










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
The coronavirus disease (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Esakandari et al., 2020), which induced the start of a viral pandemic on December 31st, 2019, in Wuhan, China (Lechien et al., 2020). A few months after the first case, cases began to be identified in other Asian countries, Iran and European countries such as Italy, Spain, France, Germany and the United Kingdom (Mullol et al., 2020). As of early August 2020, the COVID-19 disease had already affected 188 countries around the world (Mullol et al., 2020). In Spain, the first case was detected on February 2nd, 2020, reaching 2,705,001 confirmed cases and 50,806 deaths on January 30th, 2021.
The exponential increase in infection worldwide, and its severity, led the World Health Organisation (WHO) to recognize the COVID-19 outbreak as a global pandemic on March 11th, 2020. For this reason, on March 14th, the Spanish government declared a nationwide state of alert and, two days later, a formal lockdown was imposed (Royal Decree 463/2020, March 14th). Nursery, primary and secondary schools, colleges and universities had already started to close between the 9th and 13th of March, although they remained active on an online basis. Due to the established lockdown, only companies performing an 'essential service' continued their normal activity. The Spanish population was confined to their homes, being allowed to go out only to buy food, provide care for dependent people, work and walk the dog (Gismero-González et al., 2020).
On April 25th, a slow and progressive lifting of the restrictions started with letting children out for one hour a day (Orden SND/370/2020, April 25th). A week after this, a four-phase process of unlocking started (Pérez et al., 2021). In phase 0, people could go out to practise individual sports, stores could offer services by making previous appointments, and restaurants could open for takeaway. People could also take a daily walk accompanied, at most, by a partner and always within a radius of one kilometer from their homes. The walks and sports practices had a time limit. In phase 1, restaurants with an outdoor area could open partially, and little shops and hotels could also open, but were not allowed to use the common areas. Religious and sports activities were also allowed, although with restrictions. In phase 2, indoor restaurants and spaces that offer cultural activities could open with capacity restrictions. Nursery and further education (only for students preparing for university) opened their doors. In phase 3, mobility from communities was allowed, although store capacity restrictions were maintained. Thereafter, the “new normality” started, although keeping hygiene and social distance measures.
The lockdown is understood as a massive restrictive quarantine (Pandey et al., 2020). This has been imposed years ago on specific occasions to fight other viral outbreaks, such as the severe acute respiratory syndrome (SARS) in certain areas of Canada and China in 2003, and the Ebola outbreak that took place in West African villages in 2014 (Hernández-López et al., 2021; Pandey et al., 2020). It is already known that this quarantine entailed a difficult situation to cope with, which implies separation from loved ones, loss of freedom, and insecurity in the face of the possibility of being infected, as well as boredom. In turn, this can cause negative effects on people (Gismero-González et al., 2020).
However, the COVID-19 lockdown we have experienced appears to be the most extensive and restrictive quarantine to date (Pandey et al., 2020). The measures imposed have significantly changed people's daily lives and led to a disruption of self-regulated behaviour and a reduction in social connections, resulting in specific mental health problems, especially in vulnerable people, such as people with mental disorders (Benke et al., 2020). Alterations in psychological well-being such as anxiety, depression, irritability, inattention, mood changes, sleep disorders, fears, family violence and suicide attempts have been observed in different population groups during and after the lockdown, even reporting an increase in these symptoms as it lengthened over time (Every-Palmer et al., 2020; Panda et al., 2021; Planchuelo-Gómez et al., 2020; Scarpelli et al., 2021).
This impact of confinement on people's mental health during lockdown was uneven in different population groups, finding that young adults between 19 and 30 years old showed higher levels of anxiety, stress, hopelessness, depression and sleep problems than older people (Planchuelo-Gómez et al., 2020). In turn, the impact on psychological well-being was more prevalent in women than in men (Passavanti et al., 2021; Ren et al., 2021). That is why being a young person, woman, and having a previous illness or preschool children were considered risk factors for suffering alterations in mental health during confinement (Horesh et al., 2020; Liu et al., 2020).
There is a general agreement that the lockdown impacted the daily activites of individuals moving from structured to chaotic daily routines (Ren et al., 2021). This might influence health and the quality of life, since there is evidence that an active participation in daily activities, community activities and meaningful activities has a positive influence on the health and quality of life of people (Petruseviciene et al., 2018; Yaya et al., 2020). Meaningful activities are personally and/or culturally relevant activities which people, in some cases driven by personal values, enjoy and/or feel competent with (Eakman, 2011; B. Goldberg et al., 2002; Plow et al., 2015). Participating in such activities contributes to individual well-being and the satisfaction of psychological, biological and cultural needs for a meaningful life, thus improving people's emotional, cognitive and physical state (Chen, 2020; Eakman et al., 2010; Han et al., 2016; Petruseviciene et al., 2018; Plow et al., 2015). Previous studies have shown the positive impact of participating in daily activities and meaningful activities on mental health (Bjørkedal et al., 2016, 2020; Eklund & Brunt, 2020; B. Goldberg et al., 2002; Kondo et al., 2008; National Guideline Alliance (UK), 2020; Petruseviciene et al., 2018). Thus, as a consequence of the prolonged stay at home due to confinement, the restriction of participating in daily activities and meaningful activities could lead to mental health problems, which will need to be specifically addressed. Some studies have shown that engaging in physical activities and maintaining routines of daily life during lockdown may have been practical strategies to mitigate the potentially harmful mental health consequences associated with the stressors of the pandemic (Ren et al., 2021). More specifically, a recent study (Cruyt et al., 2021) has shown that engaging in meaningful activities contributed significantly to the mental health of the Belgian population in the period of confinement. However, the extent of this phenomenon in the Spanish population during the COVID-19 lockdown has not been analysed to date.
The aim of this study was to determine whether people have continued to carry out their activities during lockdown or if these activities had been interrupted. Thishis study also examined how people adapted their activities in order to maintain them, as well as the specific contribution of participating in meaningful activities on the mental health of Spanish residents during home lockdown.
The hypothesis of this study is two-folded. Firstly, we hypothesised that people found ways to adapt activities to maintain them, especially those that involved contact with others and those that used to be carried out outdoors. Secondly, we hypothesised that the level of participation in meaningful activities contributed substantially to the mental health of residents in Spain, even when controlling for other variables that could also explain this aspect.
Method
A cross-sectional online survey was conducted with a sample of adults in Spain, through the Limesurvey© online platform. The survey was translated into Spanish from the study conducted by Cruyt and colleagues (2021) in Belgium. Four Spanish health science researchers and occupational therapists, with great understanding of the English language, carried out the cross-cultural adaptation of the questionnaire questions, which were not standardised assessment tools. Doubts about the meaning of some items were discussed with Ellen Cruyt's team in order to reach an appropriate formulation of the question. The study adhered to the strengthening of the statement of reports of observational studies in epidemiology (STROBE) (von Elm et al., 2008).
Procedure and participants
The participants were recruited through social networks (Facebook, Twitter) and email (sent to the authors’ 'associations' networks).
The web-based self-reported questionnaire was distributed online in Spain between May 14th and June 12th, 2020, with data collection taking place between these dates. For this study, and due to the period in which the data were collected, the participants were in phases 0, 1 or 2.
The inclusion criteria for participants were adults with Internet access, aged 18 and over, living in Spain, and who were currently in phase 0, 1 or 2, thus excluding people whose communities were already in phase 3. Since we were in a pandemic situation, the questionnaire could only be accessed online, through the Limesurvey© online platform.
This study was approved (April 10th, 2020) by the Ethical Committee of Ghent University (BC-07585). The participants gave their informed consent by clicking on the survey's ‘next page’ button, confirming that they read the information. All methods were carried out in accordance with the relevant guidelines and regulations.
Measures
Following the study carried out by (Cruyt et al., 2021), the questionnaire included standardised tools, sociodemographic questions and questions related to carrying out activities.
Part 1: Socio-demographic and activity-related data
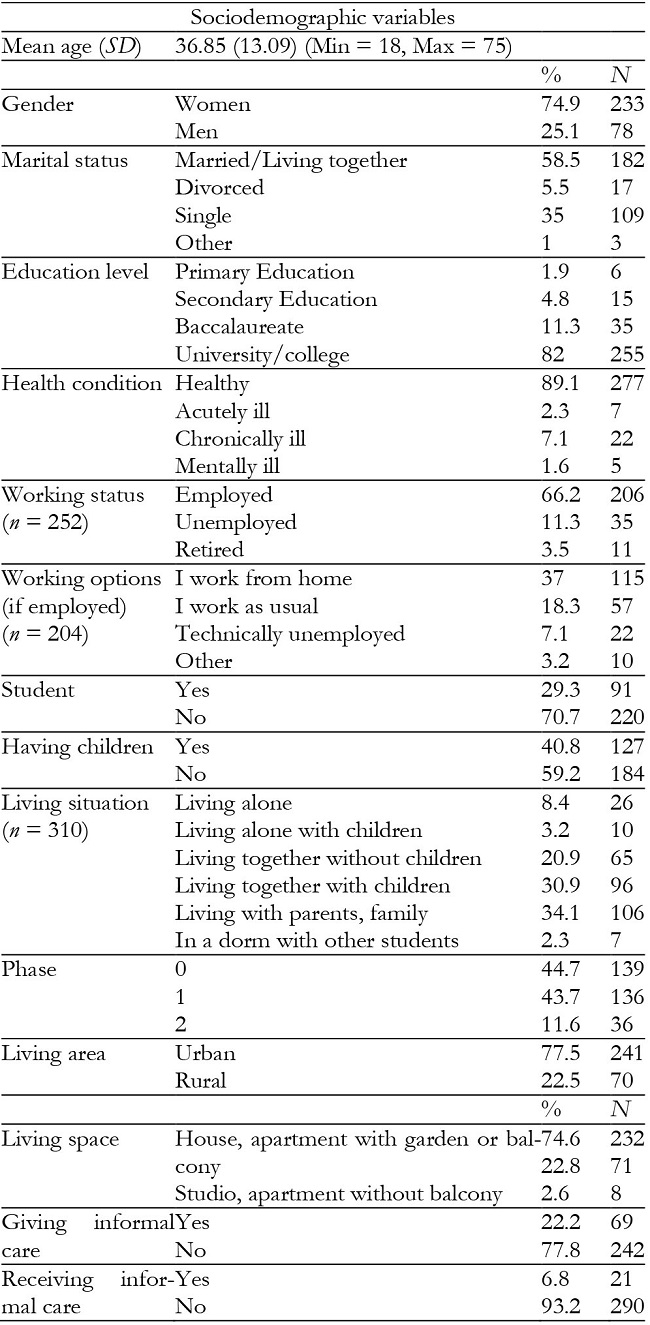
The first part of the questionnaire included the following descriptive variables: age, sex, education level, marital status, having children, employment situation (with work options), living situation, region of residence, living area, living space, phase of confinement in which they were found, health condition and whether the participants were informal caregivers or received informal care.
A fixed list of 18 daily activity categories linked to the nine domains of the International Classification of Functioning and Disability and Health (ICF) (OMS, 2001) was presented to the participants.
The participants were asked to indicate whether or not they performed each of these daily activities prior to the COVID-19 crisis. If so, they had to indicate whether they adapted the activity during the COVID-19 lockdown. Four category options were provided: (1) as usual (in the same way compared to before the COVID-19 crisis); (2) I carry out the activity in another setting (for example, at home instead of at the office); (3) in another way (for example, shopping online instead of shopping on the street); and (4) I do another activity that evokes the same purpose or meaning (for example, going for a walk instead of going to the gym). It was possible to select one or more option responses.
Part 2: Instruments
The general health questionnaire (GHQ). The mental health of the participants was assessed using the 12-item version of the GHQ, which is a valid and reliable instrument to assess psychological well-being and distinct aspects of distress (Goldberg & Hillier, 1979). The Spanish version of this questionnaire showed good internal consistency (Cronbach's alpha = .76), as well as robust external validity with the Inventory of Situations and Responses of Anxiety (ISRA) (.82; Factor II, .70; Factor III, .75) (Sánchez-López & Dresch, 2008).
