










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
4904608
Clinical measurement of joint range of motion (ROM) has been a fundamental and essential evaluation in various health speciality, predominately physiotherapy. Its history can date back to the 1920-1930s [1]. Up to now, goniometry measurement for ROM is an everyday practice for physiotherapists as well as other healthcare professionals. To advance the ROM measurement, a new approach of using accelerometers and gyroscopes to facilitate ROM measurement has been intensively investigated in the last decade [2, 3].
An accelerometer is a force sensor that senses linear acceleration along with single or multiple directions. The operation principle is based on a mechanical sensing element that includes a proof mass attached to a mechanical suspension system. Following Newton's Second Law of Motion, the inertial force produced by gravity or acceleration causes the proof mass to deflect. This acceleration of the proof mass is quantified electrically [4]. A gyroscope detects angular motion about one or more axes. It operates on the mechanism of sensing an induced Coriolis acceleration on the proof mass causing vibration along a direction orthogonal to the axis about which the rotation is applied [5].
In recent years, there is a noticeably growing trend in the use of telerehabilitation. With the use of mobile sensors, patients' physical status can be monitored remotely in the real world and in real-time [6], which increases efficiency and reduces the cost of rehabilitation services. Consequently, a reduction in healthcare disparities can be achieved. As the tele-rehabilitation system becomes more popular, biomedical engineers develop more variety of wearable sensors to facilitate the monitoring of patients' condition. Therefore, it is necessary to test the reliability and validity of the mobile sensors to ensure the accuracy of the measurement.
This study was to test the test-retest reliability of the human upper limb joints ROM measurement using a set of wearable mobile sensors. Also, it was to find out the validity compare with goniometer measurement.
MATERIALS AND METHODS
PARTICIPANTS
The participants for this study were students and staff of the Singapore Institute of Technology (SIT). They were recruited by convenient sampling. The inclusion criteria were healthy males or females aged 18 years old or above, no physical impairments in the upper limbs. Individuals not fulfilling the inclusion criteria were excluded. Ethical approval was issued by the Institutional Review Board of the SIT (Approval number: 2018008). The study was conducted in Aug 2018 in the practical skill laboratory at the SIT and written informed consent was granted from the participants before the data collection.
INSTRUMENTS
The mobile sensor used in this study was a wearableREBEE (XCLR8 Technologies) movement detection system, which consists of a 10-axis inertial measurement unit including an accelerometer, a gyroscope and a magnetometer. The specifications of the sensor are as follows: (1) range parameters: Acceleration: 16g/s2; Gyro: 2000 deg/s; Bandwidth 20 Hz. (2) Data format: Quaternion data. (3) Communication parameters: Rate: 9600; Retrieval rate: 20 Hz. Two twelve-inch plastic BASELINE goniometers (Model 12-1000) were used in this experiment to compare the measurements with the sensors.
ACTIONS AND MEASUREMENTS
Four kinds of shoulder and elbow movements were studied for the measurement of ROM. Table 1 presents the details of these movements studied. These movements covered all the axis of movements in the shoulder and elbow and are functional in daily activities. The testing protocol followed the procedure described in Reese et al., 2016 [7]. The study was conducted at the exercise laboratory at SIT. During the data collection, the participants came into the laboratory and registered for the study. The investigators explained to the participants the purpose of the study. Participants who met the inclusion criteria of the study were invited to give their informed consents. The data was collected from participants individually. After recording their demographic information, the participant was randomly assigned to either the left limb or the right limb ROM measurement groups.
The investigators took the participant to the measuring station. The participants were instructed to lie in the supine position on the examination plinth. The sensors were placed in two regions in the upper arm and wrist to measure the joints ROM (Table 1). The two regions were selected because they are the most distal parts of the upper and lower arms with prominent bony landmarks. The sensors were stabilized on the testing limbs with elastic Velcro straps. The setup of the sensors was conducted by the two investigators (Team A) who have a background in engineering but were novice in healthcare and ROM knowledge. These two investigators also recorded the degrees of ROM readings from the system. After putting on the sensors, the participants were instructed about the movements as stated in Table 1. The participants were told to perform three to five repetitions of each movement as warm-up before the actual data recording. The participants were also instructed to perform each movement as far as possible and move the testing limb back to the starting position after the investigators took the readings from the sensors and the goniometers. Each of the four movements was repeated twice.
The control ROM measurements with the goniometers were taken by another two investigators (Team B) who were third-year students of a BSc. (Hons) Physiotherapy programme. They were supervised by two instructors who each had over ten years of clinical experience. The two investigators in Team A recorded the readings of the sensors for the angles of each of the four limb movements in degrees while the other two investigators in Team B conducted the goniometric measurements. Both sensors and goniometric measurements were conducted concurrently for each of the four movements studied. Still, all four investigators in both teams recorded the reading separately and were blinded from each other's readings.
