










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
Malnutrition is highly prevalent in hospitalized patients. Butterworth et al. in 1974, were the first in talking about malnutrition in these patients 1. In the same year, Bistrian et al. reported in two different studies that half of the hospitalized patients (44% medical, 50% surgical) have certain degree of malnutrition 2,3.
Surprisingly, since then the malnutrition percentages reported in last four decades in hospitalized patients has been the roughly the same. Percentages go from 30 to 60%, in studies performed in Spain 4,5,6,7,8 or other parts of the world 9,10,11,12,13,14,15.
Malnourished hospitalized patients are at high risk of infections 16, falls 17 and pressure ulcers 18. Malnutrition is also associated with a higher mortality 19,20, higher hospital costs caused by a longer stay higher readmission rates and greater health care services utilization 21.
Consistent data have demonstrated that nutritional treatment with diet modification including oral nutritional supplements (ONS), enteral or parenteral nutrition has consistently demonstrated a beneficial effect on clinical and economical outcomes. These include improvement of the nutritional status 22, muscular mass, strength and performance, morbitity 23 quality of life 24 and mortality. Health care costs decrease is a consequence of a shorter in hospital stay 25, decrease readmission rate 26 and use of health care services in general 27.
Despite this high prevalence, malnutrition in hospitalized patients is a under-diagnosed and undertreated problem 28. Even more, 60% of them worsen their nutritional status during their admission 29.
In the PREDYCES study 30, a multicentric Spanish study, 1 out of 4 inpatients were malnourished, a condition that is associated with a longer hospital stay and with an increased health care costs especially in those that developed malnutrition during their admission.
European authorities have recognized that disease associated malnutrition is a European health problem (Praha Declaration June 11th 2009), recommending specific directives to prevent this problem and avoid the morbi-mortality associated to it 31. This directives have been integrated in the European Strategic Health Program UE 2008-2013 32.
A systematic malnutrition screening on admission and during hospital stay would be desirable aiming at improving clinical and economical outcomes.
The present study was planned to explore the nutritional status of medical and surgical patients admitted to a tertiary university hospital in La Rioja, Spain.
METHODS
This is a cross sectional study of a prospectively recruited population of a randomly sample of adult inpatients (age > 18 years old) admitted to medical and surgical wards of the Hospital Universitario de San Pedro in Logroño (La Rioja, Spain), from February to June 2011. Sample size was estimated in 384 patients considering 30-60% malnutrition prevalence with a 95% confidence interval and a precision of 5%.
Nutritional evaluation was performed within the first 72 hours of patient's admission by qualified personnel (certified dietitian). Every day patients were randomly selected using a table of aleatory numbers from the admission list.
Exclusion criteria were patients with an expected hospital stay of less than 72 hours, those with a severe disease with an imminent expected death, patients admitted to Psychiatry, Obstetrics, Ophthalmology, Intensive Care Unit, Pediatrics or those that refused to participate in the study.
Social and demographic data was registered in each patient including diagnosis and number of admissions in the previous year and laboratory lab results. Three different nutritional screening tools were used: Malnutrition Universal Screening Tool (MUST), Nutritional Risk Screening (NRS-2002) and Nutritional Control (CONUT for its spelling in Spanish), using another nutritional evaluation tool: Subjective Global Assessment (SGA). On discharge, number of diagnostic tests performed, days of hospital stay, place of discharge and mortality were registered in all patients.
STATISTICAL ANALYSIS
Results are presented as mean and standard deviation for quantitative variables and percentages for qualitative variables. Normality was tested in quantitative variables with the Kolmogorov-Smirnov test.
Difference between quantitative variables with normal distribution was evaluated with Student t test or Mann-Whitney U test for those with non-parametric distribution. Difference between quantitative variables was evaluated with 2. Comparison between different nutritional screening tools was explored with χ2 and ANOVA. Concordance between nutritional screening tools was evaluated with kappa index. A statistical significance level of p < 0.05 was determined. The statistical package IBM SPSS Statistics 21 was used for the statistical analysis.
