










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkAngiología
versão On-line ISSN 1695-2987versão impressa ISSN 0003-3170
Angiología vol.75 no.4 Madrid Jul./Ago. 2023 Epub 27-Nov-2023
https://dx.doi.org/10.20960/angiologia.00508
Technical Note
Radioguided embolization of carotid paragangliomas with Onyx©
2Department of Angiology, Vascular and Endovascular Surgery. Hospital Universitario 12 de Octubre. Madrid, Spain
INTRODUCTION
Carotid paragangliomas, also known as chemodectomas or glomus caroticum tumors, are rare tumors of the paraganglioma family being the carotid one the most common head and neck tumor originating from the paraganglionic tissue. These are rare tumors often diagnosed during the third to fourth decades of life. In addition, they are more prevalent in patients exposed to prolonged hypoxia including those living in high-altitude areas, patients with chronic obstructive pulmonary disease or heart diseases causing hypoxia.
They are found in the periadventitial layer on the posterior side of the carotid bifurcation, and are supplied by branches of the external carotid artery. They are highly vascularized tumors and are mostly benign. However, they can exhibit locally invasive behavior towards adjacent structures. They can also produce neuroendocrine substances, and cases of malignant transformation have been reported too.
Clinical presentation is often that of an asymptomatic slow-growing mass. However, they can also cause symptoms due to compression or local invasion.
Although malignant transformation is relatively low, early surgical treatment is advised due to the slow growth and local invasiveness of the tumor. Surgical resection is the primary curative treatment option.
Carotid paragangliomas are categorized based on the extent of tumor spread and damage to neurovascular structures (Shamblin classification). Surgical management poses a technically complex challenge during tumor dissection and resection due to its high vascularity, particularly in larger sizes (Shamblin type III). The development of endovascular techniques has allowed the embolization of nutrient branches as a means to reduce bleeding. However, these techniques were not stranger to risks of neurological embolization or the ability to effectively cannulate the nutrient branches based on the external carotid artery.
The objective of this Technical Note is to present a method of radioguided percutaneous embolization using embolic substances like Onyx© (ethylene-vinyl alcohol copolymer dissolved in dimethyl sulfoxide) in the preoperative preparation of the patient.
INDICATIONS AND CONTRAINDICATIONS
The indication for percutaneous embolization of carotid paragangliomas includes tumors eligible for surgical resection with favorable anatomy for percutaneous puncture and large size (Shamblin type III) in the days prior to the procedire (3 to 7 days).
Contraindications include renal and/or hepatic dysfunction, a past medical history of adverse reactions to dimethyl sulfoxide (DMSO) or situations where proper puncture-catheterization of the tumor mass cannot be achieved.
Regardings side effects, pain after DMSO administration and emitting a characteristic sweet, glue-like odor in the days following the procedure have been described.
DESCRIPTION
Onyx© (ethylene-vinyl alcohol copolymer dissolved in dimethyl sulfoxide) is an embolic, biocompatible and non-degradable agent designed to promote complete occlusion of vascular lesions. This compound contains micronized tantalum (Ta) for radiographic visualization purposes, and a solvent is added to prevent its precipitation (DMSO).
Onyx is currently available in 3 different formulations: Onyx-18 (6 % EVOH), that is less viscous and more useful for distal embolizations, Onyx-12 and Onyx-34 (8 % EVOH). Another embolic agent that can be used is SQUID© —similar to Onyx but with even more micronized tantalum— resulting in a more stable solution. The most widely used concentration is 6 %.
Prior to the procedure, it is necessary to shake the Onyx solution for, at least, 20 min using a specific machine until the moment prior to its injection.
TECHNICAL PROCEDURE
The procedure is started after obtaining the patient's informed consent with vital sign monitoring, placement of surgical drapes, and asepsis and antisepsis of the region of interest. The procedure is performed under local anesthesia.
Arterial access is then attempted often via right common femoral artery. However, other arterial access sites like radial arteries can be used. This arterial access will allow us to perform diagnostic arteriographies and monitoring throughout the procedure. Therefore, a puncture set with a metal needle, hydrophilic guidewire, and a 4-Fr introducer sheath is used for this purpose.
