










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
Schizophrenia is the most common psychotic disorder to be found amongst the non-affective psychotic syndromes contained in the DSM-5 under the heading Schizophrenia and other psychotic disorders. Annual prevalence is 0.3% and annual incidence is 0.8 cases per 10,000 inhabitants, which means 4,000 new diagnosed cases of schizophrenia in Spain1.
The inmate population of the Spanish prison system was 51,602 in February 2017, according to figures published by the Spanish General Secretariat of Prisons (IIPP)2, which belongs to the Ministry of Home Affairs. 92.45% of said population are men and 7.55% are women. The inmates are located in different establishments, most of which are ordinary prisons, while there are two high security hospitals in Alicante and Seville.
The World Health Organisation (WHO) estimates that in Western societies the incidence of psychiatric disorders is up to seven times higher in the prison population. Several studies have been carried out in Spain to establish the number and types of mental pathologies that exist in prisons. The results obtained show that 84.4% present some kind of mental disorder, while severe mental illnesses, most of which fall within the definition of psychosis, make up 4.2% of the cases3-5. Drug dependence is also a major destabilising factor in this population. It is estimated that 76% of the inmates consumed drugs in the month prior to entering prison6.
For healthcare, the Spanish inmate population depends on the General Subdirectorate for Coordination of Prison Healthcare, which in turn answers to the General Secretariat of Prisons, in accordance with Organic Law 1/1979 and Royal Decree 190/1996, with the exception of the communities of Catalonia and the Basque Country, where the prison healthcare powers have been transferred to the Health Departments of their Autonomous Governments. The range of healthcare options available within the network of the General Secretariat of Prisons for persons suffering from some kind of psychiatric illness includes:
Intervention by psychiatrists, who are staff members at the high security hospitals, or consultants at the other prisons.
Dispensation of prescribed medication.
Development of specific programs, such as the Comprehensive healthcare program for mentally ill patients (PAIEM in Spanish).
Given the high prevalence of mental illness, the use of antipsychotics in the prison milieu is widely extended. In recent years there has been an increase in the use of long-acting antipsychotic injectables (LAI), in parallel with the increased use of this therapy outside prison7,8. However, no differences in efficacy between the oral and injected formulations have been observed9. Treatments with LAIs frequently include the use of more than antipsychotic drug10-12 (some studies report up to 75.9% of antipsychotic polytherapy), although most clinical guides do not recommend the simultaneous use of more than one antipsychotic because of the risk of increased adverse effects and of pharmaco-kinetic interactions13. The appearance of adverse effects (extrapyramidal reactions, weight gain, etc.) may lead to non-compliance with treatment14 and sometimes cause subsequent use of doses higher than the ones recommended in the summary of product characteristics15.
The objective of this study is to evaluate the prevalence of antipsychotic treatments in the Spanish prison population, establish if there are differences in terms of efficacy and the financial costs of the LAIs used in prisons managed by the General Secretariat of Prisons, and determine to what extent doses higher than the ones established in the summary of product characteristics are prescribed for each antipsychotic drug included in the study.
MATERIALS AND METHODS
An observational, retrospective study was carried out at twelve prisons and two high security psychiatric hospitals. No interviews with patients or interventions that altered the prescription or dispensation of drugs were required. The data was gathered in the first week of March 2017, in unlinked form to ensure the confidentiality of the data.
Each participating centre was sent a table, containing the names of the participating centres and the total number (n) of inmates present at the time the study commenced. The clinical histories were reviewed, in order to find out the number of inmates receiving some kind of prescribed antipsychotic treatment. The clinical histories were also consulted only those that complied with the condition of antipsychotic therapeutic stability were selected. This criterion was defined as a “stable LAI regimen, at a fixed dose, for a minimum of three months”.
The following information about the patients was gathered: a) anonymous identification of the patient; b) prison; c) gender; d) age (in years); e) psychiatric diagnosis; f) LAI drug(s) prescribed, indicating the dose and frequency of administration.