The study was approved by the Clinical Research Ethical Committee of La Rioja and all the participants signed the informed consent.
RESULTS
Three hundred and eighty four inpatients were evaluated, 71.7% admitted to medical wards and 28.9% to surgical wards. Fifty percent of them were men and their mean age was 64.6 ± 16.5. Eighteen percent of patients had a previous diagnosis of diabetes mellitus, 42% of high blood pressure, 21% of dyslipemia and 16% had obesity.
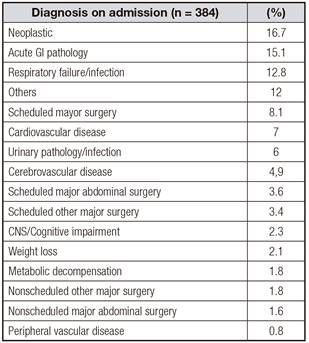
Table I shows the cause of admission being neoplastic the most frequent one in 16.7%.
Mean body mass index (BMI) was 25.7 kg/m2, 6.2% of patients had a BMI < 18.5; 33.7% have overweight and 15.7% obesity. Mean percentage of weight loss from regular weight was 4.8 ± 5.8. The mean hospital-stay was 8.7 ± 6.8 days and 51% of patients had an admission in the previous 12 months.
Results of the nutritional screening using 3 different nutritional screening tools are shown in figure 1.
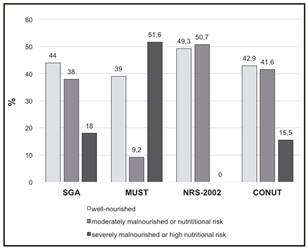
All patients underwent a SGA showing that 44% of them were well nourished, 38% mildly malnourish and 18% severely malnourished.
Concordance between SGA and the other screening tools was explored showing a good kappa index with NRS-2002 (k = 0.758), moderate with MUST (k = 0.422) and weak with CONUT (k = 0.340).
Malnutrition according to the cause of admission was 23.4% in neoplastic patients, 18.2% in those with acute GI pathology and 15.4% in those with acute respiratory infection/failure.
No statistical significant gender differences were found in malnutrition. A higher percentage of patients older than 70 years old was malnourish (70.4 vs. 45.7%, p < 0.05) and higher in medical than in surgical services (63.1 vs. 38.7%, p < 0.05).
Malnourished patients had a mean age 10 years higher than those well-nourished, weighted 11 kg lower and have a BMI 4 points lower. Mean weight loss of malnourished patients were 4.9 kg vs. 0.7 kg of those well-nourished. Statistical significant differences were found also in other anthropometric measurements: tricipital skinfold (TSF), arm circumference (AC) and calf circumference (CC) (Table II).
Table II Anthropometric parameters according to their nutritional state (SGA)

*In > 65-years-old. SGA: subjective global assessment; BMI: body mass index; TSF: triceps skinfold; AC: arm circumference; CC: calf circumference.
Malnourished patients also had lower values of albumin, prealbumin, transferrin, cholesterol and CRP (Table III).
Table III Laboratory parameters according to their nutritional state (SGA)

SGA: subjective global assessment (SGA); CRP: C-reactive protein.
Sixty two percent of the malnourished patients had an admission in the previous year compared with only 45.5% of well-nourished ones. Mean hospital stay was 2 days higher in those malnourished (9.29 vs. 7.10, p < 0.05). During their hospital stay the number of diagnostic procedures in malnourished patients was higher compared with well-nourished ones (16.4 ± 12.6 vs. 12.5 ± 10.6, p < 0.005) and they used a greater number of medicines (9.2 vs. 7.4; p = 0.001) (Table IV).

Being malnourished increased the hospital length of stay by 1.8 days (IC ± 95%: 0.3-3.2; p < 0.05) in a regression model adjusted by age, gender, weight on admission, BMI, weight loss and diagnosis on admission.
