










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 no.6 Madrid jun. 2015
PICTURES IN DIGESTIVE PATHOLOGY
A peripheral approach allowing successful endoscopic submucosal dissection for early colorectal carcinoma near the diverticula
Hideki Kobara1, Hirohito Mori1, Kazi Rafiq2, Shintaro Fujihara1 and Tsutomu Masaki1
1Department of Gastroenterology and Neurology.
2Department of Pharmacology. Faculty of Medicine. Kagawa University. Kagawa, Japan
Case report
An 86-year-old man presented with a positive fecal occult blood test. Colonoscopy revealed a 25-mm laterally spreading tumor near the diverticula located in the ascending colon (Fig. 1). Magnifying endoscopy indicated a carcinoma with adenoma, suggesting that en bloc resection by endoscopic submucosal dissection (ESD) would be optimal. In designing a strategy for this lesion, the most important issue was marginal cutting near the diverticula for complete resection without adverse events. Informed consent was received from the patient.

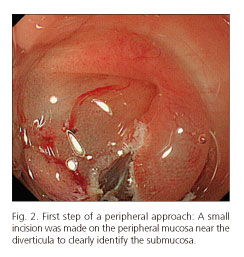
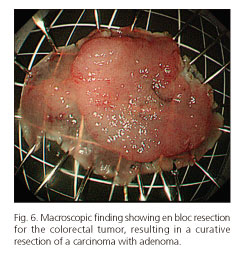
Firstly, a small incision was made on the peripheral mucosa near the diverticula to clearly identify the submucosa, followed by submucosal injection of 0.4% hyaluronate sodium solution (MucoUp; Johnson & Johnson K.K., Tokyo, Japan) with a needle knife (KD-441Q; Olympus, Tokyo, Japan). The mucosa nearest to diverticula was dissected using the needle knife from the peripheral mucosa toward the side of diverticula, resulting in safe and complete marginal cutting of the mucosa near the diverticula (Fig. 2), and followed by standard colorectal ESD. The entire dissected surface, including the diverticula, was sutured with hemoclips to prevent late complications. Histological examination revealed a curative resection of a carcinoma with adenoma. The patient was hospitalized for 1 week without associated complications and showed excellent postoperative outcomes.



Discussion
ESD is a standard therapeutic procedure for early colorectal carcinoma (1). However, various factors make en bloc resection for colorectal tumors difficult or unsafe (2). Accordingly, it is unclear whether ESD is the appropriate treatment for early colorectal carcinoma near or within the diverticula (3). Complete full-thickness dissection, a novel type of surgery using laparoscopic and endoscopic techniques, may be adaptable for colorectal tumors within the diverticula (4). Our findings suggest that the peripheral approach is safe and effective for early colorectal carcinoma near the diverticula.
References
1. Tanaka S, Tamegai Y, Tsuda S, et al. Multicenter questionnaire survey on the current situation of colorectal endoscopic submucosal dissection in Japan. Dig Endosc 2010;22:S2-8. [ Links ]
2. Takeda T, Murakami T, Sakamoto N, et al. Traction device to remove an adenoma in the appendiceal orifice by endoscopic submucosal dissection. Endoscopy 2013;45:E239-40. [ Links ]
3. Gotoda T, Takenaka R, Inokuchi T, et al. Endoscopic submucosal dissection for a superficial esophageal squamous cell carcinoma within the parabronchial diverticula. Dig Endosc 2013;25:91-2. [ Links ]
4. Fukunaga Y, Tamegai Y, Chino A, et al. New technique of en bloc resection of colorectal tumor using laparoscopy and endoscopy cooperatively (laparoscopy and endoscopy cooperative surgery - colorectal). Dis Colon Rectum 2014;57:267-71. [ Links ]

