










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkNefrología (Madrid)
versão On-line ISSN 1989-2284versão impressa ISSN 0211-6995
Nefrología (Madr.) vol.36 no.1 Cantabria 2016
Eculizumab for the treatment of an atypical hemolytic uremic syndrome with mutations in complement factor I and C3
Eculizumab para el tratamiento de un síndrome urémico hemolítico atípico con mutaciones en los factores I y C3 del sistema del complemento
Dear Editor,
Atypical hemolytic-uremic syndrome (aHUS) is a rare, life-threatening complement-mediated thrombotic microangiopathy.1 Approximately half of cases have mutations in complement proteins but only 12% have 2 or more mutations.2 Eculizumab is nowadays considered first-line therapy for aHUS.3
A 33-year-old female with unremarkable past medical history presented with a 3-day history of decreased urine output. Physical examination showed hypertension (160/90 mmHg) and lower limbs edema. Investigations revealed an acute thrombotic microangiopathy (ATM), hematuria and nephrotic proteinuria (Table 1). Daily plasmapheresis (PMP) was started immediately.
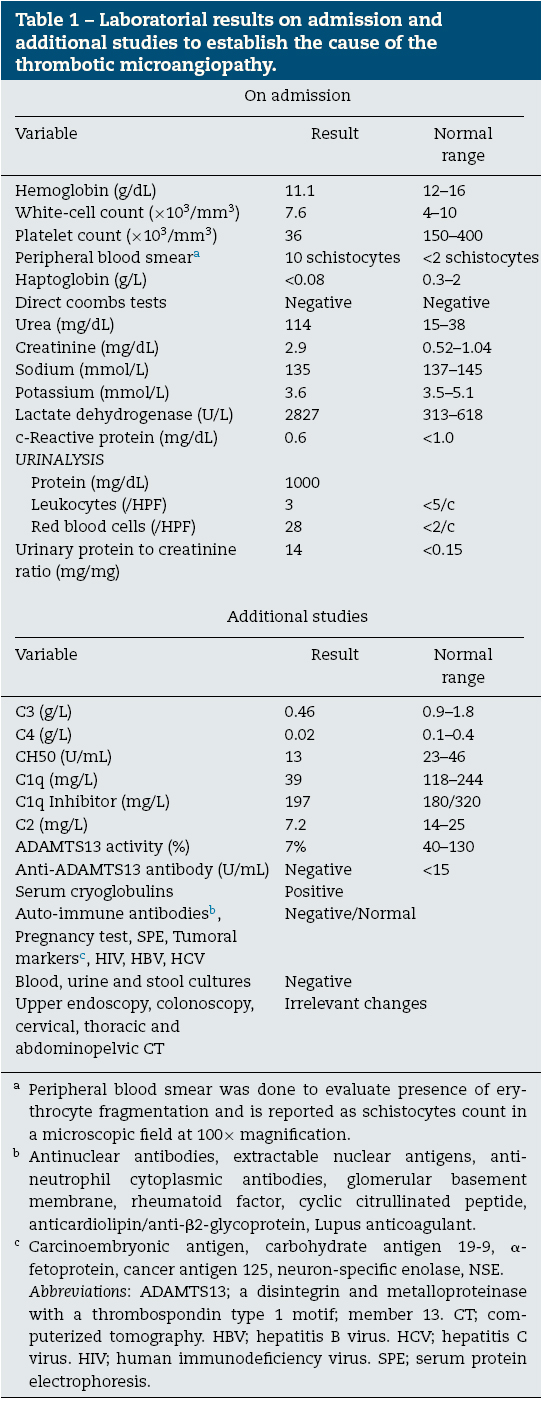
Investigations for secondary causes of ATM revealed a low ADAMTS 13 activity, decreased complement C4, C3, C1q and C2 levels and positive serum cryoglobulins (Table 1). Considering the hypothesis of an autoimmune disorder, we started 3 daily pulses of 1000 mg methylprednisolone followed by oral prednisolone.