Ninety two percent of the well-nourished patients went home at the time of discharge compared with 77% of those malnourished. A higher percentage of malnourished patients were discharged to a chronic health facility compared with those well-nourished (7 vs. 0.6%, p < 0.05). Three percent of the malnourished patients died during their hospital stay compared with only 0.6% of those well-nourished (p = 0,06).
Only 17.7% of the malnourished patients received nutritional support during their hospital stay.
DISCUSSION
Malnutrition is frequent in hospitalized patients causing a negative impact on mobility and mortality with the expected increase in health care associated costs.
Disease and malnutrition have a two way relationship. While disease could cause malnutrition, malnutrition negatively affects the main outcomes of the disease closing a vicious cycle 33.
La Rioja is an autonomous community with centralized sanitary system with only one tertiary university hospital where the present surveillance was performed.
The study sample of 384 hospitalized patients is representative of the acute hospitalized patients of this autonomous community.
Using the SGA evaluation, malnutrition was found in 56% of the hospitalized patients (38% with moderate and 18% with severe) while using any of the other screening tools (MUST, NRS-2002 y CONUT) malnutrition prevalence was always above 50%. If we compared the malnutrition prevalence found in the present work with the one found in the PREDYCES study 30 including a large Spanish sample of hospitalized patients, the figures found in La Rioja are two times higher indicating that one out of two patients are malnourished in La Rioja while one out of four in the rest of Spain. The present study confirms previous findings from a study performed in 2001 that found only 12.5% of hospitalized patients in La Rioja have a normal nutritional state on discharge, with 55% of them with mild malnutrition and 28.3% severe malnutrition 34. The prevalence of disease-associated malnutrition in other Spanish areas ranges from 24 to 66% 4,5,7. If we compared the present study findings with the ones from Latin American countries, the figures are quite similar, again with a prevalence of disease associate malnutrition of approximately 50% in the latter 10. The British Association for Parenteral and Enteral Nutrition (BAPEN) estimate that around 34% of the patients admitted to a hospital have some degree of disease associated malnutrition 35. These percentages are similar to those found in other European countries 36,37. The differences found between these studies could be related to study populations and methodology to define malnutrition in each cohort.
The present study also confirmed other studies findings indicating that a higher percentage of malnutrition is found in those patients older than 70 years old 8,30.
We also confirmed that those patients classified as malnourished have a 2.19 days longer hospital stay than those classified as well nourished 4,5,8,27,29 supporting the importance of detecting this problem on admission to avoid important health care associated costs. Then, the detection of malnutrition on admission with easy screening tools could contribute indirectly to save health care associated costs 38.
Our study also confirmed that disease associated malnutrition is also associated with higher medication consumption and performing a higher number of diagnostics tests, findings previously described in other studies performed in Spanish populations 7,29. This confirmed the external validity of our findings and again supporting the critical role of the malnutrition screening tools to detect this important issue.
The percentage of malnourished patients that were discharged home was significantly higher in those well-nourished while a higher percentage of those malnourished needed to be transferred to a chronic health facility. But most importantly, the mortality rate was also significantly higher in the malnourished patients. These findings are all in line with the findings reported in other Spanish as well as North and Latin American studies 4,5,10,27,28,30.
Finally, the present study also showed that SGA evaluation has a good concordance with NRS-2002 and weaker with the CONUT, confirming previous reports that those screening tools including biochemical parameters are not probably the adequate tools to be used in nutritional screening 39).
There are some limitations in the present study. Firstly, this is a single center study, therefore the present findings could not be translated to other populations. Secondly, we only evaluated three screening tools. We did not included Mini Nutritional Assessment (MNA) that is the recommended screening tools for patients older than 65 years old. Thirdly, the present study only included a limited number of surgical patients, but this is a representative sample of the type of patients seen in our hospital.
The most important findings from the present work are:

