










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Cannabis use tends to be more prevalent among the imprisoned population than in the general population. Specifically, in Spain the prevalence of use in the last 30 days for the general population is 9.1%1,while among inmates it is 19.4%2. The prevalence among this population when not in prison increases to 37.8%2. Thus, cannabis use is quite prevalent among those who are or have been imprisoned.
Although the recreational use of cannabis has been related to psychopathology and neuropsychological dysfunctions, its medical properties are gradually being recognized3, resulting in several countries and American states implementing scaled-up medical cannabis laws. The indications of medical cannabis include psychological issues such as anxiety, post-traumatic stress disorder (PTSD), and decreased psychological alertness and arousal, which are highly prevalent conditions among the imprisoned population4. However, anxiety as a symptom, which is also highly prevalent in stressing situations including being imprisoned, should be appropriately distinguished and the lack of evidence for using cannabis in this case should be considered. The medical use of cannabis is also being explored for the treatment of schizophrenia5 or drug and alcohol dependence6, where mixed results have been obtained. The appropriate dosages and proportion of cannabinoids in combined formulas should be elucidated in further studies5. At the same time, it should be noted that the indications for which the regulatory agencies approved the available cannabis-based medications were treatment of spasticity in multiple sclerosis (nabiximols), seizures occurring in Lennox-Gastaut and Dravet syndromes (epidiolex), and side effects associated with chemotherapy (nabilone). Cannabis use in prisons has been negatively correlated with perceived social support7,8. One qualitative study found that both inmates and prison staff used cannabis to better cope with prison life. Cannabis is also used for stress relief, as a sleep aid, and to prevent violence9. Some of these benefits, mostly related to anxiety disorders, have also been found when nabilone, a synthetic form of THC (tetrahydrocannabinol), was administered to male inmates with serious mental illness10.
