










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Defining exemption from criminal liability due to insanity is an ongoing issue in international criminal law that has yet to be fully resolved, since it involves questions taken from different sciences and disciplines. The legal treatment of the concept of criminal liability varies according to each country (possibilities of medical diagnosis, cultural context and national case law). The theoretical concepts and management of exemption depend on a complete understanding of epidemiological, medical/psychiatric, social, legal and cultural factors, which in turn generate considerable difficulties for legal administrators1-3.
Although the legal regulation of mentally ill criminal offenders has progressed since its first developments in the early 19th century, the legislative system and its dealings with involuntary commitment and psychiatric treatment requires more scientific analysis and practical improvements. Socio-demographic and medical-legal aspects of exemption have recently taken on particular importance in a number of countries, due to the fact that an increasing number of persons with psychotic disorders commit violent crimes, while simulating a psychiatric disorder enables offenders to avoid or reduce sentencing for very serious crimes. It is necessary to find a balance between the offender's rights and the need for a safer society4,5.
Modern societies strongly associate mental disorders, in particular schizophrenia, with persons who are dangerous and more likely to commit violent crimes. However, studies do not confirm this belief, although they do recognise that a higher possibility of crimes being committed by a mentally ill person may be associated with other unfavourable factors, such as poor education, unemployment, early onset of the disease and certain characteristics of the disorder itself, drug abuse, associated personality disorder, a background of violence, abandonment by the family and lack of access to specialised treatment6,7.
When a crime is committed by someone with a disorder mental that affects a person's cognitive capacities for behavioural regulation or understanding of the nature and social consequences of actions (and omissions), then there is exemption from criminal liability due to a mental disorder. In most cases, the person understands the nature of their actions, but not their consequences, or cannot control them. The concepts of exemption from criminal liability and mental illness are interrelated, but it would be a serious mistake to give them the same weight. Not all mentally ill persons who commit a crime are exempt from criminal liability. Neither is it a requirement to have a background of diagnosis and psychiatric treatment to be declared exempt as a result of diminished responsibility1.
The protection of citizens' health is socially and politically important. Strategic priorities should include vulnerable groups within society. Specialised care for persons with mental disorders should be guaranteed by the state and carried out according to the principles of legality, equality, non-discrimination, humanity and protection of human rights8.
By way of contrast, the Constitutional Court of Peru reported massive and generalised violations of the human rights of persons with diminished responsibility and the existence of an unconstitutional state of affairs with regard to them and to the mental health of prison inmates in general9,10.
The Ombudsman of Peru commented on the non-existence of any policy on the treatment and rehabilitation of persons with diminished responsibility. It also stated that there was a serious infringement of fundamental human rights of this sector of the population, such as the right to liberty, physical safety and health, due to, amongst other factors, the stigmatising spirit of the current Peruvian Criminal Code, which assumes that persons exempt from criminal liability due to mental illness are highly dangerous, combined with a high degree of prejudice amongst healthcare professionals and authorities11-14.
There are very few studies in Peru on diminished responsibility, while official records or statistics on the issue are also few and far between15-18.
The aim of this study was to describe and correlate epidemiological, clinical and legal characteristics of persons with diminished responsibility imprisoned at centres of the National Prison Institute of Peru in the period 2014-2019.
Material and method
Descriptive observational study con correlative components, retrospective, cross-sectional with secondary information sources.
Population and sample
The reference population used was the 95,548 inmates in the 68 prisons of Peru at the end of 2019, 60,669 (63.5%) of whom were convicted offenders18. The sample matched all the persons exempt from criminal liability due to mental illness (n = 179) identified as such during the investigation, who formed part of the prison population between January 2014 and December 2019. A number of them (n = 83) were released during this period as they had completed their period of forced internment and were transferred to a psychiatric hospital or had died. The others (n = 96) remained in prison at the end of the study. The inmates whose diminished responsibility had not been reliably certified by a sentence or court order were excluded. The years prior to 2014 could not be included due to the almost total lack of records.
Data gathering techniqueh
Documentary analysis was used to gather the data19. The data sources were the official documents of the Peruvian public institutions: sentences, rulings and court orders issued by the judiciary, criminal identification sheets, decisions and orders from the National Prison Institute of Peru; psychiatric reports from the Institute of Legal Medicine; reference sheets from the Ministry of Health. The unit of analysis was the patient with diminished responsibility.
The diminished responsibility or exemption from criminal liability in the sample studied had been legally imposed under article 20, point 1, of the Peruvian Criminal Code: “Those persons who do not possess the faculties to understand the criminal nature of their actions or determine their level of understanding of same as a result of psychological anomalies, serious disorders of cognition or difficulties of perception that severely affect their conception of reality, shall be exempt from criminal liability”. This status is only applicable to adult offenders20. The medical diagnoses were the outcome of unstructured clinical psychiatric interviews and based on clinical opinion, knowledge and professional experience, with the support of diagnostic guides and international psychiatric evaluations21,22.
The information was gathered in January to May 2020 by the principal investigator. A data collection sheet prepared by the authors was used. It consisted of 15 items, of which 8 related to the epidemiological characteristics, and the other 7 to clinical and legal ones. The instrument was validated by experts, with Aiken's V content values equal to or more than 0.89 in all the items.
Statistical analysis
The collected data underwent a detailed review by the principal investigator to ensure quality and coherence. The participants were codified to protect their identity. A data base was configured, which was then analysed with descriptive statistics based on the SPSS v24 software (SPSS Inc., USA), to obtain the absolute and relative frequency distributions for the qualitative variables and the means for the asymmetric quantitative variables. A simple logistic binary regression was developed for the inferential analysis, making use of the odds ratio measure of association, the chi square test, considering p <0,05, and a confidence interval of 95%.
Ethical considerations
The study was approved by the Institutional Ethics Committee for Research of the Norbert Wiener Private University (File No. 001-19 of 21 May 2019), and met the standards of the Helsinki Declaration23. No informed consent was required given that the study involved a documentary analysis. The confidentiality of the information and its use solely for scientific ends were ensured throughout all the study procedures.
Results
Descriptive analysis
The results of the study showed that there were 179 persons exempt from criminal liability due to mental illness who passed through the Peruvian prison system from 2014 to 2019. These persons were found in 36 (41.9%) of the prisons nationwide. The prison with the largest population of persons with diminished responsibility was Lurigancho prison (Lima prison department), the only one in Peru that provides psychiatric hospitalisation, with 36.9% (n = 66) of cases, followed by Cusco Varones prison (Sur Oriente Cusco prison department) with 10.6% (n = 19) and Huánuco prison (Oriente Pucallpa prison department) with 7.3% (n = 13) of cases. The distribution of persons with diminished responsibility according to prison departments can be seen in Table 1.
Table 1. Distribution of persons with diminished responsibility according to regions of the National Prison Institute of Peru, 2014-2019.
| Regions | n | % |
|---|---|---|
| Lima | 98 | 54.7 |
| Sur Oriente Cusco | 22 | 12.3 |
| Norte Chiclayo | 19 | 10.6 |
| Oriente Pucallpa | 15 | 8.4 |
| Centro Huancayo | 10 | 5.6 |
| Sur Arequipa | 8 | 4.5 |
| Nor Oriente San Martín | 4 | 2.2 |
| Altiplano Puno | 3 | 1.7 |
| Total | 179 | 100 |
94.4% (n = 169) of the sample were men. The average age was 35 years, with minimum and maximum ages of 20 and 72 years; 11 persons (6.1%) had no identity document and were not included in the National Registry of Identification and Marital Status. The main socio-demographic characteristics of the persons with diminished responsibility can be seen in Table 2.
Table 2. Socio-demographic characteristics of persons with diminished responsibility according to the National Prison Institute of Peru, 2014-2019.
| Characteristics | n | % |
|---|---|---|
| Origin (n = 179) | ||
| Lima Metropolitana and Callao | 69 | (38.5) |
| Coast, except Lima and Callao | 35 | (19.6) |
| Peruvian highlands | 67 | (37.4) |
| Peruvian rainforest | 7 | (3.9) |
| Foreign | 1 | (0.6) |
| Educational level (n = 179) | ||
| Illiterate | 11 | (6.2) |
| Special education | 1 | (0.6) |
| Primary | 29 | (16.2) |
| Secondary | 120 | (67.0) |
| Vocational | 2 | (1.1) |
| University | 16 | (8.9) |
| Occupation outside prison (n = 179) | ||
| Unemployed with occasional work | 93 | (52.0) |
| Labourer | 78 | (43.5) |
| Employee | 3 | (1.7) |
| Professional | 5 | (2.8) |
| Marital status (n = 179) | ||
| Single | 165 | (92.2) |
| Married | 9 | (5.0) |
| Cohabitee | 4 | (2.2) |
| Widower | 1 | (0.6) |
The average duration of the involuntary commitment was 11.2 years, with the minimum period being 6 months and the maximum 35 years. In 74.6% of the cases, the length of involuntary commitment was more than five years, and over 33.6% were confined for more than 10 years. 11.5% remained in prison although the detention period established by court order had effectively expired. A previous criminal background was found for only 11.2% of the persons with diminished responsibility. Other legal characteristics of these persons can be seen in Table 3.
Table 3. Legal characteristics of persons with diminished responsibility according to the National Prison Institute of Peru, 2014-2019.
| Characteristics | n | % |
|---|---|---|
| Offence committed* (n = 179) | ||
| Homicide and assault (title I) | ||
| Homicide (article 106°. 108°) | 36 | (20.1) |
| Parricide (art. 107°) | 20 | (11.1) |
| Grievous bodily harm (art. 121°) | 10 | (5.6) |
| Crimes against freedom (title IV) | ||
| Coercion (art. 151°) | 1 | (0.6) |
| Kidnapping (art. 152°) | 2 | (1.1) |
| Trafficking of persons (art. 153°) | 1 | (0.6) |
| Rape (art. 170°) | 47 | (26.2) |
| Touching. acts with sexual connotations or sexual acts without consent (art. 176°) | 19 | (10.6) |
| Crimes against property (title V) | ||
| Aggravated larceny (art. 186°) | 1 | (0.6) |
| Aggravated theft (art. 189°) | 23 | (12.7) |
| Fraud (art. 196°) | 1 | (0.6) |
| Aggravated damage (art. 206°) | 1 | (0.6) |
| Financial and monetary offences (title X) | ||
| Manufacture and Forgery of currency legal tender (art. 252°) | 1 | (0.6) |
| Crimes against public safety (title XII) | ||
| Manufacture, supply or possession of hazardous materials and waste (art. 279°) | 1 | (0.6) |
| Promotion or encouragement of illegal trafficking of drugs and other substances (art. 296°) | 7 | (3.9) |
| Crimes against the public administration (title XVIII) | ||
| Illegal exercise of profession (art. 363) | 1 | (0.6) |
| Crimes against public order (title XIX) | ||
| Falsification of documents (art. 427°) | 1 | (0.6) |
| No data | 6 | (3.3) |
| Place of involuntary commitment determined by judge (n = 179) | ||
| Hospital Víctor Larco Herrera (HVLH)-Lima. Peru | 34 | (19.0) |
| Hospital Hermilio Valdizán (HHV)-Lima. Peru | 22 | (12.3) |
| National Institute of Mental Health Honorio Delgado-Hideyo Noguchi (INSM HD-HN)-Lima. Peru | 10 | (5.6) |
| Other establishment of the Ministry of Health | 7 | (3.9) |
| Establishment of the Social Security (EsSalud) | 4 | (2.2) |
| Public welfare establishment | 5 | (2.8) |
| Not specified | 64 | (35.8) |
| Department of Mental Health of the National Prison Institute of Peru | 33 | (18.4) |
Note. *According to current Peruvian Criminal Code (DL No. 635 of 1991).
