










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
Permalink1. INTRODUCTION
The coronavirus disease 2019 (COVID-19), which started in Wuhan, China, spread worldwide. This novel coronavirus had been named Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) by the International Virus Taxonomy Committee [1]. On February 11, 2020, the disease was officially named COVID-19 by the World Health Organization (WHO) [2]. According to WHO data, approximately 275 million cases and 5 million deaths had been reported until 3 January 2021- 22 December 2021 [3]. Mortality in COVID-19 is higher than seasonal flu, which has a generally less than 0.1% mortality rate. Smoking, chronic obstructive pulmonary disease (COPD), diabetes mellitus (DM), hypertension (HT), cardiovascular diseases (CVD) and a history of malignant findings are also the risk factors that increase mortality in COVID-19 [2, 3].
To this date, no drugs have been approved to treat or prevent COVID-19. All treatment is planned according to experience. In the treatment of COVID-19, antiviral treatments are used as well as immunosuppressive and immunomodulatory treatments [4]. Immune plasma (IP) IP is one of the immunomodulatory treatments used in the treatment of COVID-19, which is a passive antibody treatment and occurs against the virus in the blood of a person who has had COVID-19 infection, has been evaluated as a promising and potential treatment option since the beginning of the COVID-19 pandemic [5]. On March 24, 2020, the Food and Drug Administration (FDA) approved IP treatment for critical COVID-19 patients as long as their approval is obtained. IP has previously been shown to effectively treat H1N1, SARS, and MERS viruses [6]. According to the FDA, eligible IP recipients are COVID-19 positive patients with severe or life-threatening complications (Table 1). The life-threatening complications are considered to include pulmonary failure, septic shock, multiorgan failure, or dysfunction [7].
Table 1: Ministry of Health IP treatment updated guidelines [8, 9].
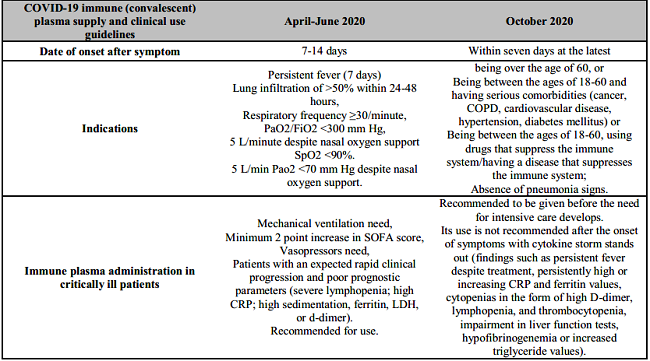
PaO2: Partial pressure of oxygen in arterial blood; FiO2: Fraction of inspired oxygen; SpO2: Oxygen saturation; SOFA: Sequential Organ Failure Assessment; CRP: C-reactive protein; LDH: Lactate-dehydrogenase COPD: Chronic obstructive pulmonary disease.
Studies on the efficacy of IP in previous pandemics in the literature have found that it reduces the rate of hospitalization and mortality. Although IP can be therapeutic in critically ill COVID-19 patients, clinical benefit is not yet known despite its usage.
Our study aims to determine the effectiveness of IP in patients diagnosed with COVID-19 that we followed in the ICU.
2. MATERIALS AND METHODS
To conduct the study, ethics committee approval was obtained from Kütahya Health Sciences University, Non-Interventional Ethics Committee with the decree number 2021/02-23, dated 09.02.2021. In this retrospective study, the patients who were hospitalized in the 8-bed pandemic ICU with the diagnosis of COVID-19 infection between April 2020 and July 2020, were included. The patients were divided into two groups, those who received IP treatment (Group 1; n=28) and those who did not (Group 2; n=25). The data of patients were retrospectively scanned from the patient files and the hospital automation system. The age, gender, and comorbid diseases of the patients were examined. It was recorded whether the patient needed mechanical ventilation, the number of days the patient received mechanical ventilation support, and whether the tracheostomy was performed. The hospitalization duration in the ICU, the Acute Physiology and Chronic Health Evaluation (APACHE) scoring, and the Sequential Organ Failure Assessment (SOFA) scoring, and mortality status of the patients were determined. The biochemical C-reactive protein (CRP), lactate-dehydrogenase (LDH), ferritin, D-dimer, total bilirubin, creatine levels, hematological parameters (leukocyte, neutrophil, lymphocyte, platelet counts), clinical sepsis scores, (SOFA, APACHE scores), and mortality rates of the patients were evaluated according to groups. Voluntary standard donor selection criteria from which immune plasma to be used in the treatment of COVID-19 will be procured were made in accordance with the instructions of the "Ulusal Kan ve Kan Bileşenleri Hazırlama, Kullanım ve Kalite Güvencesi Rehberi" and "European Medicines and Health Services Quality Directorate (EDQM)" [10].