Considering the objectives of this study, the harm reduction approach should be used when interpreting the findings. The harm reduction paradigm is based on the pragmatic goal of reducing the direct and indirect negative effects of drug use. This paradigm emphasizes the role of all the actors involved in drug use. Thus, a cooperation between different subjects, and the subsequent communal and social articulation, would be necessary to protect both human rights and the health of consumers11.
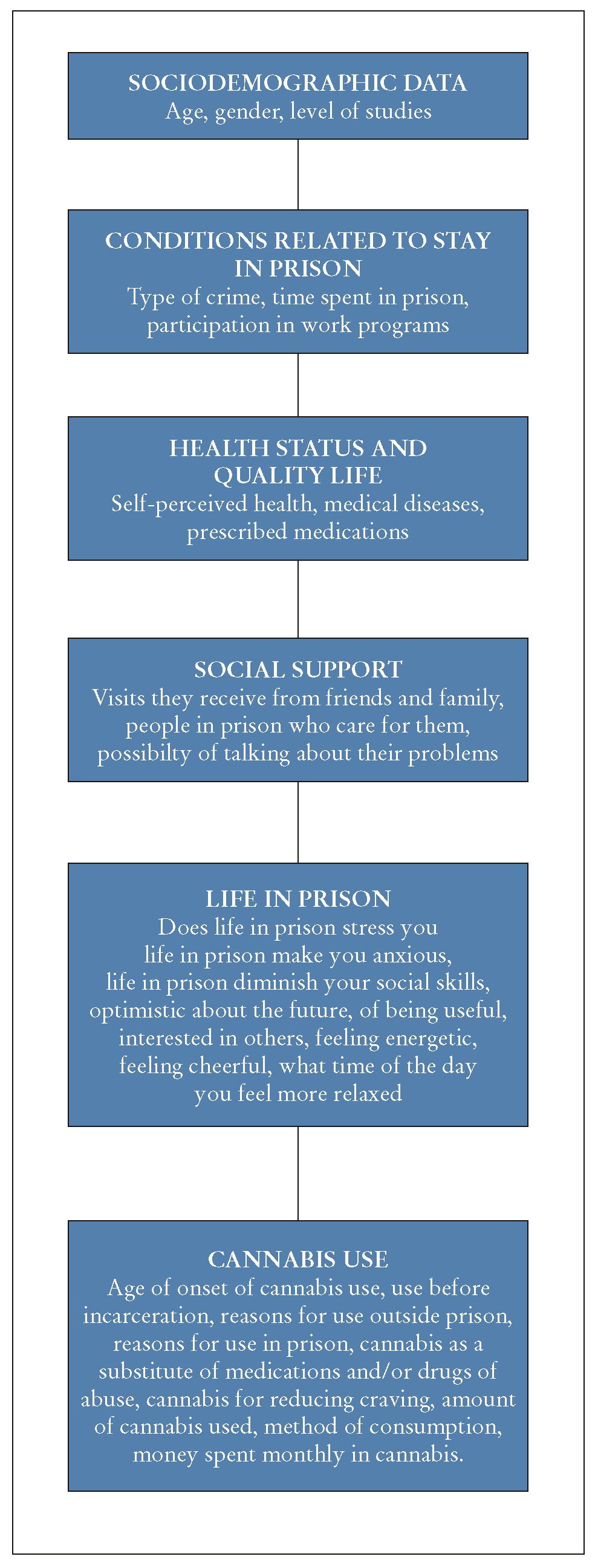
In this study, we administered a survey assessing quality of life, perceived social support, prison life, and cannabis use among a sample inmates in Spanish prisons.
Materials and methods
Research was carried out at the Drug Dependence Service of two prisons: Brians 1 (CP_B1) and Brians 2 (CP_B2), both located in Catalonia, Spain. Brians 1, a gender-mixed prison, holds 197 women and 1036 men, while at Brians 2 1504 men live in 14 residential modules. The Drug Dependence Service offers a program that trains inmates as health agents. This study had two phases: in phase 1, we organized a group discussion involving health agents in training, to discuss the use of cannabis in prison. Discussion results informed the design of the questionnaire used in phase 2, which assessed quality of life, perceived social support, prison life, and reasons for cannabis use. The questionnaire, prepared in line with health indicators contained in the Catalan Health Survey12, was administered by two of the authors.
Statistical analysis
Descriptive statistics were used to describe results, while a linear regression analysis was performed with the variable "subjective health status" as a factor (Figure 1).
Results and discussion
Sociodemographics
The main topics in the group discussion (n=14; phase 1) are included in Table 1. The questionnaire (phase 2) was administered through one-on-one meetings with 63 subjects who reported cannabis use, mostly involving hashish. The sample was 6.3% women, a percentage similar to that in Spain's prison population (6.8% females; ESDIP, 2016). The mean age was 37.5 years old (range 20-55). The level of education was 3.2% illiterate, 6.3% vocational training, 4.8% baccalaureate, 33.3% high school, and 52.4% basic education. Only 4.7% of subjects were imprisoned for the first time.
Table 1. Main points extracted from a group session (n= 14) that took place in the Phase I of the project, at Brians' drug dependence service, 2015-2016.
