMETERS
Timed up and go test (Figure 1):
This is a stroke assessment instrument organized into seven continuous tasks given for the subjects.
Patient position: The subject is asked to sit correctly in a chair with arms; the subject's back should rest on the back of the chair. The chair should be stable and positioned such that it will not move when the subject moves from sitting to standing.
Task position: Place a piece of tape or other marker on the floor 3 meters away from the chair so that it is easily seen by the subject.
Task Procedure: The patients are instructed in the word “Go” you will stand up, walk about three meters come back to the chair and sit down, they must walk in normal pace for about six meters. Go and Stop instruction is given at starting and end of the assessment.

Treatment technique: Functional task intervention (Figure 2):
In the functional task intervention the subjects are properly instructed about the task and instructed to perform each task five minutes and given interval of five minutes between tasks.
Standing up and walk Patient Position: Patient seated in an arm rest chair in front of the therapist.
Task Position: In the treatment room there are four standard armchairs placed at four corners.
Task procedure: Five minutes of repeatedly standing up and walking to the chair directly in the front, sitting then standing up and walking to the chair on the left.
Progression: From using the chair with arms can be replaced with armless chairs.
Step-ups Patient position: The patient is asked to stand in front of the steps in the treatment room.
-
Task procedure:
-
Treatment duration:

Bobath Intervention (Figure 3):
The patients were much more concentrated in gait specific activities. They include working on different phase of gait or walking with the assistance of therapist. Proper instructions were given to the patients. The intervention includes phases: Stance phase re-education and swing phase re-education.
Stance phase re-education: The treatment procedure is to gain balance while walking and to train walking. They include stepping with unaffected lower limb forward, stepping with the unaffected lower limb backward and stepping the unaffected lower limb sideways.
Swing phase re-education: The treatment procedure is to train the subject in walking and to help in proper placement of foot they include stepping with the affected lower limb and walking practice.
-
Treatment duration:

RESULTS
Table 1 shows the comparative mean value, means difference, standard deviation and Paired t-value between Pre versus post-test of group A (Functional task intervention). Figure 4 represents the data.
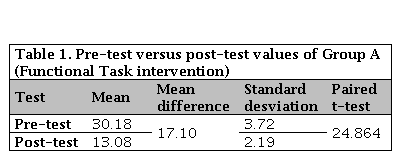
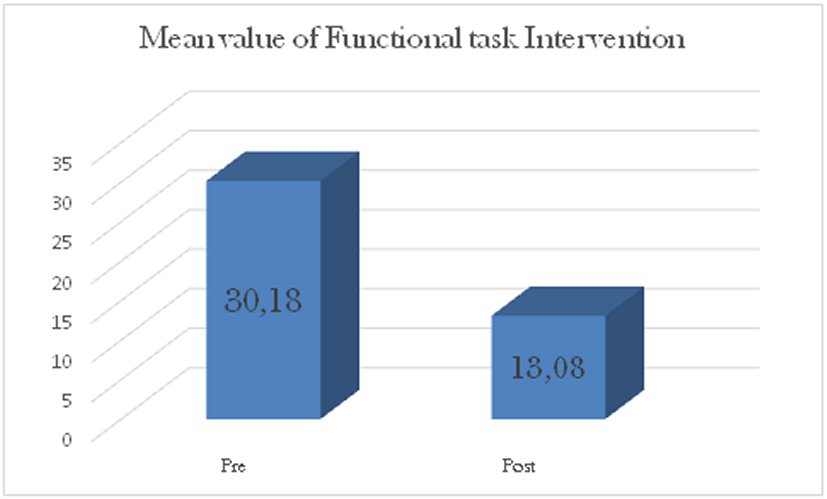
It explains, the paired t value of 24.864 is greater than the tabulated t value2.78, which showed that there is statistical significant difference at 0.05 levels between pre versus post-test results. The pre-test mean is 30.18 and the post- test mean is 13.08 and their mean difference is 17.10, which is shown in the values of timed up and go test in response to functional task intervention after 6 weeks of treatment.
Table 2 shows the comparative mean value, means difference, standard deviation and paired t-test value between pre-test versus post-test of Group B (Bobath intervention). Figure 5 represents the data.


