










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Metabolic syndrome (MetS) is characterized by a cluster of cardio-metabolic risk factors that includes abdominal obesity, high blood pressure, increased glucose concentrations, and dyslipidemia 1,2. MetS is highly-prevalent in geriatric populations, where it varies from 11-43%, 23-55%, and 37-41.9%, according to the World Health Organization, the National Cholesterol Education Program-Third Adult Treatment Panel (ATP III), and the International Diabetes Federation (IDF), respectively 3,4,5,6,7. The clinical impact of MetS in older adult populations consists in its association with cardiovascular morbidity 4,7,8,9,10 and mortality 11,12,13.
The underlying causes of MetS are still being studied. Though insulin resistance and central obesity are currently considered as the most significant factors 1, other important contributing factors include inflammation, endothelial, renal and hepatic dysfunction, and oxidative stress 14. Also, recent studies had reported an association of MetS with such gender-specific risk factors as demographic variables (socioeconomic status, educational level and marital status, among others) in adult 15,16 and older adult subjects 17,18,19,20,21. To our knowledge, there are few specific studies of the association between socioeconomic status and MetS in older people, and even fewer of older people in developing countries. It is well-known that the prevalence of MetS increases with age, especially in individuals with high body-mass index (BMI) and low levels of physical activity 22.
In Mexico, the over-60 population has grown considerably. At the same time, obesity, central obesity, type 2 diabetes and hypertension, among other ailments, have become significant public health issues 23,24. In addition, an important segment of older Mexican people have low educational levels, a large proportion has neither formal jobs nor pensions, and others have extremely low incomes. Many are single; indeed, living alone is quite common in this age group 25. Unfortunately, few data exist on the prevalence and determinants of MetS in relation to cardio-metabolic, body composition and inflammatory profiles, or to associated demographic factors in older people from low- and middle-income countries. Therefore, the objective of the present study was to estimate the prevalence of MetS and, secondly, to explore which of the cardio-metabolic, body composition, inflammatory and demographic risk factors were associated with the prevalence of MetS in a population of older Mexican adults.
METHODS
A non-probabilistic, cross-sectional study was conducted with older people from the city of Hermosillo and some rural areas of Municipality of Hermosillo, Sonora, Mexico. During visits to homes and clubs, short interviews were conducted to invite older people to participate, in order to gather information on their health and nutritional status. All potential participants then underwent a comprehensive medical examination, an oral glucose tolerance test (OGTT) and other biochemical determinations. Anthropometric measurements were taken and body composition was assessed. A series of demographic variables was also evaluated as part of the study protocols. The research protocol was carried out in the Laboratory of Body Composition and Functionality, Coordination of Nutrition, Research Center for Food and Development, and was approved by the Ethics Committee of CIAD, A.C. All volunteers were fully informed and signed the consent form before commencing the protocol.
STUDY POPULATION
The total sample comprised 369 participants, and included 195 women and 174 men over 60 years old (range: 60-83 years) who were physically independent according to the Katz scale 26 and in free-living conditions. Participants underwent a general medical examination and urine analyses and an oral glucose tolerance tests (OGTT). Subjects were free of type 2 diabetes as determined by the OGTT and the 1997 ADA criteria 27 and were also free of other major chronic diseases, according to their clinical histories. Controlled hypertensive subjects and those with controlled endocrine disorders such as hypothyroidism were included.
MEASURES
Anthropometry and body composition assessment
Body weight and standing height were recorded, and BMI (kg/m2) was determined and used as indirect marker of adiposity (overweight and obesity) 28. Waist circumference (WC) was measured to the nearest 0.1 cm at the umbilicus level using a fiberglass measuring tape. Body composition including fat-free mass (FFM), total appendicular skeletal muscle mass (TASM) and fat mass (FM) was measured by DXA using DPX-MD+(tm) (GE Lunar Madison, WI, USA), as previously published 29. Fat mass index (FMI), kg/m2 was obtained and considering the FMI values and the classification proposed by Kelly et al. (2009), three categories were formed 30. Both, FM and FMI were used as direct marker of adiposity.
Cardio-metabolic and inflammatory biochemical determinations
After an 8-12 h overnight fast, whole blood samples (20 ml) were collected. Glucose levels were measured using the glucose oxidase method, while serum insulin was analyzed by radioimmunoassay (Iso Data, IL, USA) following the Coat-A-Count(r) procedure (Coat-A-Count, DPC) and by enzyme-linked immunosorbent assay (DRG Instruments GmbH, Marburg, Germany), using ALPCO(tm) (cat. EIA2935 DRG). The homeostasis model assessment (homa) of insulin resistance (HOMA-IR) was calculated using the Matthews' equation 31 and insulin resistance was defined based on percentile distribution using the 75th percentile (HOMA-IR = 2.43). Lipid profile was calculated by the enzymatic-colorimetric method and, more recently, by RX monza (Randox Laboratories Ltd; Crumlin, UK). Serum interleukin 6 (IL-6) and C-reactive protein (CRP) concentrations were measured by ELISA High Sensitivity HS600 Quantikine(r) kit (R&D Systems Inc., Minneapolis, MN, USA).