For antipsychotic polytherapy, data about the concomitantly prescribed oral and injectable antipsychotics was gathered, indicating the daily dose. The drugs regarded as antipsychotics are those included in group N05A of the Anatomical Therapeutic Chemical Classification (ATC). An antipsychotics monotherapy is regarded as such when only one LAI was recommended, and polytherapy was considered to be treatment that consisted of an LAI and another prescribed concomitant oral or injectable antipsychotic. As regards the doses, the summaries of product characteristics were consulted and the following maximum doses for the LAIs included in the study were extracted: aripiprazol = 400 mg/28 days, flufenazine = 100 mg/28 day, olanzapine = 405 mg/28 days, monthly paliperidone = 150 mg/28 days, paliperidone quarterly = 525 mg/90 days, risperidone = 50 mg/14 days and zuclopentixol = 200 mg/14 days. When the summary of product characteristics stated that administration is monthly, it was included in four weeks (28 days). Regimens with doses over the maximum stated in the summary of product characteristics in an interval equal to or less than the one recommended were regarded as over-dosages. The prices of the LAIs were also gathered from the laboratory lists and the ex-factory prices (EFP) without VAT were included for assessment purposes.
All the data collected from each centre was grouped onto a common Excel spreadsheet for subsequent appraisal and application of the statistical study. The data is presented as means ± SEM (standard error of the mean) of the values obtained in the data collection, and the significance of the differences observed was calculated with the Student two-tailed unpaired t test. The ANOVA variance analysis was used for comparisons of means of multiple groups. The data was considered to be statistically significant when the value of “p” was less than 0.05.
The corresponding authorisation mandatory for this area of research in prisons was requested. The authorisation was granted in December 2016 the general assistant secretary of Institutional Relations and Territorial Coordination of the General Secretariat of Prisons, which forms part of the Ministry of Home Affairs.
RESULTS
1,851 inmates were prescribed an antipsychotic (87.36% of the inmates of the high security hospitals and 12% of prison inmates) and 340 received an LAI as part of their treatment. After excluding those who did not comply with the criterion of antipsychotic therapeutic stability, the population was reduced to 292 patients. Of these, 275 were man with a mean age of 42 years and 17 were women with a mean age of 43 years (Table 1).
Table 1 Inmates/patients included in the study
| Prison or hospital | Nº inmates | Patients with antipsychotics* | Patients with LAI Total LAI/Stable LAI | % Total patients with LAI compared to patients with prision antipsychotics |
|---|---|---|---|---|
| Alicante High Sec. Hosp | 289 | 264 (91.3%) | 113/113 | 42.8% |
| Seville High Sec. Hosp | 186 | 151 (81.2%) | 72/56 | 47.7% |
| Subtotal Hospitals | 475 | 415 (87.4%) | 185/169 | 44.6% |
| Albolote | 1299 | 140 (10.8%) | 36/32 | 25.7% |
| Alicante sentence | 728 | 24 (3.3%) | 7/6 | 29.2% |
| Córdoba | 1265 | 127 (10.0%) | 19/19 | 15.0% |
| El Dueso | 453 | 88 (19.4%) | 7/3 | 7.9% |
| La Moraleja | 953 | 240 (25.2%) | 14/7 | 5.8% |
| Madrid III-Valdemoro | 1037 | 74 (7.1%) | 11/11 | 14.9% |
| Madrid IV-Navalcarnero | 1089 | 185 (17.0%) | 12/7 | 6.5% |
| Madrid V-Soto del Real | 1333 | 81 (6.1) | 5/3 | 6.2% |
| Málaga | 1188 | 107 (9.0%) | 12/10 | 11.2% |
| Pamplona I | 271 | 56 (20.7%) | 6/4 | 10.7% |
| Valladolid | 500 | 55 (11.0%) | 4/2 | 7.3% |
| Zaragoza | 1362 | 259 (19.0%) | 22/19 | 8.5% |
| Subtotal Prisons | 11478 | 1436 (12.5%) | 155/123 | 10.8% |
| Total hospitals + prisons | 11953 | 1851 (15.5%) | 340/292 | 18.4% |
Note. *Patients with antipsychotics: % regarding the population of the prison.
The diagnoses showed that 181 presented schizophrenia, and 52 had other psychotic disorders (25 diagnosed with secondary psychotic disorder from substance consumption). 39 cases were diagnosed with personality disorder, four with impulse control disorder, three with bipolar disorder, two with intellectual disability, one with Gilles de la Tourette syndrome, one with severe depression and psychotic symptoms and one with agitation.
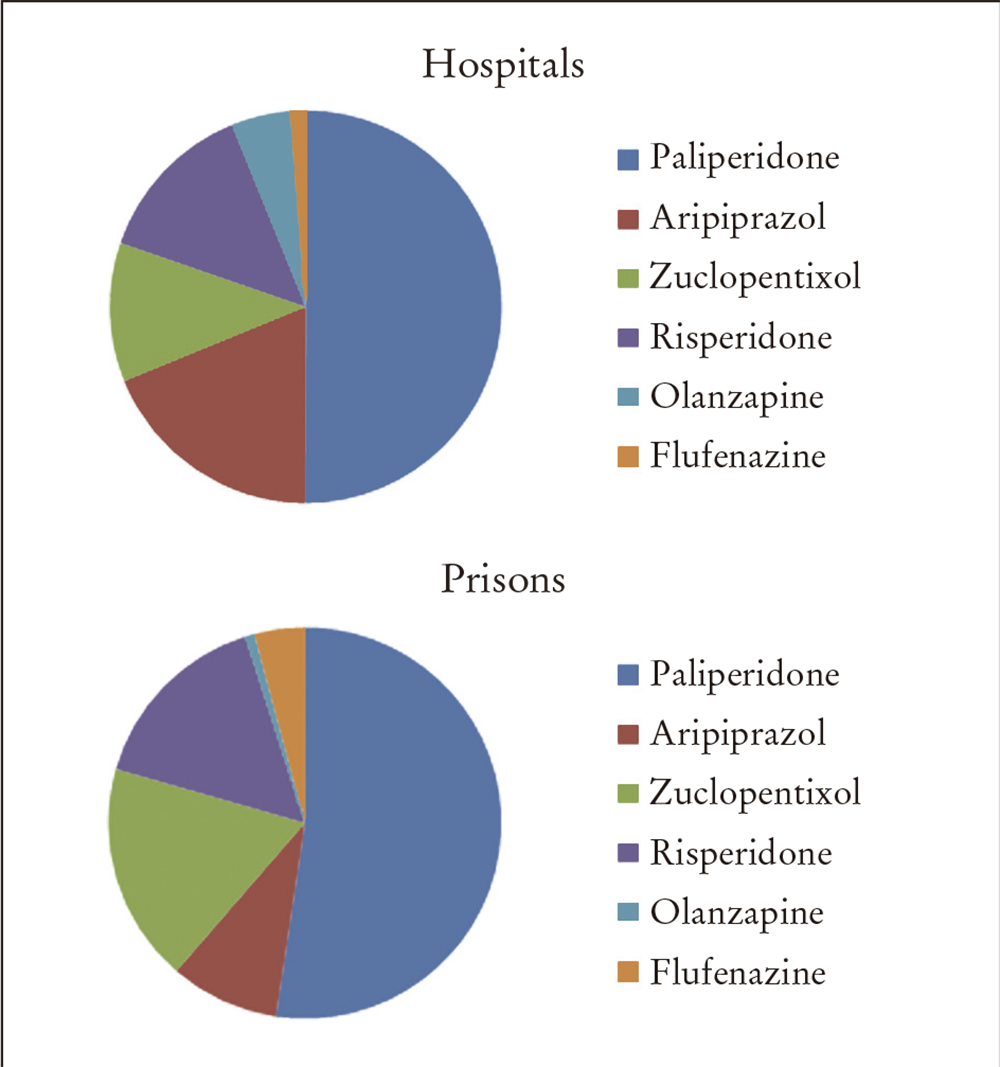
The prescription pattern showed that paliperidone was the most commonly prescribed antipsychotic (50%), followed by aripiprazol, zuclopentixol and risperidone, in very similar percentages, which were approximately 14%. Flufenazine and olanzapine were only prescribed for 3%, and quarterly paliperidone for 1%. However, the last of these drugs was placed on the market in 2016, which made the option of prescribing it a difficult process (Table 2 and Figure 1).
Table 2 Distribution of LAI prescriptions in two hospitals and in prisons
| Hospitals | Prisons | % Hospitals | % Prisons | |
|---|---|---|---|---|
| Aripiprazol | 31 | 11 | 18 | 8.9 |
| Flufenazine | 5 | 5 | 3 | 4.1 |
| Olanzapine | 8 | 1 | 4.7 | 0.8 |
| Paliperidone | 82 | 64 | 48 | 52 |
| Risperidone | 22 | 19 | 13 | 15.5 |
| Zuclopentixol | 19 | 22 | 11.2 | 18 |
| Palip quarterly | 2 | 1 | 1.2 | 0.8 |
| Total | 169 | 123 |
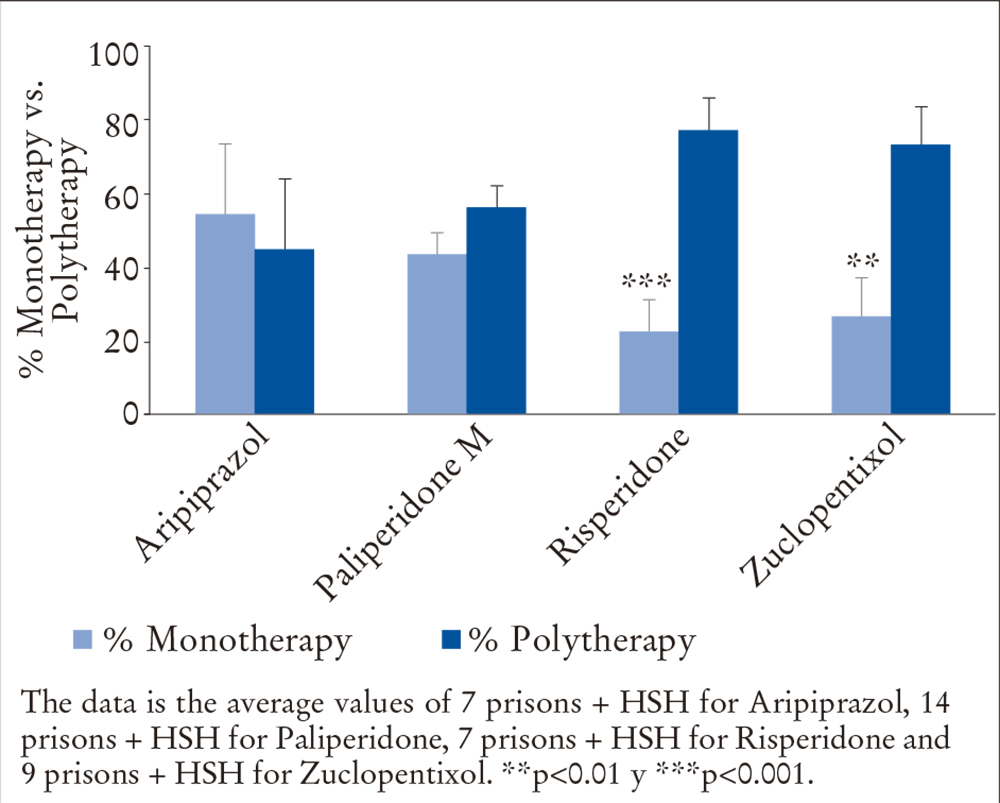
The level of association between LAI and other antipsychotics showed that 191 (41%) were receiving monotherapy and 171 (59%) were undergoing polytherapy. Only two LAIs were associated with two, and an injectable antipsychotic was associated with an oral one. 19% had been prescribed oral antipsychotics, and in one case, three oral drugs. Figure 2 shows the percentages of antipsychotics in monotherapy compared to polytherapy and the statistical association.
As regards oral antipsychotics associated with an LAI, olanzapine and quetiapine were the most frequently used combination (37% and 31% of the cases of polytherapy, respectively) and haloperidol, amisulpride and paliperidone were the ones least combined (percentages below 3%). Other antipsychotics (aripiprazol, clozapine, clotiapine, levomepromazine and risperidone) were combined in 13%, 10.5%, 10%, 6.5% and 6%, respectively.