Each item has four response options using a Likert scale (0 = 'not at all'; 1 = 'not more than usual'; 2 = 'somewhat more than usual'; or 3 = 'much more than usual'). The total sum of scores ranges from 0 to 36, with higher total scores reflecting higher levels of psychological distress. A score of 12 or less in adults indicates psychological well-being (Goldberg et al., 1997).
Connor-Davidson Resilience Scale (CD-RISC). The CD-RISC is a tool that measures personal resilience, which is a concept about healthy and adaptive functioning after adversity (Connor & Davidson, 2003; Southwick et al., 2014). The CD-RISC consists of 10 items and is scored on a 5-point Likert scale that ranges from 0 = 'not at all true' to 4 = 'true almost all the time'. The total score ranges from 0 to 40 points. A higher score indicates greater resilience (Campbell-Sills & Stein, 2007). The CD-RISC is a widely recognised and well-validated resilience measure in Spanish (Notario-Pacheco et al., 2011) showing good internal consistency (Cronbach's alpha = .86) and a clear one-dimensional structure (García-León et al., 2019).
Engagement in Meaningful Activities Survey (EMAS). The 12-item EMAS was used. This measure has been developed to assess the frequency with which people engage in significant activities in their lives, according to a series of dimensions (Eakman, 2012). The participants were asked to indicate how often they carry out each statement (for example, "The activities I do reflect the type of person I am") on a 4-point Likert scale, ranging from 1 = "rarely" to 4 = "always". The total score ranges from 12 to 48. The importance of a person's activities can be low (EMAS < 29), moderate (EMAS 29 - 41), or high (EMAS> 41). The EMAS has been shown to have very good convergent and predictive validity relative to measures of meaning and purpose in life and mental health (Eakman, 2013, 2014; Cruyt et al., 2021), as well as a good internal consistency (α = .81-83) (Lacroix et al., 2018). This tool has been translated and validated in the Spanish context (Fernández-Solano et al., 2022; Prat et al., 2019).
Data analysis
Initially, the sample data were described, and descriptive statistics were also used to indicate the type of activities that people maintained and stopped doing due to COVID-19, as well as the adaptation they made.
Step 1: bivariate analyses
Different bivariate analyses were carried out to determine whether there were differences in the GHQ score for the different nominal and ordinal variables using the Mann-Whitney U-test (gender, having children, living area, informal caregiver, receiving care, living space) and the Kruskal-Wallis test (marital situation, educational level, employment situation, living conditions, confinement phase, work options, health conditions). Variables for which there were significant differences in the GHQ score were entered, in step 2, as explanatory variables in the regression model. In the same way, the Spearman's correlation coefficients were obtained for the continuous variables (age, EMAS and CD-RISC) and those that obtained a significant correlation index with the GHQ score were selected for the regression analysis in step 2.
Step 2: multivariate analysis
A multivariate analysis was applied using hierarchical multiple linear regression analysis. All categorical variables with more than two categories were transformed into "dummy variables" (e.g., the categorical variable “marital situation” became 1 = married, 2 = not married). In model 1, the regression coefficients were calculated for the control variables. The factor "meaningful activities" was added in model 2 to examine the contribution of the frequency of significant activities on mental health, controlling for the remaining key confounding variables (demographic and personal characteristics). The multicollinearity of the models was examined according to the variance inflation factor (VIF) calculations. F-values under .10 were automatically removed, as they are considered insignificant variables.
All statistical analyses were performed using SPSS 26 (SPSS Inc, Chicago, IL), and p < .05 was considered significant in all analyses.
Results
Descriptive results
Sociodemographic variables
A total of 311 participants, recruited by convenience sampling, completed the questionnaire. Table 1 presents the descriptive data of the variables.
Activities during the COVID-19 lockdown
The impact of confinement on activities carried out before and during the COVID-19 home lockdown (before restriction began to be lifted) are shown in Table 2. A high percentage of people had stopped doing social activities (36.4% of 258 people), caring for others outside the family (33.8% of 74 people) and free time activities outside (23.3% of 236 people). Most adults who volunteered (n = 32) before the COVID-19 crisis had to quit these activities. Activities that continued indoors, alone or with the closest family members, such as leisure activities indoors (n = 288), taking care of the family (n = 143), housekeeping (n = 296), doing chores in the house (n = 213) and self-care (n = 306) and tasks related to being a student (n = 146) were largely retained.
Table 2: Percentage of continuity in the participation of activities during COVID-19 lockdown.
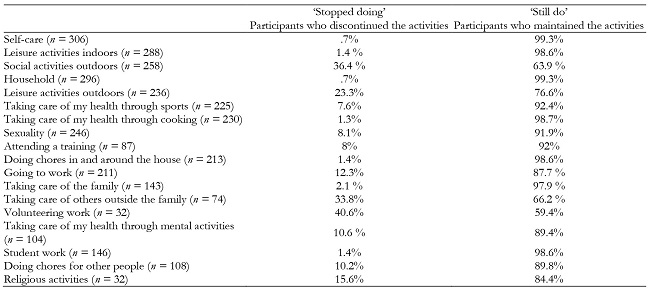
Note.n = number of participants who performed the activity before the COVID-19 crisis.
Table 3 shows that the participants who continued to carry out the activities included a series of changes in order to maintain them.
Table 3: Percentage of the type of changes necessary to maintain participation in activities during the COVID-19 lockdown.

Self-care, home, cooking, activities related to sexuality and housework activities inside and outside the home were carried out in the same way as before the home lockdown, as well as taking care of other people outside the family and taking care of one's own health through mental activities.
The leisure activities that were performed outside and inside the household, as well as sports, work, and religious activities, were carried out mostly in an environment different from the pre-COVID one. The way of doing some activities changed mainly for outdoor social activities, as well as attending a training, volunteer and student work and doing chores for other people. For family care, the highest percentage of responses was concentrated in the response option that indicates that a comparable activity was performed.
Mental health, resilience and meaning in activities
GHQ (Cronbach's Alpha = .89), EMAS (Cronbach's Alpha = .89), and CD-RISC (Cronbach's alpha = .88) showed a good-excellent internal consistency.
The mean GHQ score was 16.12 for the general sample. Based on the threshold score of 12 for adults, the mean score is above the threshold score, which reflects higher levels of psychological morbidity or distress.
The participants obtained a mean score of 25.48 on CD-RISC. Thus, they showed a lower level of resilience, since the cut-off score in this tool is 29 for adults.
Based on the EMAS categories, 56 participants experienced low meaning in their activities (score < 29), 223 participants experienced a moderate sense of meaning in their activities (score between 29 and 41), and 32 experienced high meaning in their activities (score > 41).
Bivariate analysis
The independent variables that were statistically significantly associated with mental health (GHQ) in the Mann-Whitney U-test were gender, having children, being a student, living area, living space, giving informal care and receiving informal care. The results are provided in Table 4. The men scored significantly lower in the GHQ than the women (p = .040), which indicates better mental health. The participants who had children scored significantly lower in the GHQ than those without children, which indicates better mental health (p = .001). Non-students indicated a lower GHQ score (better mental health) than students (p <.001). The participants whose living space consisted of a garden or balcony had a lower score in the GHQ, which reflects better mental health (p = .033). There were no significant differences between those who lived in a rural or urban area (p = .425), those who provided care to others (p = .224) and those who did not, or between those who received care and those who did not (p = .566).
Table 4: Overview bivariate analysis results (1): Mann-Whitney U-test: differences between groups (dichotomous) for the General Health Questionnaire (N = 311).

Note.GHQ= General Health Questionnaire; higher scores in GHQ means lower mental health; SD = Standard Deviation
Marital status, employment status, living conditions, meaning of activities, resilience, and age were the significantly independent variables obtained through the Kruskal-Wallis test associated with mental health. The results are displayed in Table 5. Being married / living together scored significantly lower in the GHQ than being alone (p = .001), indicating better mental health. The participants who were retired obtained significantly lower scores in the GHQ than unemployed people (p = .010). Those who lived together (couples) with children (p = .001) or without children (p = .04) scored lower in the GHQ than the participants who lived with their parent(s) or family (relatives).