Blood pressure measurements
Blood pressure (BP) was measured with a mercury column sphygmomanometer (Graham-Field(tm) Inc., NY, USA). The values reported are the mean of two measurements. In relation to the application of the MetS criteria, subjects with a systolic BP > 130 or diastolic BP > 85 mmHg, or who were taking medications for previously-diagnosed hypertension were registered as hypertensive (ATP III and AHA/NHLBI), while for the 2009 IDF standards, systolic BP ≥ 130 or diastolic BP ≥ 85 mmHg, or treatment of previously-diagnosed hypertension were the parameters used.
Assessment of demographic variables
In the study protocol, age and gender were recorded. Family income was ascertained from the amount estimated by subjects considering all household members who contributed to total monthly family income. Classification of socioeconomic status followed the procedure in Esteban et al. (2007) obtaining three socioeconomic (SES) groups (Low SES group: 38.7%; medium: 46.7%; high: 14.6%) 32. The estimates in this study for the low SES group (the poor) comprised 52%, in line with those shown in official poverty figures from CONEVAL (2015) 33. In addition, educational level was classified in accordance with Mexico's educational system. Technical careers were also considered when classifying educational levels. Marital status, toxicities (smoking and alcoholism) and employment status were identified.
Physical activity level
Physical activity levels (PAL) were estimated by predictive equations that estimate total energy expenditure and resting metabolic rate in older people 34. PAL was classified as sedentary, moderately active, vigorously active, and extremely active 28.
Diagnoses of MetS
We applied three sets of criteria to diagnose Mets: ATP III 35, ATP III modified by the AHA/NHLBI in 2005 (AHA/NHLBI) 1, and the 2009 IDF classification 36. For the 2009 IDF criteria 36, the cut-off points for WC recommended for Asian populations were used.
Statistical analysis
Student's t-tests or Chi-squared tests were used to compare several characteristic of the subjects with and without MetS. The main associated factors of the MetS were explored by multiple logistic regression, both univariate analysis and multivariate stepwise regression methods. It is important to specify that models were constructed separately for MetS as diagnosed by the ATP III, AHA/AHLBI, and 2009 IDF criteria. Models were evaluated for logistic regression assumptions (i.e., lack of strongly-influential outliers) and interactions of all variables in the model with gender were tested at p ≤ 0.1. All analyses were performed using STATA (version 11.0; Stata Corp, College Station, TX, USA).
RESULTS
The mean age of the total sample was 68.9 ± 6.5 years, and they had a mean BMI of 27.3 ± 3.9 kg/m2. Women represented 53% of the total sample. Overall prevalence of MetS was 36% and 45% according to ATP III and AHA/NHLBI, respectively, increasing to 52% with the 2009 IDF criteria.
Table I shows the behavior of several cardio-metabolic, marker of adiposity, inflammatory and demographic variables according to the different criteria used. Subjects with MetS were heavier and had greater BMI, FM, FMI, and WC. Overweight and obesity were more prevalent in subjects with MetS, regardless of the criteria applied (p < 0.0001). Additionally, they had higher values of triglycerides and lower values of total HDL-cholesterol compared to those without MetS (p < 0.0001). Fasting glucose, insulin and HOMA were significantly higher in the MetS group diagnosed by AHA/NHLBI and 2009 IDF criteria. Also, an effect of gender and hypothyroidism was found. MetS was also more prevalent in older subjects with educational levels of high school or less, single or widowler or divorce, low socioeconomic status, and those who were sedentary or had low physical activity levels, regardless of the criteria applied.
Table I Behavior of several cardio-metabolic, body composition compartments, inflammatory and demographic variables according to MetS status as defined by three different sets of criteria

BMI: body mass index; HOMA: homeostasis model assessment; TASM: total appendicular skeletal muscle; HDL: high-density lipoprotein; LDL: low-density lipoprotein; CRP: C-reactive protein; IL-6: interleukin 6; SES: socioeconomic status; PAL: physical activity level. A Student's t-test was used for continuous variables and Chi-squared test for categorical variables.