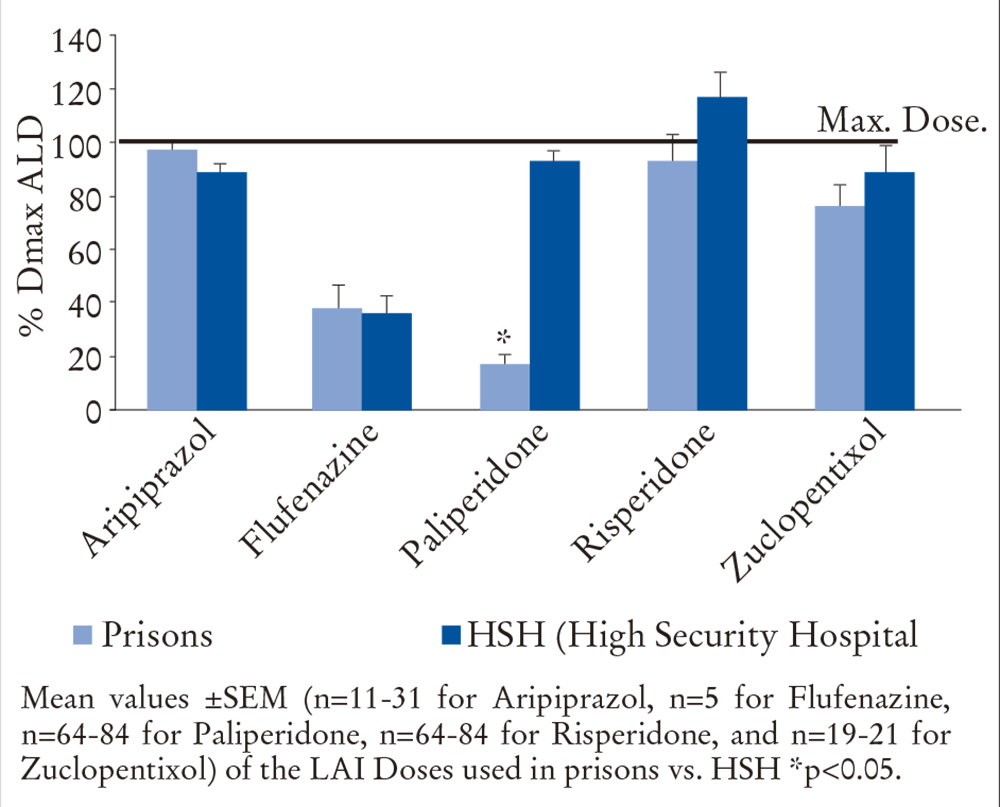
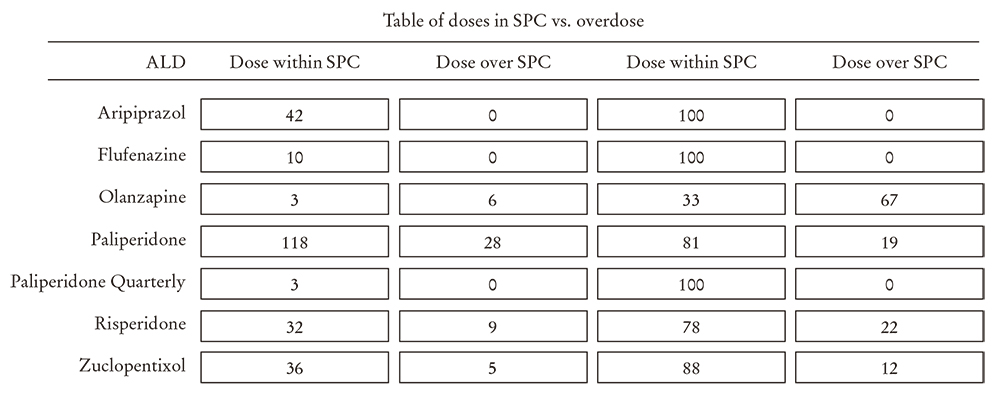
83.6% of the prescribed treatments (n = 244) were within the therapeutic range, and 16.4% at doses above this range (Figures 3 and 4). The result, broken down into each drug, is as follows:
In prisons and high security hospitals, the prescriptions of aripiprazol (97.72 ± 2.38 and 88.62 ± 3.32, respectively), flufenazine (38.33 ± 8.12 and 35,.99 ± 6.7, respectively) and zuclopentixol (76.32 ± 8.11 and 89.12 ± 9.42, respectively) were within the therapeutic range interval.
In prisons and high security hospitals, the prescriptions of paliperidone were also within the therapeutic range (17.37 ± 3.43 and 93.06 ± 3.97, respectively), but with statistically significant differences between both types of centers (p<0.05).
In prisons and high security hospitals, the prescriptions of risperidone (93.42 ± 9.38 and 116.66 ± 9.24, respectively) were made above the dose recommended in the summary of product characteristics.
As regards the financial cost, the mean cost per LAI and patient was 252.8 euros/28 days (Table 3). There is a highly variable interval, between those of higher cost, which correspond to the ones recently marketed, and the others. Thus, the cost of paliperidone is 338.92 euros, while the cheapest one, flufenazine, is 3.06 euros.