It explains, the paired t-value of 29.71 is greater than tabulated t-value 2.78, which showed that there is statistical significant difference at 0.05 levels between pre versus post-test results. The pre-test mean is 31.48 and the post test mean is 18.04 and the mean difference is 13.44, which is shown increase in the values of Timed up and go test in response to Bobath intervention after 6 weeks.
Table 3 shows the comparative mean value, mean difference, standard deviation and unpaired t-test value of group A and Group B. Figure 6 represents the data.
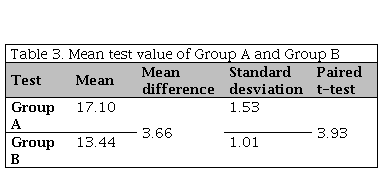
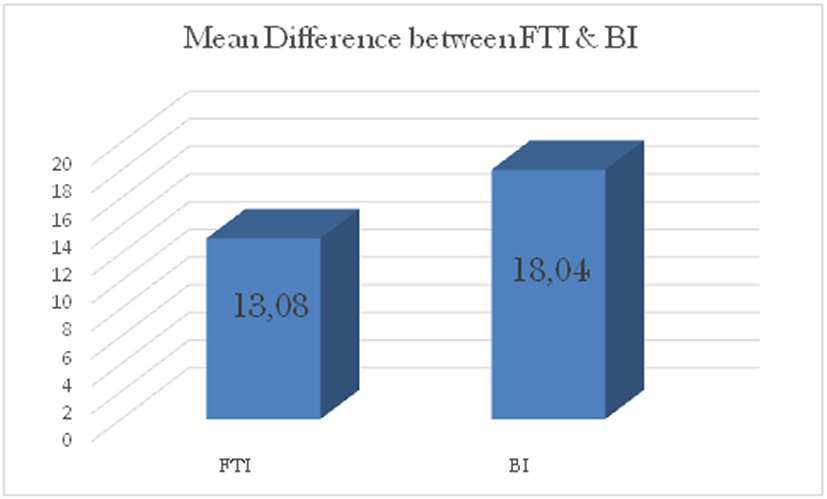
Figure 6. Mean value of timed up and go test between Group A and Group B.FTI: Functional task intervention; BI: Bobath intervention.
It explains, the unpaired t-test value of 3.93 is greater than tabulated value 2.31, which shown that there is significantly difference at 0.05 level between mean difference Group A and Group B. the pre-test versus post-test mean of Group A=17.10, the pre-test versus post-test mean of group B =13.44 and the mean difference of Group A and Group B=3.66, which has shown in timed up and go test in response to treatment of Group A when compare to Group B.
DISCUSSION
The aim of the study was to compare the effectiveness of Functional task intervention and Bobath intervention as Treatment of stroke patients with Timed up and go test as a parameter.
Conducted a study to examine the reliability of Timed up and go test in 10 healthy subjects and 11 subjects with chronic stroke treated with task related training. The timed up and go test showed excellent reliability (ICC>.95). The results from the study concluded that Timed up and go test is reliable measure for assessing the impairment in a population of patients undergoing rehabilitation following stroke [12].
The paired t-test 24.864 was greater than the tabulated t-value 2.78 at0.05 level of confidence, which showed that there was a statistically significant difference between pre-test and post-test with Timed up and go test. The pre- test mean was 30.18 and the post-test mean was 13.08. The mean difference between pre-test versus post-test was 17.10 which showed that there was increase in Timed up and go test that results in improvement of Group A patients.
The paired t-test 29.71 is greater than the tabulated t-value 2.78 at 0.05 level of confidence, which showed that there was a statistically significant difference in Timed up and goes test between pre-test and post-test. The pre-test mean was 31.48 and the post-test mean was 18.04. The mean difference between pre-test versus post-test was 13.44 which showed that there was a increase in Timed up and go test that results in improvement of Group B patients.
Avoid hyphenation at the end of a line. Symbols denoting vectors and matrices should be indicated in bold type. Scalar variable names should normally be expressed using italics. Weights and measures should be expressed in SI units. All non-standard abbreviations or symbols must be defined when first mentioned, or a glossary provided.
The unpaired t-test value 3.93 was greater than the tabulated t-value 2.31 at 0.05 level of confidence, which showed that there was a statistically difference between pre-test versus post-test results of Group A and Group B. The mean value of Group A 17.10, Group B 13.44 and the mean difference was 3.66 which showed that there was significant increase in Timed up and go test and its improvement in conditions of patients in Group A when compared to Group B in response to treatment.
CONCLUSION
The study concluded that Functional task intervention and Bobath intervention has beneficial effect on stroke patients based on Timed up and go test. The result of the comparative study concluded that the Functional task intervention with unilateral knee gaiter along ankle foot orthosis was effective treatment than Bobath intervention for the therapeutic management of affected stroke subjects.
Future recommendations: The future Study with long term follows up along with large sample size need to be further evaluated. The Dominant and non-dominant involvement could be analyzed separately. The evaluation criteria for the selection of the sample should be relaxed for further generalization and other parameters can be used to assess upper limb function.