Table 5: Overview bivariate analysis (2): Kruskal-Wallis test: differences between groups (categorical) for the General Health Questionnaire according to Mann-Whitney U-test (N = 311).
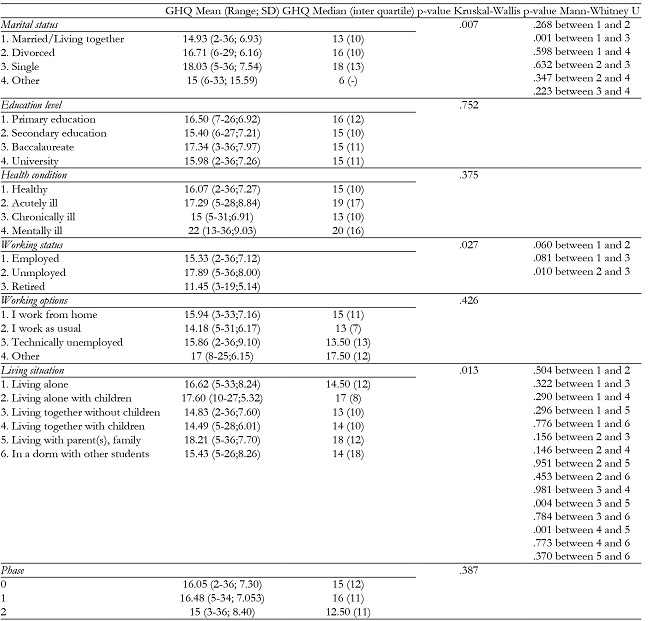
Note.To increase the interpretability of the results, the means and median were included in this table.
The Spearman's Rho test showed a significant moderate relationship between EMAS-GHQ (Rs = -. 376, p < .001) and CD-RISC-GHQ (Rs = -. 494, p < .001). Age was also significantly related to GHQ (Rs = -. 255, p <.001) (Table 6).
Table 6: Overview bivariate analysis (3): Spearman's correlation test: associations between mental health and continuous independent variables in the study sample (N = 311).

Note.EMAS = Engagement in Meaningful Activities Survey; CD-RISC = Connor-Davidson Resilience Scale.
The only VIF factors that showed multicollinearity problems were "living conditions" and "marital status", which reflect whether they live alone or share their life with someone. For a VIF factor of 1, it was decided to exclude living conditions. Similarly, the age variable was closely related to having children (r = -.741; p < .001) and, since it reflects a vital moment, it was decided to eliminate the age variable.
Multivariate analysis
In the next step, mental health was regressed at all seven variables, which were statistically significantly related to mental health during bivariate analysis.
The results of the hierarchical regression analysis are displayed in Table 7. The seven control variables (gender, having children, living space, working status, marital status, being a student, and resilience) were entered at once into Model 1 and accounted significantly together for 31.6% of the variance in mental health (p < .001). After entering meaning in activity (EMAS), the total variance explained by the model was 32.6% (p < .001). In Model 2, EMAS (p = .04) together with living space (p = .045) and resilience (p < .001) contributed significantly to lower scores on the GHQ (better mental health).
Table 7: Hierarchical regression analysis of demographical data, personal factors and meaning in activities associated with mental health.
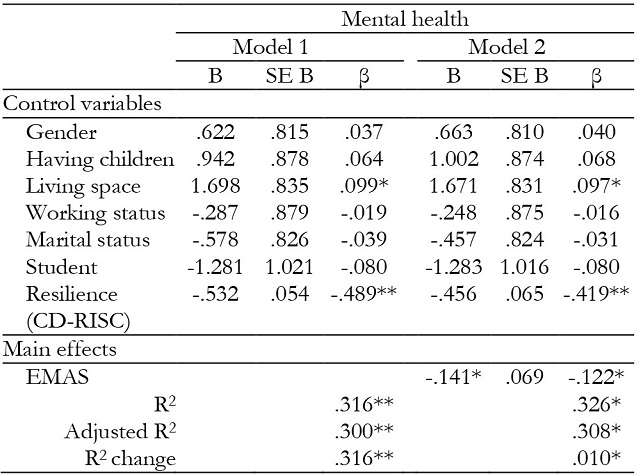
Note.**significant result (p < .001),
*significant result (p < .05);
EMAS= Engagement in Meaningful Activities Survey; CD-RISC= Connor-Davidson Resilience Scale.
Discussion
The present study aimed to analyse the participation in daily and meaningful activities of Spanish adults during home confinement by COVID-19, as well as its impact on and relationship with mental health. When interpreting the data, it is important to note that it was mostly women who responded to the questionnaire (74.9%). Except for the differentiation for the level of mental health (dependent variable) between men and women, the discussion of the results is done for all participants together.
Overall, the participants of the present study (36.85 years) showed a greater alteration of psychological well-being and mental health (GHQ = 16.12) during the period of confinement compared to another similar group of Spanish adults (41.75 years) in a pre-COVID-19 situation (GHQ = 8.52) (Sánchez-López & Dresch, 2008). This fact shows that confinement has had a substantial impact on the state of mental health of the population worldwide, due to mobility restrictions, as other studies have also shown in other populations, such as Turkish (Göl & Erkin, 2021) and Belgian (Cruyt et al., 2021) student populations, making use of the same assessment tool.
For the well-being of the population, it is essential to explain what factors have contributed to reducing the level of mental health or, on the contrary, those that have contributed to improving it. In this sense, this study shows that resilience is the most relevant variable in explaining the level of mental health. In addition, and as a novelty, our study demonstrates that participation in meaningful activities during the confinement period also explains, beyond the contribution of other sociodemographic variables, the reported mental health level of the population in a positive way. These results are in line with what was already discovered by Cruyt et al (2021) in a sample with a Belgian population. This may be due to the fact that, by participating in meaningful activities, people can meet basic needs, such as autonomy, competence and relatedness, which, in turn, makes one's life more meaningful (Eakman, 2013) and increases the perceived well-being (Steger et al., 2008). In the study carried out by (Hooker et al., 2020) with a sample of people with a mean age of 43.3 years, it was found that, when people did more meaningful activities than usual, positive mood increased. In addition, people who participated in a greater number of meaningful activities during the study reported greater vitality and satisfaction with life. Therefore, it is essential within public health programmes, especially after this pandemic, to carry out intervention programmes that increase participation in meaningful activities, with the aim of improving the mental health of the population, using interventions focused on increasing awareness of the meaning attached to such activities, as is proposed by Hooker et al., (2020).
In relation to the maintenance of the different types of activities by the participants, the results of this study show that all the activities that the participants carried out at home before confinement were maintained, i.e., those of self-care and home organisation, such as those aimed at taking care of oneself, through sports activities, cooking or, to a lesser extent, activities such as mental activities, sexual activities, taking care of others or activities associated with the student role. However, and although we do not have pre-pandemic reference data for the Spanish population, following the interpretation of Cruyt et al. (2021), these activities could have been carried out with the simple purpose of satisfying basic needs, without being able to cover psychological needs that contribute substantially to well-being (Eakman et al., 2010).
On the contrary, as might be expected, since phase 0 (n = 139) involved home confinement and phase 2 (n = 136) involved mobility restrictions, the activities that most participants stopped doing were those performed in the outside or that involved contact with people outside the family (volunteering and leisure or social activities outdoors). The lack of opportunities to regularly participate in occupations that are meaningful or necessary due to factors beyond the person's control, such as home confinement, results in occupational deprivation (Whiteford, 2000). Studies in different groups have suggested that the effects of occupational deprivation can include poor health, loss of economic income, loss of capacity and / or social exclusion (Whiteford, 2000), and difficulties in structuring time in a meaningful way (Long et al, 2008).
However, people, as the data show, tried to adapt the way in which they carried out the activities to continue doing them. Work, volunteering, leisure and sports activities, religious activities and those related to studying, were those that required a modification of the environment or way of performance during this period. People wanted to continue keeping themselves busy, since it allows them to develop as people and as members of society (Reed et al., 2011).