Table 3 Study of measured expenditure according to drug used
| Coste de todos los centros penitenciarios | |
|---|---|
| Cost for all prisons | |
| Average cost a year of all LAIS per stable patient | 3.286,43 € |
| Reported average cost at 28 days | 252,80 € |
| Patients | 292 |
| LAI | |
| Average cost per year of ariprazol | |
| Per stable patient | 2.982,75 € |
| Reported average cost at 28 days | 229,44 € |
| Patients | 42 |
| Average cost per year of flufenazine | |
| Per stable patient | 39,81 € |
| Reported average cost at 28 days | 3,06 € |
| Patients | 10 |
| Average cost per year of olanzapine monthly | |
| Per stable patient | 4.302,84 € |
| Reported average cost at 28 days | 330,99 € |
| Patients | 9 |
| Average cost per year of paliperidone | |
| Per stable patient | 4.405,96 € |
| Reported average cost at 28 days | 338,92 € |
| Patients | 146 |
| Average cost per year of paliperidone quarterly | |
| Per stable patient | 2.698,59 € |
| Reported average cost at 28 days | 207,58 € |
| Patients | 3 |
| Average cost per year of risperidone | |
| Per stable patient | 3.411,76 € |
| Reported average cost at 28 days | 262,44 € |
| Patients | 41 |
| Average cost per year of zuclopentixol | |
| Per stable patient | 97,31 € |
| Reported average cost at 28 days | 7,49 € |
| Patients | 41 |
DISCUSSION
There is a high prevalence of pathology in the prison environment2. Furthermore, the unfavourable environment, the lack of awareness in some cases of the illness and the possible fear of patients of being stigmatised as someone who is mentally ill, may have a lot to do with low adherence to treatment. Therefore, the use of LAIs may be a very attractive option for prisons and high security hospitals to ensure patient adherence.
New LAIs have recently been put onto the market (aripiprazol, olanzapine and paliperidone), at a cost way above that of antipsychotics already on sale, which puts into question if the efficacy/economic cost quotient really implies a benefit for the health system.
The idiosyncrasies of the prison environment, where patients feel a certain degree of fear about being affected by regulatory measures and where there are considerations of an ethical nature that complicate the processes involved in experimental studies, have played part in the decision to carry out an observational study. There is a higher probability of bias in this type of study, but it does avoid the use of standardised scales and enables work to be done with a very numerous patient sample.
The results show that the LAI recently included in the Medical Drug Guide, such as aripiprazol and paliperidone, and to a lesser extent other drugs such as olanzapine, zuclopenxitol, risperidone and flufenazine require less frequent association with other antipsychotics to stabilise the patient.
The rate of antipsychotic prescription in Spanish prisons is in the range (4-70%) shown in scientific publications, depending on the place and population studied16.
Olanzapine and quetiapine stand out amongst the prescribed oral antipsychotics associated with LAIs, probably because of their greater sedative capacity, which is highly beneficial for some patients. In the case of olanzapine, this may also be due to the search for a synergistic effect in the mechanism of action of the associated drugs.
As regards the cost of treatments, only the direct costs have been taken into account, and it was found that there were major differences between them. Zuclopentixol and flufenazine are the most economical options compared to aripiprazol, risperidone, olanzapine and paliperidone, in decreasing order.
The conclusion can be drawn that: aripiprazol and monthly paliperidone present the best results in accordance with the measured variable, which is the level of prescription in monotherapy. Aripiprazol works at a lower cost than monthly paliperidone. Zuclopentixol did not achieve good results, with 27.16% of co-prescriptions with oral antipsychotics. Its use may well be restricted by its potential advantages, which are: flexibility of dosage and frequency compared to the new LAIs and low cost.
Considering that this groups of medicines has a large number of adverse effects, especially effects on the metabolism and extrapyramidal symptoms, and that they are drugs that the patient is going to take for a long time, it is essential to avoid redundancy in prescribing antipsychotics. In this regard, aripiprazol and paliperidone have shown themselves to be superior in comparison to the other LAIs in the study.
CONCLUSIONS
Antipsychotic polytherapy is widely used in this environment. Given the large number of side effects and interactions with other treatments, efforts should be made to establish measures that promote the prescription of monotherapy.
The percentage of LAIs prescribed as antipsychotic treatment is less in prisons than in high security hospitals.
The LAI most recently included in the Medical Drug Guide, aripiprazol and paliperidone, have shown better results in terms of stabilising patients under a regime of prescribed monotherapy.
The LAI that is most frequently used above the maximum in the therapeutic range of the summary of product characteristics is risperidone, and this tends to take place more frequently in high security hospitals than in prisons.
Given that there is a major difference in cost between the different treatments studied, it should be another factor to bear in mind when selecting the most adequate therapeutic option.