STATISTICS
All data were analyzed with IBM SPSS 23 for Windows (IBM Corp., Armonk, NY, USA). Intraclass correlation coefficients (ICCs) and 95% confidence intervals (CIs) were computed to determine the test-retest reliability of the measurements. Pearson correlation coefficient (r) was calculated from the data between the sensors and goniometers to establish the ICCs and construct validity. Bland-Altman plots were generated to illustrate the 95% mean difference between the two measurements.
RESULTS
Thirty-four asymptomatic young Asian adults participated in this study and 15 of them were males. The average age of the participants was 24.2 ± 3.82 (mean ± standard deviation) years old. The average height and weight were 165.9 ± 8.3 cm and 61.2 ±13.6 kg, respectively. Half (N= 17) of participants were tested with their left limb and the other half on the right limb. A total of 544 data points were collected from the sensors and goniometer (34 participants x 4 movements x 2 rep. x 2 measurements). Among these, seven data points were discarded due to technical errors in the measurements with either the sensors or the goniometers. These included 2 data points in elbow flexion, 2 data points in shoulder flexion, 2 data points in shoulder abduction and 1 data point in shoulder external rotation.
The test-retest reliability as indicated by ICC for the ROM measured by the sensors were between 0.94 and 0.99, p < 0.01; and for the goniometer measurements were between 0.95 and 0.98, p < 0.01 in the four movements (Table 2). The reliability was considered as excellent strength (> 0.90) in both measurements, according to Koo and Li [10]. Pearson's correlation between the sensor's ROM and goniometric data in four kinds of movements ranged from r = 0.96 to 0.99, p < 0.01, which explained 92% to 98% of variances indicating the correlation of these two measurements was very strong [11]. The Bland–Altman plots (Figure 1) illustrate that 95% of the differences in ROM measured by the sensors compared with the goniometers were from less than -10 deg to slightly more than 20 deg.
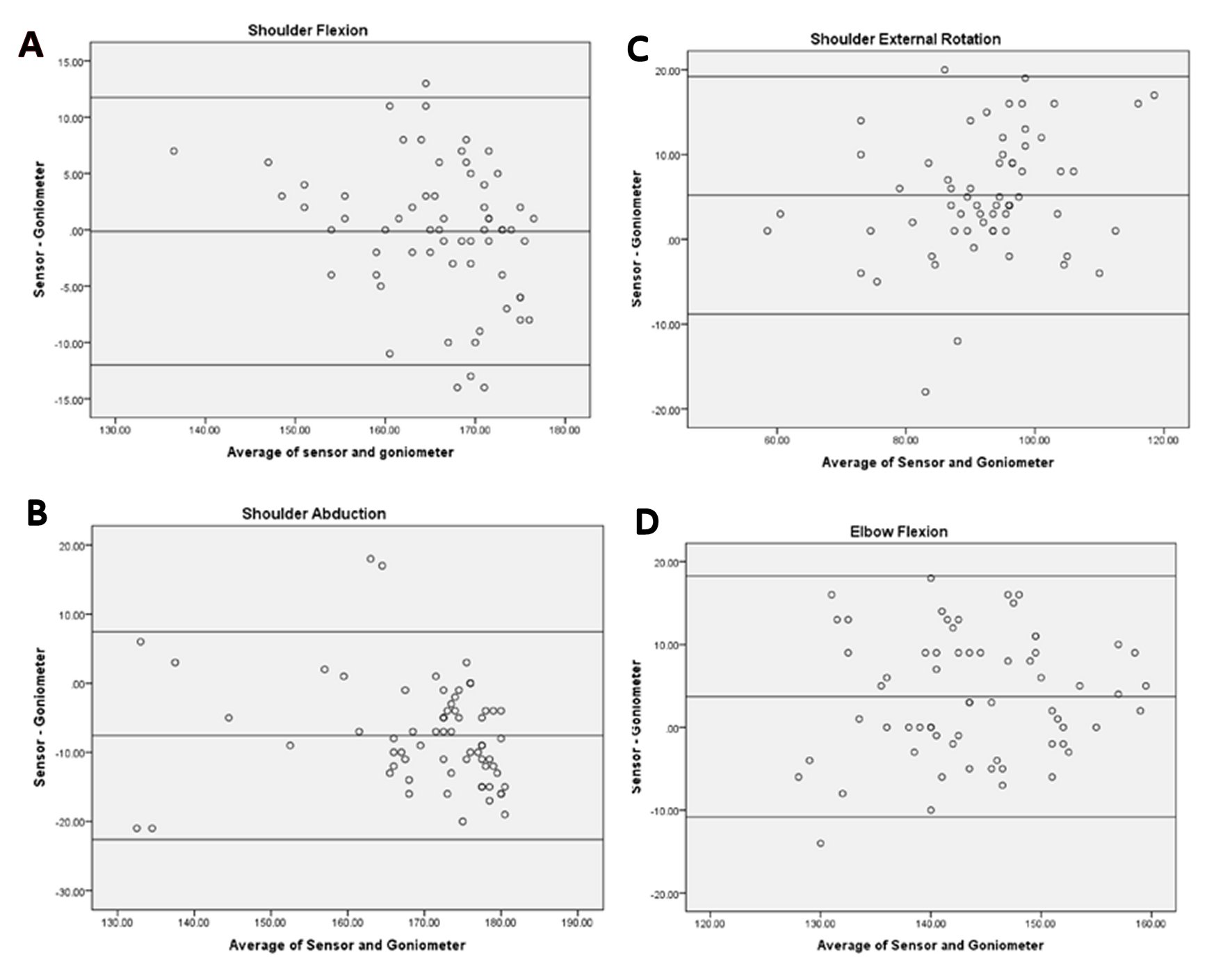
Figure 1. Bland-Altman plots of results of two measurements in shoulder flexio (A), shoulder abduction (B), shoulder external rotation (C) and elbow flexion (D).