Although participation in meaningful activities was a factor that substantially contributed to the mental health of the study population, it should be noted that the contribution of resilience was even greater. During the entire pandemic situation, people faced different continuous stressors, which forced them to minimise the psychological anguish that was generated by them (Chen & Bonanno, 2020). These results are in line with the study of Cruyt et al. (2021), in which this variable also contributed significantly to the GHQ score. Furthermore, as is shown in other studies, resilience mediates the link between changes in daily lifestyles and mental health outcomes, associating higher resilience scores with a reduced rate of anxiety and depression (Barzilay et al., 2020). Moreover, resilience reduced the effects of pandemic fatigue on mental health, sleep quality and job satisfaction in healthcare professionals.
Finally, another sociodemographic factor that contributed to the mental health of the participants was having an outdoor area in the house, which could be a balcony, terrace, patio or garden (Aerts et al., 2021; Dzhambov et al., 2021; Pouso et al., 2021). This may be partly due to the fact that contact with nature might have mitigated the social isolation (Cartwright et al., 2018) that occurred in the period of confinement and / or that there is a space for recovery from stress and promotion of physical activity (White et al., 2020). In the present study, as is also reported in the study of Cruyt (2021), this factor has proven to be a determining factor, having a direct impact on the mental health of the population (Table 7).
The other sociodemographic variables, such as gender, having children, being a student, marital status and working status, did not contribute significantly to determining mental health in the pandemic, although they obtained significant differences in the bivariate analysis. This may be due to the fact that, although they have an influence on the mental health of the population, its contribution is no longer significant when the rest of the variables that had more weight were included, which gives even more relevance to resilience, participating in significant activities and having an outdoor space.
However, it is necessary to discuss that the women in this study showed poorer mental health (higher scores on the GHQ) than the men, which is in line with the results of previous studies that compared both populations (Jacques-Aviñó et al., 2020). In general, regardless of gender, the participants who were married or had a partner also showed better mental health than those who were in opposite situations during confinement, which can be explained by the support received by the other member of the couple (Holt-Lunstad et al., 2008). Although having children during confinement seems to be a factor associated with worse mental health, both the present study and that of Cruyt et al. (2021) showed significant results in the opposite direction. Although in the study by Cruyt et al. (2021) these data could be due to a low percentage of people with children, in our case the sample was much more balanced. Future studies should specify other factors that could substantially influence the results, such as the number of children or their age.
In turn, the bivariate analyses show that the participants who did not have the role of student presented better mental health than students, which may be due, as previous studies also reflect, to the fact that the closure of educational centres, living in confinement and the risk of infection generated anxiety, depression and sleep disorders. These alterations directly affected the educational process, psychological health and well-being of the students, causing, in some cases, post-traumatic stress disorder (Evans et al., 2021; Ma et al., 2021). Finally, the unemployed participants, being in a situation of productive inactivity, reflected poorer mental health, in line with what was reported by Posel et al., (2021), where the negative effect on mental health of unemployment during the pandemic was demonstrated (Posel et al., 2021).
Limitations of the study
This study has some limitations that need to be highlighted. One of the main limitations is that the sample is not representative of the entire Spanish population, and the data, therefore, must be treated with caution, e.g., due to the greater number of female participants in the sample. All the data collected here were self-reported by the participants through a virtual platform, due to the sanitary conditions in force during the study period. Thus, this may have been a bias in the people who participated, who should have a minimum of digital knowledge. Similarly, the data shown here did not indicate causal relationships, since the study was not experimental.
Conclusions
The period of confinement caused by the COVID-19 pandemic has generated a worsening of mental health in the Spanish population. However, this study demonstrates a number of factors that appear to have positively influenced the mental health of the population. Participation in meaningful activities has been crucial in the mental well-being perceived by the population, as well as resilience and having an outdoor space in the home. This information can be valuable at the public health level to generate mental health programmes that allow the population to improve their subjective well-being in the face of future (although unwanted) global crises, such as that caused by COVID-19.