| Cannabis in prison | ||
|---|---|---|
| Main points made by imates regarding cannabis use | Advantages of using cannabis | Disadvantages of using cannabis |
| In prison, cannabis is used more than other drugs | Cannabis use relaxes | Difficulties to get cannabis |
| Inmates use cannabis for not taking prescribed medications | Stimulates the appetite | Possible debt |
| Cannabis is considered as a medication | Relieves the stress | Worrisome |
| Using cannabis helps to not take harder drugs | Time goes faster | Fear of losing control |
| You have to be careful. If you abuse, you may become addicted | It helps with overthinking | Memory hampered |
| For some people, cannabis is sacred | Relieve sadness | Anxiety |
| It is not necessary to smoke daily, you need to establish some limits | You can avoid harder drugs | Aggressiveness |
| Smoking regularly can cause some diseases | You smoke less tobacco | Disrespect |
| Smoking in plastic dirty bottles or in pens is also harmful for your throat and lungs | It helps you to get to sleep | Bad mood |
| Cannabis use is not associated with physical withdrawal syndrome, but it can generate psychological dependence | It allows you to take less medication | Low self-esteem |
| You must take care in case you need to drive or work. Cannabis affects your attention | Paranoia; Criticisms, hate, anger; Dry mouth; Respiratory issues; Difficulties in concentration; Tiredness and confusion | |
Conditions related to stay in prison
Regarding the types of crimes, 50.8% were in prison for robbery or theft, 22.2% for violent crimes (injuries, homicides, attempted murder, attack on authority, gender violence), 23.7% for miscellaneous other crimes and, finally, 3.2% of subjects were serving sentences for crimes against public health (drug trafficking).
Regarding the length of time participants had been imprisoned, the average was 64.7 months (M= 48 months; SD= 50.2), which could be for a single crime or multiple sentences.
Finally, 90.5% of the sample reported participating in at least one prison work program. Among the 38.1% of subjects who participated in addiction-treatment programs, 14.2% attended for relapse prevention and 14.3% for heroin cessation, which includes methadone maintenance.
Perceived health and quality of life
Regarding perceived health, 22.2% of subjects reported having "very good health", 46% "good", 20.6% "fair", 9.5% "bad", and 1.6% "very bad". Among the sample, 47.6% of subjects reported having at least one medical disease. Prescribed medications were regularly taken by 76% of subjects; while 28.4% of subjects without a medical condition also used medication regularly. The medications prescribed most frequently were benzodiazepines and analgesics: clorazepate (17.4%), clonazepam (14.2%), alprazolam (9.5%), diazepam (9.5%), methadone (4.7%), sinogan (4.7%), tramadol (3.1%), Ventolin (3.1%), suboxone (1.6%) and aspirin (1.6%).
Social support
For the item "visits they receive from friends and family", 42.9% of participants reported insufficient, 33.3% sufficient, and 23.8% considerable visits. Regarding having other persons inside the prison who care for them, 31.7% of subjects reported insufficient, 41.3% sufficient, and 27% considerable care. Regarding opportunities to speak with someone about their problems, 25.4% of participants reported insufficient, 50.8% sufficient, and 23.8% considerable opportunities.
Prison life
Subjects answered a series of questions regarding their adaptation to prison life. The answers are detailed in table 2. While most subjects answered that life in prison is stressful and was causing them anxiety, a majority of subjects also answered that they felt mostly optimistic about their future or that they had feelings of usefulness. Another item related to prison life asked, "At what time of the day do you feel more relaxed?" The most frequent answer was "when in the cell after the count" (55.5%), followed by "during educational activities" (9.5%), "at any moment" (8%), "when working" (7%), and "when in the prison yard" (1.6%).
Cannabis use
The mean age of onset of cannabis use was 14.4 years (SD= 6). Only 7.9% of inmates had not used cannabis before entering prison. Reasons for commencing cannabis use were recreational (93.7%) and medicinal (6.3%). Reasons for current cannabis use included relaxing (77.8%), mood improvement (57.1%), anxiolytic purposes (50.8%), to treat insomnia (49.2%), appetite stimulation (38.1%), and pain relief (3.2%).
About half of the participants (49.2%) reported using cannabis as a substitute for other medications, including benzodiazepines (20.6%), antipsychotics (6.3%), hypnotics/sedatives (3.1%), antidepressants (1.6%), and methadone (1.6%). When asked if they used cannabis as a substitute for illegal drugs, again 49.2% answered affirmatively. These illegal drugs included heroin (15.8%), cocaine (8%), MDMA or ecstasy (8%), alcohol (6.3%), amphetamines (1.6%), tobacco (1.6%), and LSD (1.6%).
