










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Low physical activity and a sedentary lifestyle are related to increased risks for various diseases 1. However, the influence of physical activity and sedentary behavior on the biologically active, 1 , 25-dihydroxy vitamin D is not well defined 2. Several hypotheses have been proposed about the mechanisms for their biological effects 3,4,5-6. Bertrand et al. pointed out that physical activity had a strong effect on the 25-hydroxyvitamin D (25 [OH] D), where outdoor physical activity levels provide increased exposure to sunlight 7. Some association between physical activity and serum vitamin D level has been justified via such increased sun exposure during outdoor physical activities 8,9. Moreover, it has been stated that the physical activity may be related to increased serum vitamin D levels in a different unknown way 10,11. For example, it has been discussed that in sedentary lifestyle practices, the accumulation of fat mass results in decreased participation in outdoor activities, and adipose tissue may serve as a site for the sequestration of vitamin D. This can cause its trapping and yield for lower circulating levels of vitamin D biomarkers 3,12.
One of the proposed mechanisms for the association between vitamin D and some metabolic disorders is its postulated effect on the blood lipid profiles. However, there is no consensus in the literature for such relationship 10,13,14. It has been pointed out that with increasing 25 (OH) D levels, a decrease in body mass index (BMI) happens. BMI is associated with lipid profile 10,15. About 12-15% of studies in one meta-analysis have pointed to an inverse relationship between triglycerides (TG) and serum levels of 25 (OH) D 16. In addition, there are studies that have shown a positive correlation between vitamin D status and high-density lipoprotein (HDL) while reporting the inverse association of vitamin D status with low-density lipoprotein (LDL) 16,17,18-19. Moreover, the results from previous studies have shown a seasonal variation in concentrations of thyroid stimulating hormone (TSH) like vitamin D, which provides evidence for the link between vitamin D and serum TSH levels for changes in lipid profiles, since such seasonal variations have been previously reported for vitamin D 20,21,22.
To date, few attempts had been made to assess the relationship between the level of vitamin D in subjects with sedentary lifestyle behaviors and thyroid hormones, followed by changes in blood lipid profiles and their health risks. This study was aimed to investigate the relationship between serum vitamin D levels and circulating thyroid stimulating hormones, blood sugar, and lipid profiles among a sample of sedentary staff.
MATERIALS AND METHODS
PARTICIPANTS
The study population in this cross-sectional study consisted of 300 healthy staff aged 18-65 years with a sedentary lifestyle pattern from two different institutions (Development Bank and Institute for the Intellectual Development of Children and Young Adults), who were selected via random sampling. Among these participants, eligible individuals who were not pregnant, lactating or taking drugs that affect the lipid profile, calcium and bone metabolism were recruited. Individuals lacking chronic disorders such as liver and kidney insufficiencies, endocrinology disorders, anticonvulsive drug users, vitamin D, and calcium supplement users. All subjects were recruited during the winter of 2015. Anthropometric data including weight and height were obtained using a Seca(r) scale (Seca(r) 725; GmbH & Co., Hamburg, Germany) with a stadiometer, with participants wearing light clothes and no shoes. Weight and height were measured to the nearest 100 g and 0.5 cm, respectively. BMI was calculated.
BLOOD SAMPLING AND MEASUREMENTS
In order to obtain the clinical and laboratory data, a 10 ml peripheral blood sample was drawn after overnight fasting. Blood samples were centrifuged at 3,000 rpm for ten minutes and stored at -20 °C. A serum level of 25 (OH) D was measured using the direct competitive immune assay kit (Diasercine Italian Company, Monza, Italy). Serum levels of TSH were measured using a Radio-Immuno Assay kit (CIS Bionic(r) international, France). The levels of free T3 (triiodothyronine) and free T4 (thyroxine) were measured using a direct chemiluminescent immunoassay (Siemens Healthcare Diagnostics Inc., Berlin, Germany) kit. Fasting blood sugar was measured using the glucose oxidase method via Pars Azmoon kit (Pars Azmoon Co., Tehran, Iran). Plasma total cholesterol, HDL and triglyceride concentrations were measured in two consecutive different times using enzymatic kits, standardized reagents (Bionic(r) International, France). LDL concentration was calculated based on the Friedewald equation. A 25(OH) D level less than 20 ng/ml was considered as vitamin D deficiency, levels from 20 to 29.99 were considered as insufficient, and levels ≥ 30 ng/ml were considered as sufficient.
PHYSICAL ACTIVITY ASSESSMENT
A researcher-made questionnaire with different questions was used to assess the level of physical activity (Fig. 1). For the design of the questionnaire, some questions about physical activity were designed based on the Leisure Time Exercise Questionnaire used in the study by Scragg and Camargo 4. Also, a one-day routine diary of physical activity was gathered from each participant for verification.

