










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkCLINICAL DESCRIPTION
48 year old male with social difficulties, admitted into prison.
Refers that he has been operated on for cancer of the colon nine months ago, and since then has not attended any medical check by specialists (oncology or surgery). The patient is homeless although he does receive some family support.
Drug user and undergoing replacement therapy with methadone. Was an intravenous drug user (IDU). There are no other personal details of interest.
Presented a stoma prolapse of more than 15 cm length and over 25 cm perimeter (Figures 1 and 2) at the base. No signs of infectious process or progression of the cancer, apart from caquexia.


EVOLUTION
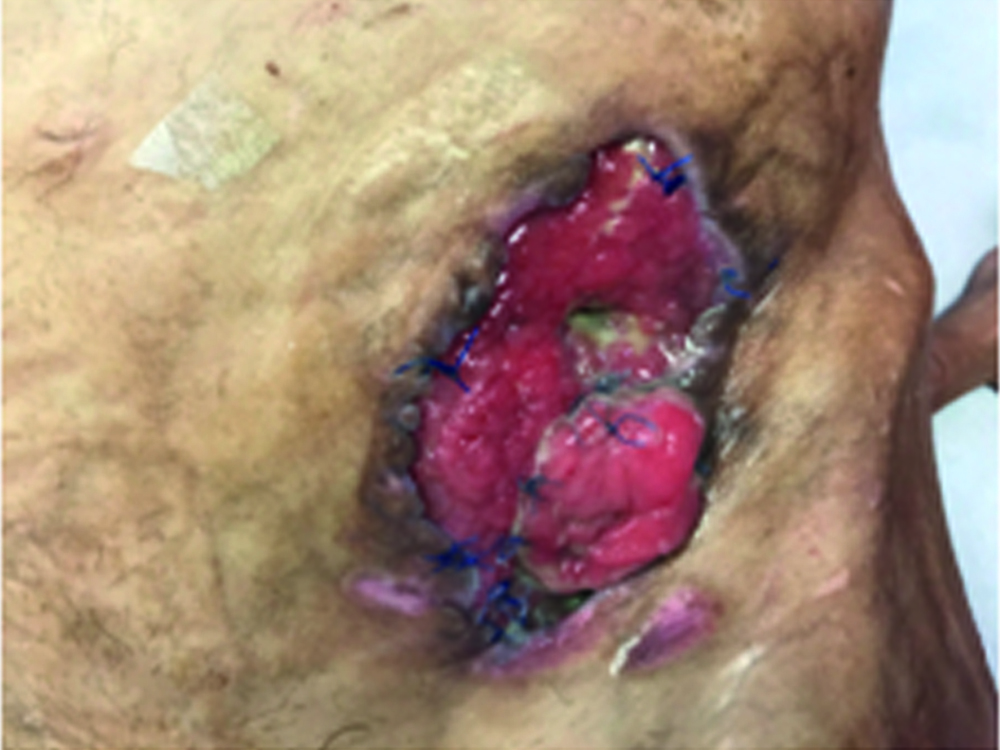
Cross-consultation was requested with surgery, and an intervention via local approach was carried out, the stoma was freed from the abdominal wall, the redundant intestine was removed and the stoma was reshaped (Figures 3 and 4).

The studies showed that there was a progression of the cancer with liver metastasis. The patient was released after applying article 196 of the Prison Regulations.
He entered prison in a generally bad state and underweight, with a body mass index (BMI) of 18.
COMMENTS
A prolapse is a late complication of colostomíes, and is defined as the protrusion of the stoma above the abdominal surface. It is a rare complication (2-10%), the frequency of which varies according to the location of the stoma, and if more common in ileostomies and loop colostomies, and less in terminal colostomies.
The origins of a prolapse are unclear and depend on a lot of factors. Possible causes include constipation, mismatch between the size of the intestine and the hole made in the abdominal wall and the existence of long, mobile intestinal loops.
Recurrence is frequent.