Table II Univariate associations of potential predictors of MetS as defined by three different sets of criteria

BMI: body mass index; HOMA: homeostasis model assessment; TASM: total appendicular skeletal muscle; HDL: high-density lipoprotein; LDL: Low-density lipoprotein; SES: socioeconomic status; PAL: physical activity level; FMI: fat mass index; Ref: reference. †Variables not selected for the multivariate analysis according to the criteria p≤0.2 and/or a reduced number of observations or categories. OR: odds ratio; SE: standard error.
Table II shows the potential predictors of MetS. Waist circumference, BMI, FM, FMI, fasting glucose and insulin, HDL-cholesterol, triglycerides, gender, educational level, alcohol consumption, PAL, BMI, owerweight and obesity by BMI classification and hypertension, all proved to be predictors of MetS defined by all three sets of criteria (p ≤ 0.2). Other variables were selected as predictors of MetS, but for only one or two criteria, such as residence (rural and urban), marital status, socioeconomic status, obesity by FMI classification and HOMA and insulin resistance.
Table III, Table IV and Table V show the final separate models, and in which the components of each of the three criteria used for MetS were not included. These models were adjusted for age, and shows that both, biological and demographic variables such as fat mass and HOMA, and schooling, socioeconomic status, and physical activity level, respectively were the best predictors of MetS defined by the ATP III, AHA/NHLBI and IDF criteria. The OR for each predictor of the different criteria is depicted in the Table III, Table IV and Table V.
Table III Association between MetS defined by the 2001 NECP ATP III criteria as dependent variable and fat mass and demographic variables as risk factors

Stepwise backward using logistic regression analysis using MetS as the dependent variable. The model was age-adjusted. SES: socioeconomic status; OR: odds ratio; SE: standard error; CI: confidence intervals.
Table IV Association between MetS defined by 2005 AHA/NHLBI criteria as dependent variable and fat mass and demographic variables as risk factors

Stepwise backward by logistic regression analysis using MetS as the dependent variable. The model was age-adjusted. PAL: physical activity level; SES: socioeconomic status; OR: odds ratio; SE: standard error; CI: confidence intervals.
Table V Association between MetS defined by 2009 IDF criteria as dependent variable
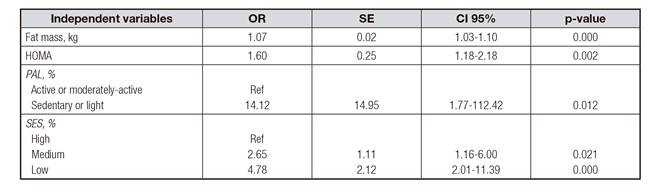
Stepwise backward by logistic regression analysis using MetS as the dependent variable. The model was age-adjusted. HOMA: homeostasis model assessment; PAL: physical activity level; SES: socio-economic status. OR: odds ratio; SE: standard error; CI: confidence intervals.
DISCUSSION
The prevalence of MetS in this Mexican aged group is high, and varies widely according to the diagnostic criteria used (p = 0.0001), with the 2009 IDF standards generating the highest prevalence. Similar findings have been reported by studies carried out in some Latin American countries with older people 5,6,21. This could be explained largely by the high proportion of obesity, especially central obesity, in this age group. In fact, recent evidence underscores that older obese people with MetS have more abdominal visceral fat, but less subcutaneous thigh fat than older obese people without this condition 37. To our knowledge, few studies have explored cardio-metabolic, body composition, inflammatory and demographic variables as the main the determinants of MetS in older people in a developing country. Our results show that this high prevalence is strongly and consistently associated with fat mass as direct marker of adiposity in this age group. It is important to note that, aside from fat mass and HOMA, only some sociodemographic variables assessed in this study were found to be mainly determinants of the high prevalence of MetS. Therefore, our findings are important and may help define specific lifestyle and demographic strategies for preventing MetS in this vulnerable age group as evidence of the association between MetS and cardiovascular mortality in older adult population continues to accumulate 11,12,13.
At the national level, the prevalence of MetS in older people is relatively high in Mexico. The 2012 National Health and Nutrition Survey (2012 ENSANUT for its initials in Spanish) reported a prevalence of MetS of 56.3% using the ATP III criteria, 60.8% according to the AHA/NHLBI's definition, and 67.9% by the IDF criteria 24. The prevalence found in this non-representative sample is lower (36%, 45% and 52% according to the ATP III, AHA/NHLBI, and 2009 IDF criteria, respectively), perhaps because our study excluded subjects diagnosed with type 2 diabetes by the 1977 ADA criteria 28, while the ENSANUT report included them. However, independently of the inclusion of diabetics, prevalence in this non-representative sample is high, indicating that greater attention must be paid to preventing this condition. Overall, prevalence of MetS in this age group is within the range reported for other, non-Latin American populations 3,4,7. Thus, it seems that the presence of MetS in older adult populations is relatively high regardless of genetic background, environmental exposures and the diagnostic criteria used.