Immune plasma taken from the donor by apheresis method; It can be stored for 3 years by freezing below -25 degrees. In patients for whom immune plasma therapy was planned, serum IgA levels were measured. It was found to be normal. Immune plasma to be given to the patients in Group 1 was melted from the frozen state to the appropriate temperature and given through a large intravenous line within 30 minutes. IP was administered in group 1 on the 7th day of hospitalization (min: 1, max: 20) in intensive care. It was found that two doses of IP were administered to the patients is 200 millilitersin group 1 with an interval of 48 hours. The results were checked after the second dose of IP. The minimum recommended dose for a patient is 200 millilitres that had a neutralized antibody titer of at least 1:640 of COVID-19 immuneplasma unit.1 unit per day, 1-2 doses at 48 hours intervals, maximum 3 doses (600 millilitres) if necessary is in the form [9]. The patients in group 2 were those who were not given immune plasma.
The COVID-19 diagnosis was made according to WHO COVID-19 diagnostic criteria [2]. A COVID-19 polymerase chain reaction (PCR) test positivity from an upper respiratory tract swab sample, being 18 years of age and older, having symptoms for COVID-19 (fever, cough, shortness of breath patients) as conditions chosen and included in the study. The patients who do not meet these criteria are excluded from the study.
2.1. STATISTICAL ANALYSIS
In order to obtain the results in the tables, which contains the demographic characteristics, laboratory values, clinical and treatment characteristics of the study, a two-sample t-test was used for variables that provided parametric test assumptions such as the normal distribution assumption, and Mann-Whitney U test for non-parametric and variables which the assumption was not provided. Also, through chi-square test analysis (Pearson chi-square, Phi, Cramer's V, Contingency Coefficient) conditions such as relationship and difference between categorical variables were examined (*p<0.05). While the mean and standard deviation values of the variables were presented in the data, which the two-sample t-test was performed, in the data where the Mann Whitney-U test was used, the median (median) and first quartile (25%) values of the variables were presented. In the study, variables, which were considered to valid for differences between groups, such as age, CRP, SOFA, Apache, Apache rate, and hospitalization duration in the intensive care unit (days) were evaluated with parametric tests and other variables with non-parametric tests. While evaluating the study's findings, IBM SPSS (Statistical Package for Social Sciences) Statistics 20 program was used for statistical analysis.
3. RESULTS
Patients followed in the intensive care unit with the diagnosis of COVID-19 were included in the study. A power analysis of the study, which included 53 patients, was performed. Fifty-three patients who were followed up in the ICU with the diagnosis of COVID-19 were included in the study. Using the significance test of the difference between two independent means, the power of the test was calculated as 0.81 when the sample numbers were studied with 28 and 25 in the groups with an effect size of 0.8 and a significance level of 0.05 (95% confidence level). Supportive treatment and oxygen support were administered after all patients in both groups, which were admitted to the ICU. It was found that hydroxychloroquine and azithromycin were given as antiviral treatment. The mean age of the patients in both groups was over 65 years. 60% and 40% of the patients were male in group 1 and group 2 respectively. There was no statistically significant difference between group1 and group 2 in terms of mean age values (p=0.347) and gender distribution of the indivudals (p=0.132).
While 57% of patients in group 1 had mechanical ventilation, 43% did not have mechanical ventilation. While 52% of the patients in group 2 had mechanical ventilation; 48% did not have mechanical ventilation.There was no statistically significant difference between the groups in terms of the mechanical ventilation support (p=0.707). While 89% of the patients in group 1 did not have a tracheostomy; 11% had tracheostomy. Not all patients in group 2 had tracheostomy. No statistically significant difference was found between the groups in terms of the presence of tracheostomy (p=0.092). When the patients' comorbid diseases were examined, there was no statistically significant difference between the two groups. Approximately 39% of the patients in group 1 and 40% of the patients in group 2 were transferred to the pandemic inpatient clinic. While 61% of the patients in group 1 died, the death rate was 52% in the group 2 (Table 2).
Table 2: Demographic characteristics (age-gender) mechanical ventilation support, presence of tracheostomy, comorbidity, the first day of immune plasma administration, mortality.
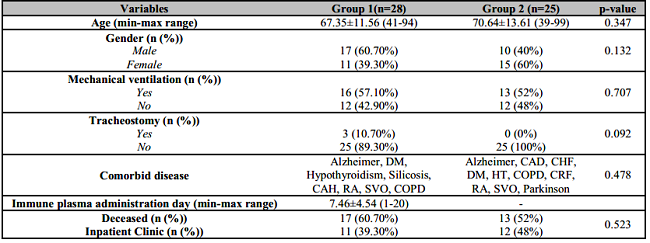
Age and immune plasma values are expressed as mean ± standard deviation. P value statistically significant: p<0.05.
CAD: Coronary Artery Disease; CHF: Congestive Heart Failure; DM: Diabetes Mellitus; HT: Hypertension; COPD: Chronic obstructive pulmonary disease; CRF: Chronic Renal Failure; RA: Rheumatoid Arthritis; CV: Cardiovascular event.
When the data in both groups were examined, there was no statistically significant difference between the two groups in terms of mean CRP, SOFA, and Apache scores. There was a statistically significant difference between the two groups only in terms of the mean duration of hospitalization in the intensive care unit. The mean value of hospitalization duration in the intensive care unit was 13.9±6.8 days in group 1, while it was 5.4±4.6 in group 2 (Table 3).
Table 3: CRP, SOFA, APACHE, duration of hospitalization in the Intensive Care Unit.

Values are expressed as mean ± standard deviation. P value statistically significant: *p<0.05.
CRP: C-reactive protein; SOFA: Sequential Organ Failure Assessment; APACHE: Acute Physiology and Chronic Health Evaluation.
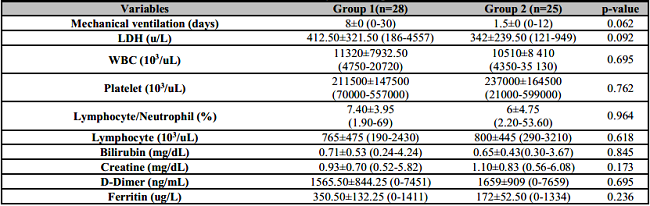
No statistically significant difference was found in the monitored laboratory values of the patients in both groups (Table 4).There was no statistically significant change in the laboratory results of the patients in group 1.
4. DISCUSSION
In terminology, convalescent plasma and hyperimmune plasma terms are used, and they refer to plasma consisting of high titer polyclonal antibodies against the virus. The antibodies found in IP may kill the virus in four ways. The first is viral neutralization by coating the virus. The second is the virolysis by activating the complement directly. The third is to facilitate the virus's uptake by immune cells, and the fourth is to promote the death of virus-infected cells [11]. Special laboratories and tests should control the antibody level in IP. However, this may not be possible for every medical center. IP treatment started quickly in a pandemic like COVID-19. It was impossible to know the antibody titer in IP, which administered to patients at the beginning of the pandemic [12]. We administered IP treatment to patients diagnosed with COVID-19, which hospitalized in intensive care, in line with the Ministry of Health guidelines (8-9). However, the minimum recommended dose for a patient is 200 millilitres that had a neutralized antibody titer of at least 1:640of COVID-19 immune plasma unit. Approximately 25.9% of patients diagnosed with COVID-19 are hospitalized in the ICU [13]. There is currently no vaccine or approved antiviral regimen for the treatment of critically ill patients. The treatments of patients diagnosed with COVID-19 in the ICU are treated with mainly supportive treatments such as infection control, hemodynamic stabilization, acute kidney ınjury and renal replacement therapy, pharmacologic interventions, extracorporeal membrane oxygenation, mechanical ventilation, and fluid management [14]. With this study, we aimed to determine the effectiveness of IP treatment in patients’ diagnosed with COVID-19 in ICU. In our study, no statistically significant difference was found between the two groups in terms of mortality. While the patients' mortality rate in group 1 was 60.7% and 52% in group 2. IP was also used in the West African Ebola epidemic in 2013. Fifty three were included and groups with and without IP were compared. Shorter symptom duration was observed in the IP group. While the mortality risk was found to be 31% in the group with IP, and 38% in the group which not given [15]. The studies conducted with IP in the literature stated that early IP administration significantly reduced mortality [16, 17, 18, 19]. Several studies also concluded that IP treatment does not affect mortality. In a study, by Ling et al. administered supportive treatment as well as IP to 52 patients diagnosed with severe COVID-19 and only supportive treatment to 51 patients. 28-day improvement was seen with 51.9% in the IP group and 43% in the supportive treatment group. No significant difference was observed in mortality rates between the two groups [20]. Zhen et al. compared the mortality of 6 patients which administered IP and 15 patients who were not which critically ill COVID-19 patient. As a result, they stated that IP could not reduce mortality in critically ill COVID-19 patients, and treatment should be started earlier [21]. In a meta-analysis conducted by Psaltopoulou et al. summarizing the available evidence on IP with COVID-19, which registered trials and guidelines from the authorities, they concluded that IP treatment should be administered in severe cases and as early as possible to maximize efficacy [22].