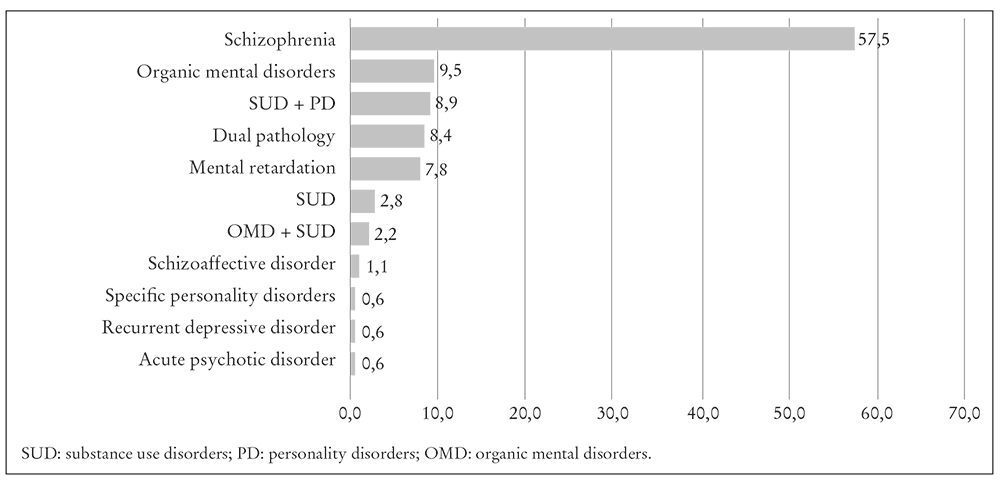
The main psychiatric diagnoses in the sample can be seen in Figure 1. 22.3% (n = 40) consumed illegal drugs prior to hospitalisation. 46.9% (n = 84) of the persons with diminished responsibility were found to have a background of psychiatric treatment before committing the crime. 67.7% (n=65) of the 96 persons with diminished responsibility recruited at the end of the study were medically discharged.
Bivariate analysis
Associations between specific clinical variables (e.g. diagnosis) and legal ones, such as the type of crime, were identified. These can be seen in Table 4.
Table 4. Association between clinical variables and offences amongst persons with diminished responsibility according to the National Prison Institute of Peru. 2014-20199.
| Variable | c2 | OR (IC: 95%) | p |
|---|---|---|---|
| Crimes against public safety and property | |||
| Background of drug abuse | 30.34 | 0.12 (0.05-0.27) | <0.001 |
| Homicide and assault | |||
| Schizophrenia spectrum disorder | 4.13 | 2.02 (1.02-4.00) | 0.044 |
| Crimes against freedom | |||
| Mental retardation | 15.68 | 21.10 (2.68-166.46) | 0.044 |
| Serious offences | |||
| Background of drug abuse | 15.99 | 0.21 (0.09-166.47) | <0.001 |
Note. IC: confidence interval; OR: odds ratio.
Discussion
This study is the first one in Peru to quantify persons exempt from criminal liability due to mental illness who passed through the national prison system, and the first to describe their epidemiological, clinical and legal characteristics. Adequate identification and recording of persons with diminished responsibility in prison is the first step in recognising the problem when official figures cannot be found. Strategies are also needed that can help to put an end to the massive and general violation of their fundamental rights, reverse the unconstitutional state of affairs through the Constitutional Court9, and to plan the appropriate medical and preventive measures. It is important to evaluate the problem in all its dimensions, with the added perspective of national and international experiences.
The socio-demographic results obtained enabled us to identify a characteristic profile of the patients with diminished responsibility in the sample: male, middle aged, from the capital or mountain regions, different number of years in secondary education, unemployed or working in jobs where specialised academic training is not required, without a partner or children. This profile matches other Peruvian16,17,24, Latin American6,25, European26,27 and African studies28. On the other hand, a study in the USA found an average age of 42.2 years; older than the ages found in this study, although the American study only included persons with diminished responsibility sentenced for sexual crimes. The same study showed considerable ethnic diversity; reflecting the American population in general29.