Central obesity, hypertension and low-HDL-cholesterol were the most frequent criteria components found in subjects with MetS, and similar results have been reported by other studies in adults and older people 12,38. Central obesity was consistently the most prevalent factor identified by each set of criteria (87%, 87% and 99% by the ATP III, AHA/NHLBI, and 2009 IDF, respectively), followed, in second place, by hypertension (84%, 81% and 79% by the ATP III, AHA/NHLBI and 2009 IDF criteria, respectively), and then low HDL-cholesterol (87%, 75% and 72%, respectively). It is interesting to note that low HDL-cholesterol was the most prevalent component of abnormality found in a study of young and middle-aged Korean men and women 39. In our sample, the prevalence of central obesity, hypertension and low HDL-cholesterol were related to the increasing prevalence of MetS, which has been found to be relatively high among older age groups 40.
The regression analysis showed that most of the variables were determined to be significant predictors of MetS, but that some cardio-metabolic, body composition, inflammatory and demographic variables (including age, TASM, total cholesterol, LDL-cholesterol, CRP, interleukin-6, marital status, employment status, smoking, alcohol consumption, insulin resistance and chronic diseases) were not selected as predictors of MetS (Table II). It is important to note that several studies have shown a strong association between demographic variables and MetS in adult and fewer in older adult subjects 15,16,17,18,19,20,21. In fact, in this study we found a significant association between schooling or education level, socioeconomic status based on family income, and physical activity level with MetS, together with several biological factors as shown in Table I and Table II. In addition, multiple logistic regression results presented in Table III, Table IV and Table V show that high school or less; low SES and sedentary or light activities, together with fat mass and HOMA as independent variables were main determinants, regardless of the criteria used. Therefore, our results do support that fat mass as direct marker of adiposity and HOMA, and some demographic variables as the main determinants of the high prevalence of MetS. Other studies have reported a significant association between such variables as gender, socioeconomic status, educational level and marital status, among others, with MetS in adults 15,16 and older adult subjects 17,18,19,20,21.
Importantly, there are few studies in older people and the results are controversial about the association between SES, schooling and MetS, and fewer on the association between PAL and MetS 17,18,19,20,21,41,42. These three factors are important indicators of social status. The role of education level in the development of MetS is unclear nowadays. However, it has been reported that SES or income and education level can influence health behaviors, psychological distress, neighborhood characteristics, and access to health care 42. Regarding to the association between fat mass and MetS, some studies have shown a significant association; however, this component no added value over other markers of adiposity such as WC and BMI 43,44. In the elderly, adiposity particularly peripheral subcutaneous fat and trunk subcutaneous fat are associated with insulin resistance and this last one is one of the markers of MetS 45.
In accordance with the results of our multiple logistic regression analysis, it is clear that in addition to fat mass and HOMA, some demographic variables were main determinants of MetS in older subjects who may, therefore, be at high risk of cardiovascular morbidity and mortality. Of the total mortality recorded in Mexico in 2014 (633,000 deaths), 63.9% corresponded to people aged ≥ 60. Heart diseases (16.9%), cerebrovascular diseases (6.8%) and hypertension (4.7%) were the main contributing factors to all deaths that occurred in this population group (INEGI, 2014) 46. Therefore, we must give high priority to defining and implementing strategies to prevent MetS in this growing, older Mexican adult population.
The present study had some limitations. Firstly, all subjects included were free of type 2 diabetes, using the former criteria of 2 hour glucose value OGTT (fasting glucose ≥ 126 or ≥ 200 mg/dL at 2 h). Therefore, prevalence of MetS found is only valid for this particular sample. Second, HOMA to define insulin resistance and its associations could not be determined using the hyperinsulinemic-euglycemic clamp. However, it is well known that the method used in the present study correlated well with the hyperinsulinemic-euglycemic clamp. Additionally, the methods used for insulin determination in the three different mentioned studies varied in sensitivity. Third, this is a cross-sectional study, therefore only an association, not a causal relationship, is shown. Further studies in different settings are required to explore the effect of demographic variables as determinant of MetS in older people.
In conclusion, metabolic syndrome is highly prevalent in non-diabetic older adults and non-representative sample. In this study, the main determinants were fat mass and HOMA, and some demographic variables, mainly schooling, physical activity and SES. It is well-known that all these risk factors are potentially modifiable at general population. However, more research in other population on the interrelation between MetS and socioeconomic status and other demographic variables would provide additional evidence and allow us to identify other significant factors and to strength our results. At present, however, our findings support the importance of strengthening specific lifestyle strategies to prevent MetS in this vulnerable age group.