Table 2. Reliability of the sensors and goniometer measurement and correlationThe reference ROM values of shoulder flexion, abduction, external rotation (in 90 deg abduction) and elbow flexion are 170.4, 184.5, 98.6 and 147.3 respectively for healthy individuals in the age group 20-40 years old [8, 9].
ICC = Intraclass correlation coefficient. * ICC2,1 with p<0.01. **r value with p<0.01
DISCUSSION
Movement measurements through accelerometers are not a novel idea. Several previous studies had been conducted to test for the accuracy of the measurement devices [12, 13]. In the current study, the specifications of the sensors and the measurement procedures were stated clearly, which allowed future studies to reproduce the procedures in further testing. With the advancement of ROM measurement technology, the findings of this study showed that investigators with no prior training in ROM measurement could use the mobile sensors and achieve highly reliable and valid ROM measurements compared to those of health professionals, which further indicated the practicability of this technology.
Similar to the previous studies of measuring joint angles using electronic sensors [2, 14], the mobile sensors used in this study demonstrated excellent test-retest reliability of upper limb ROM measurements. The measurements of upper limb ROM data between the sensors and goniometers in all four kinds of movements had a very strong correlation, which was especially noteworthy due to our effective blinding process in our measurement procedure. The mean difference between the two measurements and the Bland–Altman plots provide more specific ideas about the correlation. The ROM measurements of the sensors and the goniometer were concurrently but separately recorded by two teams of investigators who were not aware of the other team's readings. In addition, the team A investigators who operated the sensors were not trained in healthcare knowledge and therefore, they had no preconception of the sensor's ROM readings. It was previously proposed that the reliability of goniometry depends on the clinicians' experience [15, 16]. Therefore, our findings implied that novice investigators could operate the sensors properly and performed reliably with valid clinical ROM measurements. The mobile sensor system may allow non-healthcare trained family members to record clinically useful measurements for upper limb ROM for symptom monitoring when therapists were not present to tend for the patients.
The average values in all four kinds of ROM were close to the previously established normative ROM values of the shoulder joint from the same age group [8, 9], which provided support for the validity of our ROM data. The mean differences between the two ROM measurements for shoulder flexion and shoulder abduction were 0.13 degrees and 7.6 degrees respectively. The mean difference and 95% CI indicated that there was no statistically significant difference. The ROM of the elbow flexion and shoulder external rotation movements recorded by the sensors were statistically significantly higher than that of the goniometer, as indicated by the mean difference 95% CI (Table 2). Traditionally, goniometry is a gold standard for measuring shoulder ROM [17] but not for elbow ROM. Instead, the gold standard for elbow ROM is radiographic measurement [18]. However, we found that the correlations of the upper limb ROM measurements between the sensor and goniometer in all four kinds of movements were over 0.95 [18], indicating that the measurement of elbow ROM with goniometers is a valid method.
This study did not include lower limbs measurement for a few reasons. First of all, the ROM measurements recorded by the standardized procedures during lower limb movements such as knee flexion or single-leg raises were not as functional. Some clinicians and researchers would prefer taking the ROM of the lower limb in more functional ways, such as standing and walking [2, 19]. Secondly, the sensors were developed for telerehabilitation, for which the patients are supposed to put on the sensors and perform the actions themselves, or with assistance from non-healthcare trained people. Without the supervision of clinicians or researchers, the lower limb ROM measurements using the standard procedures are certainly inaccurate due to many possible measurement pitfalls [19, 20]. The measurement of lower limb ROM with the sensors using the standard procedures would be difficult for non-healthcare trained investigators to perform. Accordingly, the current study focused on establishing the reliability and validity of ROM measurements of the upper limb using the mobile sensors.
Convenient sampling is one of the limitations of this study. The current study recruited merely healthy and young participants; the generalizability of our results to different populations of participants would be limited.