Before confirming the correct vascular access, a 100 cm Simmons-type hydrophilic catheter or a 100 cm vertebral catheter is mounted over the hydrophilic guidewire under radiological guidance. Afterwards, the latter is removed, and the initial angiography is performed to locate the glomus tumor and carotid bifurcation (Fig. 1).
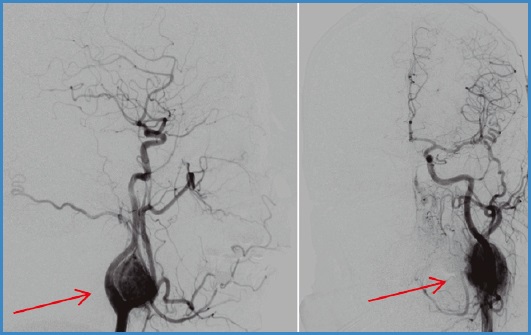
Afterwards, percutaneous diagnostic puncture of the tumor mass (ultrasound guided) and administration of contrast are performed under radiological guidance to better define the area to be sclerosed.
Finally, after preparing the sclerosing agent, the lumen of the metal puncture needle should be filled with DMSO to prevent copolymer precipitation inside the lumen. Transcutaneous puncture and local injection of Onyx are performed with angiographic control during the entire procedure, thus avoiding inadvertent puncture of the carotid arteries and selecting the area with the greatest susceptibility to sclerosing and the best trajectory towards the tumor.
Once injected, the material flows as molten lava into the tumor space through the numerous vascular branches. The injection should be slow, not exceed 0.3 mL/min, and be spaced up to 2 min apart. The final solidification occurs within 5 min after the administration of the agent.
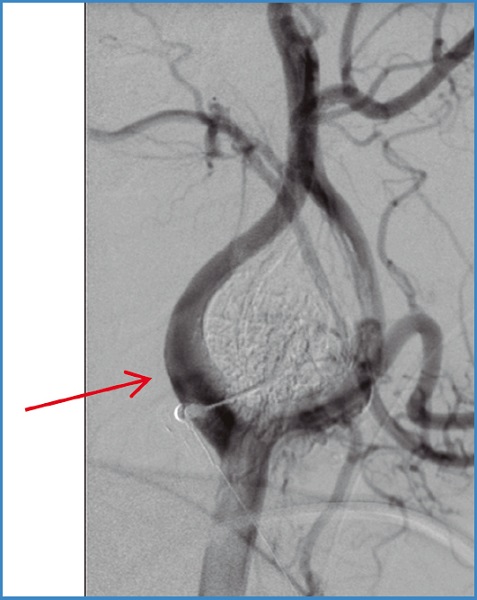
A final angiographic control is performed, and if the result is satisfactory, the catheter and femoral introducer sheath are removed, followed by the final compression of the puncture site (Fig. 2).
García Gutiérrez A, González-Fajardo JA. Radioguided embolization of carotid paragangliomas with Onyx©. Angiología 2023;75(4):273-275
REFERENCES
1. Chow WB, Moore WS, Lamuraglia GM. Carotid Body Tumors. En:Sidaway AN, Perler BA (coord.). Carotid Body Tumors. Rutherford's Vascular Surgery and Endovascular Therapy. Philadelphia (PA, USA): Elsevier Health Sciences Chapter; 2019. 1255-64. [ Links ]
2. Liberato Cano CP, García Villanego J, Pérez Martín A, et al. Embolización percutánea con Onyx por punción directa de tumores hipervasculares en la región cervical. 2019. Sociedad Española de Radiología Médica (SERAM). DOI: 10.1594/seram2014/S-0003 [ Links ]
3. Navarro Garre M, Astudillo Reyes PS, Viñán Robalino CE, et al. Resección de paraganglioma carotídeo previa embolización percutánea con Onyx® bajo control radiológico. Cirugía Española 2021;100(12):802-4. DOI: 10.1016/j.ciresp.2021.09.014 [ Links ]
Received: March 10, 2023; Accepted: April 21, 2023
 This is an open-access article distributed under the terms of the Creative Commons Attribution License
This is an open-access article distributed under the terms of the Creative Commons Attribution License