PMP was stopped on the eighteenth day of admission (D18) due to normal platelet count during 3 consecutive days (Fig. 1). On the D19 a renal biopsy was made. It showed a "thrombotic microangiopathy with acute tubular necrosis" and "deposition of IgM, C3 and C1q in the capillary wall". Due to increased hemolytic activity, PMP was resumed on the D21. On the D27, rituximab was started to enhance immunosuppression. PMP was stopped on the D35 based on the absence of schistocytosis, hemoglobin stability and lactate dehydrogenase (LDH) normalization.

Fig. 1 Clinical course: laboratory data and treatment. Corticosteroid therapy was started
with intravenous administration of methylprednisolone (1000 mg/day for 3 days) followed
by oral prednisolone and an initial dosage of 60 mg/day. This dosage was maintained until
the 53rd day after admission, with posterior tapering. Rituximab (arrows) was administered
at a dose of 600 mg (375 mg/m2) on the 27th, 34th, 41st and 48th days after admission.
Cyclophosphamide (arrowhead) was administered in a single dose of 1000 mg on the 61st
day after admission (2nd day after readmission). Eculizumab was administered at a dose
of 900 mg for a week for 4 weeks, started on the 158th day after admission, followed by
a dosage of 1200 mg 1 week later an then a maintenance dose of 1200 mg every 2 weeks.
This dosage is still being continued. We performed a total of 79 plasma exchange sessions.
The last three laboratorial test results were done on the 270th, 340th and 466th days
following first admission.
On the D50, LDH was high but hemoglobin and platelet count were stable. A state of compensated hemolysis was assumed and the patient was discharged home.
Ten days later she was readmitted due to increased hemolytic activity (Fig. 1). PMP was resumed and 1000 mg cyclophosphamide was given. At that time ADAMTS13 and complement C4 levels were normal but complement C3 levels remained low.
A genetic screening for mutations in complement regulatory proteins was made. Two mutations were found in factor I (C. 452 A>G, pASN 151 Ser) and C3 (C193 A > C, pLys 65 Gin) proteins. The process of eculizumab acquisition was lengthy, wherefore this therapy was started only on the 98th day after readmission. At that moment we were performing one PMP session/week, LDH remained high (859 U/L) and moderate renal dysfunction (creatinine 2.08 mg/dL and urea 60 mg/dL) and nephrotic proteinuria persisted (5.2 g/24 h). Eculizumab was administered at a dose of 900 mg per week for 4 weeks followed by subsequent doses of 1200 mg every 2 weeks since the 5th week. Complete hematologic remission was attained 2 days after eculizumab initiation. The patient was discharged home on the 105th day after readmission. Four weeks later, proteinuria was only 0.6 g/24 h.
Currently, 10 months after first infusion, the patient remains under biweekly administration of eculizumab. Hematologic remission persists and there is a significant recover of renal function (urea 43 mg/dL, creatinine 1.27 mg/dL).
Complement factor I (CFI) and C3 mutations account for 10% and 4% of the overall aHUS-associated mutations, respectively.3 C3 mutations are among the ones with the poorest prognosis: 75% risk of death or end stage renal failure (ESRF) at 3-5 years follow up and 50% risk of recurrence.3 CFI mutations have a 50-60% risk of death and ESRF at 3-5 years follow up and 10-30% risk of recurrence.3
Both mutations present in our patient were previously reported.4,5 The p.Asn151Ser mutation causes a quantitative deficiency of factor I4 and the p.Lys65Gin mutation weakens the affinity of C3b to complement factor H.5
Despite the growing importance of eculizumab,6,7 PMP remains the mainstay of treatment while waiting for the immunoglobulin.3 Nonetheless, its benefit depends on the underlying genetic defect - only 25% and 57% of those with CFI and C3 mutations, respectively, achieve remission.8 In our patient, PMP was critical to prevent further progression of renal failure and the development of other systemic involvement. However, as described by Loirat,2 it was unable to achieve complete and sustained remission.
In our case, the confounding presence of low ADAMTS13, C4, C2 and C1q levels, the presence of cryoglobulins and the existence of immune deposits in the glomerular capillary wall led to the misdiagnosis of a thrombotic thrombocytopenic purpura secondary to an autoimmune disease. It explains the preference for glucocorticoids, rituximab and cyclophosphamide in relation to eculizumab.9
Eculizumab is nowadays considered first-line therapy for aHUS.3 It is a humanized monoclonal immunoglobulin IgG that targets C5 and blocks the uncontrolled generation of the cytotoxic membrane attack complex.10 When we started Eculizumab, our patient was still PMP dependent despite the 79 PMP sessions. Contrariwise, complete hematologic remission was attained two days after first infusion and a remarkable recover of renal function and reduction of proteinuria was evident. These findings reinforce the benefits of eculizumab in aHUS, even in cases of severe renal involvement.
