










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.110 no.4 Madrid abr. 2018
https://dx.doi.org/10.17235/reed.2017.4911/2017
PICTURES IN PATOLOGY DIGESTIVE
Cholangitis secondary to afferent loop syndrome from a gastric stump adenocarcinoma
1Servicios de Aparato Digestivo. Complejo Hospitalario Universitario de A Coruña. A Coruña, España
2Servicios de Cirugía General. Complejo Hospitalario Universitario de A Coruña. A Coruña, España
CASE REPORT
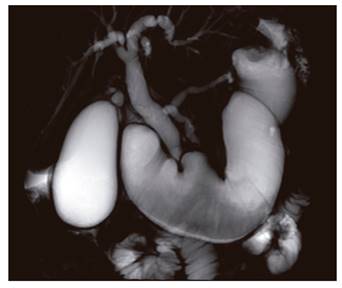
An 85-year-old patient who had undergone a subtotal gastrectomy and Billroth-II reconstruction for ulcer disease 40 years ago was admitted due to abdominal pain and jaundice. The laboratory parameters were as follows: total bilirubin: 2.1 mg/dl, NR: 0-1.3 mg/dl; direct bilirubin: 1.5 mg/dl, NR: 0-0.3 mg/dl; and alkaline phosphatase: 2.369 IU/l, NR: 91-240 IU/l. An ultrasound scan revealed a dilated biliary tree with echogenic material inside. The afferent loop could not be reached via endoscopic retrograde cholangiopancreatography (ERCP) due to a neoformation at the gastric stump; biopsies confirmed an intestinal type adenocarcinoma. Magnetic resonance cholangiography (Fig. 1) identified an ulcerated growth on the gastric remnant with secondary afferent loop dilation and bile duct dilation. The patient was managed surgically with a total gastrectomy and Roux-en-Y reconstruction and had a favorable outcome.
DISCUSSION
Afferent loop syndrome is a complication of a partial gastrectomy with Billroth-II gastrojejunostomy or cephalic duodenopancreatectomy, with an incidence of 0.2-20.0% 1. It may arise from adhesions, loop angulation, anastomotic strictures, internal herniation or tumor relapse 2. Biliary and pancreatic secretions accumulate in the afferent loop, which results in distension and may lead to necrosis and perforation. In our case, high pressure in the afferent loop resulted in a secretion reflux into the biliary tree which induced secondary cholangitis. As a neoplastic obstruction was the primary cause, surgical treatment was performed. Cases managed endoscopically have been reported, with the production of gastrojejunal fistulae using lumen-apposing stents which may play a greater role in poor surgical candidates in the future 3.
BIBLIOGRAFÍA
1. Aimoto T, Uchida E, Nakamura Y, et al. Malignant afferent loop obstruction following pancreaticoduodenectomy: report of two causes. J Nippon Med Sch 2006;73:226-30. DOI: 10.1272/jnms.73.226 [ Links ]
2. Lehnert T, Buhl T. Techniques of reconstruction after total gastrectomy. Br J Surg 2004;91:528-39. DOI: 10.1002/bjs.4512 [ Links ]
3. Shah A, Khanna L, Sethi A. Treatment of afferent limb syndrome: novel approach with endoscopic ultrasound-guided creation of a gastrojejunostomy fistula and placement of lumen-apposing stent. Endoscopy 2015;47:E309-10. DOI: 10.1055/s-0034-1392210 [ Links ]