As regards the legal characteristics, the main offences in the sample were against sexual freedom (39.1%) homicide, assault and drug-related offences (36.8%), followed by offences against property (14.5%). A Colombian study showed a sample distribution of 10.2%, 74.0% and 11.1%, respectively6. A study in Belgium showed a predominance of violent crimes (58.0%), followed by sexual (20.9%) and other offences (21.1%)26. Swedish persons committed offences against property, homicide and sexual offences in 40.9%, 12.1% and 9.4%, respectively30. In studies carried out in Russia, the offences committed by persons exempt from criminal liability were against property (41.0%), homicide (15.7%) and sexual offences (3.1%). Hospitalised patients under special regime committed serious offences with violence in 48.4% of cases, offences against property without violence were the most common offence committed by outpatients with diminished responsibility (57.7%)27,31. South African persons with diminished responsibility committed offences against persons in 87.9% cases and against property in 7.7% of cases28. The differences found can be explained by the specific characteristics of the criminal law in each country, as well as the diversity of criteria, procedures and resources used to establish diminished responsibility die to mental illness and the different systems of obligatory commitment and confinement used.
A notable feature of the study was the predominance of schizophrenia spectrum disorders (67.0%), although organic mental disorders, mental retardation and drug-related pathologies were also common. The prevalence of schizophrenia in the study sample (57.5%) was similar the one reported in the Colombian (63.0%)6, but significantly higher than the findings in the Swedish research (33.6%)30 and lower than the Canadian study (77.9%)32. The Turkish study showed a prevalence of schizophrenia of 42.5%, below the level in this study, but the presence of affective disorders was significantly higher (19.5%)33. One possible explanation may be differences in diagnostic criteria, times and conditions of the medical-legal evaluation, and access to information about the psychiatric background prior to the offence, which is a factor mentioned by other authors3,4,28. In Peru, there is no forensic psychiatric hospital, which is one of the structural defects in the diagnosis, treatment and rehabilitation of persons exempt from criminal liability, especially when compared to other countries29,30.
The mental pathology of patients with diminished responsibility also varies, depending on the type of sample, according to other characteristics such as the offence that was committed. In this study, the prevalence of diagnoses related to congenital or acquired organic cerebral pathologies (19.5%) was lower than in the American study, which found intellectual or cognitive impairment in 64.0% of the persons with diminished criminal responsibility29.
The prevalence of drug use (22.3%) reported in the research was less than in the Chilean study amongst pyromaniacs25 and sexual offenders in the American study29 with a prevalence of 41.1 and 47.0%, respectively.
The study on Italian women who had committed homicide and were declared exempt from criminal liability showed a prevalence of schizophrenia (60.0%) similar to the results in this study, although the sample used here was made up mostly of male patients who had committed other crimes34.
This study also set out to associate mental pathologies with the type of criminal offence, and found a statistically significant association between schizophrenic spectrum disorders and offences such as homicide, parricide and grievous bodily harm; while mental retardation was associated with crimes against freedom, mainly sexual assault, which matches the results in other studies29,33,34.
Escobar-Echavarría et al. reported schizophrenia as a risk factor when the victim is a family member or acquaintance. However, mental retardation is a protective factor against the same variable6. On the other hand, a statistically significant association was found between drug abuse and offences against property (aggravated theft) and against public safety (drug trafficking). The same variable was associated with serious offences, consisting of those with sentences of more than five years20.
More wide-ranging and homogenous research projects are required that include links between the mental pathology and the type of criminal conduct. Other aspects that should be considered in future studies are the characteristics in the development of mental disorders, such as premorbid conditions, the onset of the illness, its progress, access to health services, availability and adherence to treatment, comorbidities, social and family support. etc., and the resulting likelihood of dangerous and illegal behaviour3,26,31.
In the vast majority of the cases studied, the duration of the involuntary commitment was more than five years, with an average of 11.2 years and a maximum of 35. These findings match those in the American study on the average duration of hospitalisation (10.5 ± 6.7 years). However, the maximum duration of internment was longer (45 years)29. The maximum term was forty years in the Colombian study6. On the other hand, the European studies showed that forensic psychiatric hospitalisation was on average shorter than in this study (0.4-4.5 years)26,30. In the Russian study, only 5.1% of cases were interned for more than ten years4, which is way below the results obtained this study (33.6%). The excessive length of mandatory hospitalisation, which is issued in court according to the prison sentence established for the type of offence20, contradicts medical criteria and evidently infringes rights to health and freedom. This situation was denounced by the Ombudsman on a number of occasions11-14. The studies show that in cases of offences committed as a result of psychotic disorders, prolonged internment leads to a progressive deterioration of the personality, physical impairment and problems in family, labour and social adaptation4.
In this study, 67.7% of the persons with diminished responsibility had been given a medical discharge, which was not taken into consideration by the court administrators as a determining factor in terminating the confinement provided for in the Criminal Code20. A similar problem was reported in Peruvian psychiatric hospitals24. In addition, 11.5% of the persons with diminished responsibility stayed in prison even though the confinement period had ended, which is a serious infringement of their right to freedom.
According to the Peruvian Mental Health Act and its regulations, the length of enforced hospitalisation should not exceed the time established by the medical committee of the healthcare department. Patients with diminished responsibility are only hospitalised in conditions of clinical instability and to bring about objectives that cannot be achieved through outpatient treatment. Stigmatising activities such as custody, hostels or preventive imprisonment should be eradicated since they generate stigmas associated with mental asylums. Alternatives to hospitalisation include mandatory outpatient treatment or a protected home or residence35,36, in line with the conclusions drawn in international studies6,37 carried out in contexts similar to those in Peru.
Other findings in this study include the fact that 6.1% of the persons exempt from criminal liability due to mental illness did not have any identification in the Peruvian national system, making it impossible for them to carry out civil or legal actions and thus violating their rights to identity38.
Most of the persons with diminished responsibility in the prison system should have been sentenced to commitment in public hospitals but did not go there because of the lack of beds. They were sent to prison modules to live alongside other prisoners where they are exposed to abuse and mistreatment12,13. However, the budget for hospitalisation of persons with diminished responsibility was assigned to the 15 hospitals under the control of the Ministry of Health, of which 11 did not report that they had been admitted14.
The situation is even more serious since 18.4% of the sentence stipulated that prison healthcare units as the location where the patient's sentence was to be served. In addition, 35.8% of the sentences do not specify the place of internment. This means that a significant number of persons with diminished responsibility are in prisons, which clearly contradicts article 74 of the Criminal Code20 and is a serious violation of these patients' fundamental rights. The only prison that has a psychiatric hospital service in Peru is Lurigancho, but the psychiatric care conditions to be found there do not meet the technical standards for healthcare, according to a report by the Ministry of Health39. It should also be mentioned that Peru does not have an adequate forensic psychiatric system in comparison to other countries26-27,29-32,40.
The limitations of the study include the fact that the persons with diminished responsibility were identified from the available court records, and such data may have potential problems of under-recording. The years prior to 2104 could not be considered because there was almost no data for that period.
Conclusions
The main epidemiological, clinical and legal characteristics of the persons exempt from criminal liability due to mental illness incarcerated in prisons of the National Prison Institute of Peru in the period 2014-2019 were described and presented in comparison with cases in other countries. Aspects of the current situation were identified that do not comply with national and international regulations (excessive length of internment, in unsuitable places and with unjustified deprivation of liberty, etc.), and infringe the fundamental human rights of this group. Associations between variables such as diagnosis and the type and seriousness of the crime were also found.
The findings of this study not only provide data to enable greater understanding of the problems associated with exemption from criminal liability due to mental illness in Peru, it also opens the way to proposals for corrective, preventive and promotional measures with a greater focus on human rights, interdisciplinary processes and crime prevention, as part of the reform of mental healthcare currently in progress. Major changes in the mental healthcare system are required, including but not limited to the creation of a comprehensive, solid and sustainable mechanism for care, assessment, treatment, rehabilitation and re-socialisation of persons with mental disorders who commit criminal offences, and the updating of the Criminal Code and other relevant legislation.