In conclusion, our case highlights the diagnostic challenge of aHUS and emphasizes the notion that isolated PMP is no longer the best therapeutic option in aHUS, in which cases a prompt switch to eculizumab is mandatory.
The authors declare that they have no conflicts of interest related to the contents of this article.
Emanuel Ferreiraa, Nuno Oliveiraa, Maria Marquesa,
Luís Franciscob, Ana Santosa, Armando Carreiraa and Mário Camposc
a Servicio de Nefrología, Centro Hospitalar e Universitário
de Coimbra-Hospital Geral, Coimbra, Portugal
b Servicio de Hematología, Centro Hospitalar e Universitário
de Coimbra-Hospital Geral, Coimbra, Portugal
c Servicio de Nefrología, Centro Hospitalar e Universitário de
Coimbra-Hospitais da Universidade de Coimbra, Coimbra, Portugal
References
1. Fremeaux-Bacchi V. Treatment of atypical uraemic syndrome in the era of eculizumab. Clin Kidney J. 2012;5:4-6. [ Links ]
2. Loirat C., Frémeaux-Bacchi V. Atypical hemolytic uremic syndrome. Orphanet J Rare Dis. 2011;6:60. [ Links ]
3. Campistol J.M., Arias M., Ariceta G., Blasco M., Espinosa M., Grinyó J.M., et al. Actualización en síndrome hemolítico urémico atípico: diagnóstico y tratamiento. Documento de consenso. Nefrologia. 2013;33:27-45. [ Links ]
4. Bienaime F., Dragon-Durey M.A., Regnier C.H., Nilsson S.C., Kwan W.H., Blouin J., et al. Mutations in components of complement influence the outcome of Factor I-associated atypical hemolytic uremic syndrome. Kidney Int. 2010;77:339-49. [ Links ]
5. Volokhina E., Westra D., Xue X., Gros P., van N., van L. Novel C3 mutation p.Lys65Gln in aHUS affects complement factor H binding. Pediatr Nephrol. 2012;27:1519-24. [ Links ]
6. Rathbone J., Kaltenthaler E., Richards A., Tappenden P., Bessey A., Cantrell A. A systematic review of eculizumab for atypical haemolytic uraemic syndrome (aHUS). BMJ Open. 2013;3:e003573. [ Links ]
7. Legendre C.M., Licht C., Muus P., Greenbaum L.A., Babu S., Bedrosian C., et al. Terminal complement inhibitor eculizumab in atypical hemolytic-uremic syndrome. N Engl J Med. 2013;368:2169-81. [ Links ]
8. Noris M., Caprioli J., Bresin E., Mossali C., Pianetti G., Gamba S., et al. Relative role of genetic complement abnormalities in sporadic and familial aHUS and their impact on clinical phenotype. Clin J Am Soc Nephrol. 2010;5:1844-59. [ Links ]
9. Kaplan A.A., George J.N. Treatment and prognosis of thrombotic thrombocytopenic purpura-hemolytic uremic syndromes in adults. Uptodate. 2014. Available at: http://www.uptodate.com/contents/treatment-and-prognosis-of-thromboticthrombocytopenic-purpura-hemolytic-uremic-syndromesin-adults?source=search result&search=Treatment+of+thrombotic+thrombocytopenic+purpura-hemolytic+uremic+syndrome+in+adults&selectedTitle=1150#H30 (accessed14.06.14). (Updated 2014 May 14). [ Links ]
10. Keating G.M. Eculizumab: a review of its use in atypical haemolytic uraemic syndrome. Drugs. 2013;73:2053-66. [ Links ]
![]() Correspondence:
Correspondence:
Emanuel Ferreira
Servicio de Nefrología,
Centro Hospitalar e Universitário de Coimbra-Hospital Geral.
Rua do Buxo, lote 17,
3040-792 Coimbra, Portugal.
emanuelfeferreira@gmail.com