STATISTICAL ANALYSIS
All of the statistical analysis was conducted using the SPSS (Version 21.0 for Windows, SPSS, Inc., Chicago, IL, USA). Two-sided p values less than 0.05 were considered to indicate significant differences.
The values for quantitative parameters were expressed as the mean value and standard deviation (SD), whereas the qualitative data were presented as numbers and percentages. One-way ANOVA and the Tukey's post hoc test were used to identify the significant differences between the groups based on fasting blood sugar (FBS), total cholesterol, LDL, HDL, and triglycerides. Bivariate correlation analysis was used for testing the correlation status between each of the mentioned lipid profiles and vitamin D levels. Multiple linear regression analysis was performed to determine the association between vitamin D levels and the predicted serum lipid levels, after stepwise adjustment based on age, gender, BMI, and physical activity.
ETHICS STATEMENT
This study was approved by the Ethics Committee and the Institutional Review Board of Urmia University of Medical Sciences (IR.umsu.rec.1395.165). The board waived the need for informed consent, as the subjects' records and information were anonymous and de-identified prior to the analysis. All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and national research committee, and with the 1964 Declaration of Helsinki and ethical standards.
RESULTS
Our results demonstrated that the prevalence of vitamin D deficiency was 65.7%; vitamin D insufficiency and sufficiency was 18.6% and 15.7%, respectively. Table 1 presents detailed information about deficiency prevalence between the two genders. Participants were 209 (69.66%) men and 91 (30.33%) women. The mean serum levels of 25-hydroxyvitamin D and TSH in total population were 19.17 ± 11.72 ng/ml and 1.94 ± 1.91 µIU/ml, respectively. The mean BMI was 25.63 ± 10.25. The average age of participants in the study group was 36.69 ± 7.14 years. Sample population stratification by 25(OH) D levels as deficient, insufficient and sufficient showed that mean 25(OH) D levels for each group was 12.74 ± 4.03, 23.24 ± 2.44, and 41.28 ± 10.94 ng/ml, respectively. Results from statistical analysis for comparing the three subgroups based on basic demographic variables showed no significant differences, except for serum vitamin D.

Results from ANOVA for comparing the means between the three groups showed that there were significant differences based on TG (F; 3.97, p = 0.02), HDL (F; 8.71, p < 0.001), and T4 (F; 8.88, p < 0.001). In comparison with the sufficient group, the deficient group had higher cholesterol, but in a statistically non-significant amount (F; 0.21, p = 0.80). The highest TG, T3, and T4 were seen in the deficient group. The insufficient group showed the highest HDL and lowest LDL values. The lowest triglyceride level was observed in the insufficiency group. Data revealed that the serum levels of 25(OH) D had an inverse but not significant association with LDL (F; 0.73, p = 0.47) and had a positive correlation with HDL (r = 0.20, p < 0.001). There was the highest LDL level and the lowest amount in the insufficient group. Meanwhile, the highest FBS and TSH in normal range values were seen in the vitamin D sufficient group (Table 2).