Cannabis was also reported by 58.7% of the sample to reduce their craving for other drugs, and 65.1% reported using it in addition to other drugs, where it helped them to reduce their consumption of other drugs. The amount of cannabis consumed was around 3 joints per day, on average (M= 2.97, SD= 4.13). Joints were the most commonly used method of consumption (44.4%), but since rolling papers are forbidden in Catalonia prisons, subjects also use other methods, such as a "bottle" (31.7%) or "pen" (3.1%). Finally, the average of money spent per month on cannabis was 81.9 euros (SD= 99.5).
Linear regression model
A linear regression model was built with self-perceived health as a factor. Numerous independent variables were introduced. The model found that only the number of visits received was a predictor (R2= .46, β= -.34, t(7)= -2,38, p= .02), where subjects who reported receiving more visits also showed a better health status.
Discussion
This study presents, for the first time, the characteristics of a sample of inmates in Spanish prisons who use cannabis. Although most of them started to use cannabis for recreational purposes before entering prison, once in prison the reported reason was mainly to cope with the stress associated with prison life. Other reasons included the substitution of prescription medicines and illegal drugs, as well as associated cravings. All of these uses have been reported in the literature as common among non-incarcerated populations13,14.
The perceived social support of the sample was low. This variable tends to be inversely correlated with stress and substance use.8 Among 70% of our sample, self-reported levels of anxiety and stress were "a lot" and "extremely." Although our sample had poor rates in terms of feeling cheerful, being interested in others, and feeling useful, almost 80% felt "very" and "extremely" optimistic regarding their future. In the regression analysis, none of the variables related to either cannabis use or prison activities were associated with self-reported health status. Remarkably, the only variable that was considered a predictor of health status was the visits received from friends and relatives. This reinforces the well-known idea that social support is essential for mental health and well-being in the prison context15.
Research on cannabis use in the prison context is scarce, although previous research has found similar results regarding both psychological benefits (in terms of coping with prison-related stress) and its role as a substitute for other drugs and prescription medicines, and thus enhancing its role in harm reduction strategies9. Like Ritter et al.9, we failed to find reports of withdrawal symptoms or cravings among cannabis users. Our subjects smoked 3 joints per day, which seems to not be a problematic pattern of abuse and is below the mean use for medical users in Europe.16 Although more than half of our sample had a medical condition, it would be difficult to say whether the cannabis use observed was medicinal or therapeutic. In fact, the main purpose seems to be to better cope with the effects of incarceration, which suggests use could be considered a self-care practice with the goal of improving quality of life, akin to therapeutic users in the general population.17 Notably, due to the prohibition on rolling papers in Catalan prisons, inmates have to use alternative and more harmful methods, involving plastic bottles and pens, and therefore expose themselves to health risks. Again, from the paradigm of harm reduction, basic strategies improving the safety of drug use should be facilitated. For instance, it would be advisable to allow rolling papers in order to reduce the potential harms associated with cannabis use. Finally, some potential limitations regarding the sample should be mentioned, since it was recruited via contacts that the health agents provided rather than random selection. Notably, the percentage of inmates serving sentences related to harm to public health (drug trafficking) was very low (3.2%), whereas among the general Spanish incarcerated population this percentage is 25.2%.2 The questionnaire was administered to different wards with varying rates of participation, so it is challenging to know what extent our results can be generalized.
Conclusion
Further research is needed in order to explore whether cannabis use in prison has benefits or not, not only for specific symptoms but also in terms of reducing the stress associated with the institution.9 These results warrant further research that might support a serious consideration of harm reduction programs or even pilot programs of cannabis dispensation inside prisons. Those pilot programs should compare the potential benefits/detriments of other drugs and use standardized measures of quality of life and other variables. This proposal could be better framed in Spain if cannabis were finally regulated, as is currently being proposed by some political parties. It is clear that better forms of using cannabis, for example allowing rolling papers inside prison, should be implemented.