No significant difference was found between the two groups in terms of WBC, lymphocyte, thrombocyte, lymphocyte, and neutrophil percentage. In the literature, it is stated that the regression in the infection parameters of the patients, especially lymphopenia, is an essential parameter for follow-up. Duan et al. determined that after IP administration to 10 patients diagnosed with COVID-19 in April 2020, oxygen saturation and lymphocyte values increased. They stated that IP could be used as promising rescue therapy for severe COVID-19 patients [23]. In the study, which conducted by Shen et al. published that the symptoms and laboratory values of five critical COVID-19 patients resistant to steroid and antiviral treatment after IP administration. It was reported that symptoms of five patients regressed three days after treatment, respiratory functions improved, lymphocyte count increased, and chest radiography findings improved after seven days [24]. Erkut et al. did not find a significant difference in leukocyte, neutrophil, lymphocyte, thrombocyte, CRP, ferritin, LDH, ALT, AST, SpO2, and total bilirubin values, which measured one week after the IP treatment given to 26 COVID-19 patients who were followed up in the intensive care unit. They stated that it could effectively treat patients in the early period without the need for mechanical ventilator support [25].
In a multi-center study conducted in Kuwait, Alsharidah et al. compared 135 patients who were given IP and 233 moderate and severe COVID-19 patients who did not. They found that the 30-day mortality was significantly lower in the group given IP and IP was significant in clinical improvement. They found that the number of lymphocytes increased, and CRP levels decreased in patients with administered IP [26]. In a study comparing 40 patients with and without IP, Omrani et al. found that the decrease in CRP, WBC, creatine, ferritin, and ALT values and the increase in thrombocyte and lymphocyte count were not different in both groups, and they concluded that the recovery of the patients was not directly related to IP [27].
Although IP has historically proven useful in treating some viral diseases, its use in the treatment of COVID-19 is still controversial. Although IP administration seems to be safe in studies conducted to date, transfusion-related acute lung injury is among the potential risks [28]. Another issue is the proper timing of the IP treatment. IP should be administered as early as possible to maximize efficacy and should be used in critically ill cases. However, the IP efficacy in COVID-19 infection is not yet clear. IP can be therapeutic in critically ill COVID-19 patients. Joyner et al. have revealed that IP, which given to 5000 patients diagnosed with COVID-19, is safe [29]. In our study, no severe side effects were observed.
In a pandemic, IP can be an easily accessible source of antiviral antibodies. Fresh frozen plasma (FFP) is a treatment used in many clinical indications with a well-known safety profile. In our country, in the guideline published in April 2020, it is recommended to use IP between 7-14 days, preferably after the onset of symptoms in COVID-19 patients [8]. In the guideline updated in October 2020, it is recommended to be used within seven days at the latest after the onset of symptoms [9].
The indications for IP administration were narrowed, and it was recommended to be given before intensive care. They stated that IP, which is given in critical condition and when cytokine storm develops, might harm the patient since the antibodies have already been developed (Table 1). In our patients, IP was applied approximately seven days after the ICU hospitalization. According to the recently updated guideline, it seems that it was administered later than the recommended time for the treatment of COVID-19. This may be why it was not statistically significant in terms of mortality and intensive care stay in both groups.
5. CONCLUSIONS
IP was used in the early stages of the pandemic in critical intensive care patients in the COVID-19 pandemic. As time passed, publications were stating that the earlier initiation of IP in the treatment of COVID-19 would be more effective. IP treatment was started before the patients came to the intensive care unit. As a result, administering convalescent plasma at an early stage of sickness should potentially be more effective.
Our findings revealed that immune plasma treatment was not effective in recovery and decreasing the mortality rates in the COVID-19 infected intensive care unit patients. Further studies are needed to investigate the efficacy of administering immunomodulatory therapies on the outcome before the hyperinflammatory process starts.