Table II. Results from the one-way ANOVA and t-test for comparing means between groups with different levels of vitamin D status
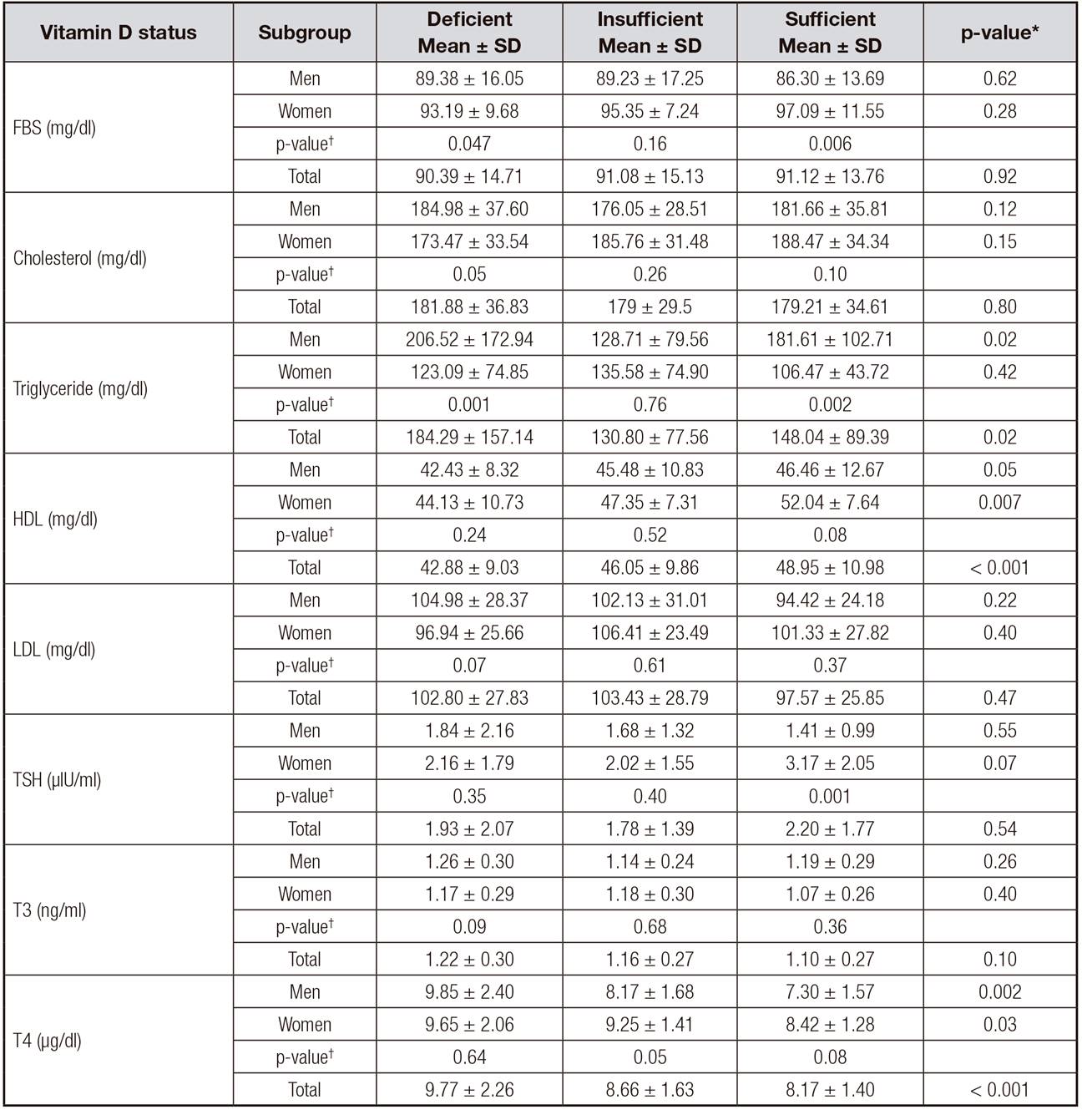
*One way ANOVA.
†Independent sample t-test.
The correlation analysis showed that among lipid profile fractions, just HDL had a significant correlation with serum vitamin D level (r = 0.2, p < 0.001). There was no significant correlation between LDL and vitamin D (r = 0.01, p = 0.81). Among the evaluated correlation for TG (r = -0.11, p < 0.04), T3 (r = -0.14, p = 0.04) and T4 (r = -0.29, p < 0.001), there was just a negative significant correlation for T3 with vitamin D. Figure 2 and Figure 3 show the results of different correlation analyses among all participants. Moreover, a significant negative correlation between LDL and T4 was observed (r = -0.22, p = 0.002).
The results of the linear regression analysis showed that after adjustment for gender and age, there was a significant association between the 25 hydroxyvitamin D concentrations with HDL and T4. This means that with 10 ng/ml increasing units in 25 hydroxyvitamin D concentrations, a 1.77 mg/dl increase in HDL and 0.51 µIU/ml decrease in T4 concentration can be expected within normal reference ranges.

Figure 2. Correlation between 25 (OH) D level and different fractions of serum lipids and glucose. A. Correlation between 25 (OH) D level and fasting blood sugar level (r = 0.07, p = 0.20). B. Correlation between 25 (OH) D level and cholesterol level (r = 0.01, p = 0.79). C. Correlation between 25 (OH) D level and triglyceride level (r = -0.11, p = 0.04). D. Correlation between 25 (OH) D level and HDL level (r = 0.2, p < 0.001). E. Correlation between 25 (OH) D level and LDL level (r = 0.01, p = 0.81). F. Correlation between 25 (OH) D level and TSH level (r = -0.04, p = 0.44).

DISCUSSION
There are controversies regarding the factors that could provide sufficient levels of vitamin D. Low physical activity and a sedentary lifestyle are related to increased risks for various diseases such as cardiovascular disorders, diabetes mellitus, hypertension, cancer, and multiple sclerosis. It has been proposed that most of these effects can be explained by the postulated effect of vitamin D on blood lipid profiles. Some previous studies have implicated that, in most instances, people with low physical activity have higher weight and less physical activity that results in reduced sun exposure 1, but some studies such as Jerome et al. have shown lower vitamin D level in subjects with higher physical activity level 2. Some reasons for such results can be related to the fact that students are mostly engaged in indoor activities.
The present study investigated the relationship between vitamin D status and lipid profiles in healthy subjects with a low level of activity and vitamin D deficiency. Vitamin D deficiency was observed in 65.7% of the studied subjects.
The mean serum vitamin D in the total studied population was 19.17 ± 11.72 ng/ml. This amount is higher in comparison with that of other studies 7 that were conducted on subjects with light physical activity level or a sedentary lifestyle, and lower than the amount observed in some others such as the study by Hibler EA et al. 1. The highest FBS in the normal range values were seen in the sufficient vitamin D group, but with no significant differences between groups. In this study, the correlation analysis showed no significant correlation between vitamin D level and FBS, while in other studies low 25 (OH) D levels have been associated with higher plasma glucose 19. Serum vitamin D levels have been inversely related to fasting glucose and insulin 10. In a similar study, no significant difference was proposed based on the different levels of vitamin D 23. Theoretically, several mechanisms have been proposed to explain the relationship between vitamin D and blood sugar via both genomic and non-genomic pathways, with its role in pancreatic beta cell function 18,19,24. Vitamin D receptors are present in pancreatic B-cells and skeletal muscles, which demonstrated that vitamin D can enhance insulin responsiveness for glucose transport 19.
There are various previous studies with different results regarding the vitamin D status effect on the blood lipid profiles 17,18,19,25. Direct and indirect effects of vitamin D to modify the lipid profile have been proposed. Vitamin D may decrease the TG serum levels through its regulatory action by increasing the lipoprotein lipase activity in adipose tissue 26. Additionally, its effect on the serum levels of total cholesterol and LDL may be mediated by its decreasing effect on the absorption of fat, particularly saturated fatty acids 27. Also, it has been suggested that it can be mediated via calcium, which increases the conversion of cholesterol to bile acids 18.
In the present study, a comparison based on the mean TG between the three groups showed significant differences plus a relatively significant inverse correlation with serum vitamin D concentration (r = -0.112, p = 0.055). Lower TG levels accompanied higher serum vitamin D levels. These results are in accordance with the results from several previous studies that indicated an inverse correlation between vitamin D and TG. In some previous studies such as those of Ponda et al. 17 and Kelishadi et al. 16, similar results have been reported. There are few studies reporting no relationship between vitamin D status and serum TG levels 23,28.
Regarding the effect of vitamin D on HDL, Karhapa et al. 25 and other cross-sectional 10,12 and trial studies 23,28 have postulated that there is no association between 25 (OH) D levels and HDL, while other studies have proposed a positive association between vitamin D status and HDL. In some trial studies 29,30, an increase in HDL with vitamin D supplementation has been mentioned. In the current study, a positive and direct correlation between serum levels of 25 (OH) D and HDL was observed. Reviewing the previous literature revealed that some of the above relationships might be explained by the necessity of vitamin D presence for maintaining the adequate levels of apolipoprotein A-1, the main component of high-density lipoprotein 31.
The results of the present study counteract the findings of many others 17,25,28 with regard to the possible association between vitamin D status and LDL levels, as our results showed no significant association between vitamin D and LDL. The highest LDL level was in the insufficient group and the lowest amount was in the sufficient group, but no significant differences were observed. Karhapaa et al. 25, who included in their study 909 healthy males between 45-70 years of age, found an inverse association between 25-hydroxyvitamin D and LDL, alongside with a lack of association between 1,25-hydroxyvitamin D and LDL.
In different studies, a positive relationship between TSH and lipid profiles has been discussed and it has been stated that such relation can predispose subjects to develop different types of diseases that are mediated by obesity. The positive correlation between weight gain and a progressive increase in serum TSH and elevated TSH levels in obesity over a 5-year period has been reported 24. Our study confirms the results of previous studies, which showed a positive inverse relationship between vitamin D and thyroid hormones, because vitamin D deficiency and lower serum levels of 1, 25-hydroxy vitamin D were accompanied by higher levels of T3 and T4, with a significant difference for T4. This study, unlike that of Barchetta 20, which pointed out a central action for the active form of vitamin D on TSH secretion, showed no significant association between vitamin D and TSH.
There were some limitations in our study. First, the cross-sectional design of the study. Second, no data about the dietary intake levels of participants has been gathered. Third, all participants were subjects with a sedentary lifestyle and there were no comparable groups with other levels of physical activity.
CONCLUSION
Our results showed improvements in lipid profile fractions and thyroid hormones secretion, such as a decrease in the levels of TG, T3, and T4, and increments in HDL with favorable serum vitamin D status. The detection of causal relations needs the design of a well-controlled intervention or cohort studies to provide benchmark evidence. The biochemical and physiological mechanisms, as well as molecular and genetic pathways for verification, will be as well an area for further research.

