










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkINTRODUCTION
Osteoporosis is a metabolic bone disease characterized by decreased bone mass and impaired microarchitecture of bone tissue, leading to increased bone fragility and increased risk of fracture 1,2. Some factors could contribute to reducing bone mass and increasing bone fragility, such as incapacity to reach optimal peak bone mass, bone loss owing to increased resorption, or erroneous replacement of lost bone due to decreased bone formation 3.
For the correct control of osteoporosis, it is important to maximize peak bone mass, preventing rapid bone loss occurring after menopause, for women, and in the elderly 4. A correct nutrition is essential for maximizing peak bone mass. In fact, nutrients as calcium, magnesium, vitamin D or vitamin K, casein peptides or isoflavones are able to determine and promote healthy bone metabolism 5,6-7. Calcium is a key nutrient for maximizing peak bone mass and the maintenance of bone mass during adult life 8,9. Milk and dairy products provide great amounts of calcium, vitamin D, phosphorus, and proteins (mostly casein), which may enhance calcium absorption and mineral retention 10. Milk and dairy products constitute about 70% of dietary intake of calcium, supporting a balance diet 10.
Regarding dairy consumption and bone turnover, previous studies have reported an improvement of bone turnover both in pre- and postmenopausal women 11,12,13,14. Moreover, previous studies also suggest that regular milk consumption is associated with an increase on bone mass density (BMD) and bone mass content (BMC). In premenopausal women undergoing secondary causes of osteoporosis, the treatment of this primary cause should be the management to increase bone health 15. However, despite the importance of prevention of osteoporosis, there is a lack of scientific literature related to dietary intervention on premenopausal women 16.
The aim of the present research was to determine the effectiveness of a diary intake of three different milky products enriched with vitamins and minerals on decreasing bone mass and bone turnover biomarkers.
MATERIAL AND METHODS
DAIRY PRODUCTS
The nutritional composition of the dairy products is displayed in Table 1. The common ingredients used for the elaboration of each one were: partly skimmed milk, milk proteins, calcium salts and stabilizers (E-450 and E-452). However, they differ in some details. CALACT60 contained vitamin D, while CALDOB54 contained five stabilizers (E-450, E-452, E-460, E-466 and E-407). In turn, CALNAT48 contained calcium salts from a different source than CALACT60 and CALDOB54, besides vitamins D and K2. The quantity of each dose of product was 250 ml.

VOLUNTEER INCLUSION
A total of 210 healthy female young volunteers were selected for the study. Finally, only 181 patients entered in the study. For inclusion in the study, female volunteers must remain in their premenopausal stage. Exclusion criteria were chronic diseases, chronic consumption of drugs, or inadequate feeding habits. Informed and signed consent of each individual involved in the trial was obtained.
Due to the homogenization of the groups, volunteers were homogenized in the three groups to study. Both the BMI and the age of all the volunteers were determined, with slight statistical variation (p > 0.05). The age of the volunteers was 39.2 ± 4.6 years old (p > 0.05). Volunteers were divided in the groups resulting in the following age-stratification: 38.9 ± 5.0 years old for the CALNAT48 group, 40.0 ± 4.8 years old for the CALDOB54 group and 38.7 ± 4.9 years old for the CALACT60 group.
Regarding weight and height, IMC of volunteers were 25.78 ± 5.1. After distribution of the groups, volunteers from CALNAT48, CALDOB54 and CALACT60 group showed IMC 25.9 ± 5.1, 27.4 ± 5.3 and 24.2 respectively.
STUDY DESIGN
The present study is a comparative trial of three dairy products fortified with calcium and vitamin D, parallel, randomized, double-blind and single-center. The study was previously approved by the scientific committee of the Catholic University of Murcia and the Ethical Committee of Scientific Investigation (ECSI). Initially, the total 181 volunteers were randomly divided into three study groups: group CALNAT48, composed by 59 subjects; group CALDOB54, composed by 59 subjects; and group CALACT60, composed by 63 subjects. However, due to the length of the treatment some volunteers left the study. Randomization was accomplished by parallel design, in which volunteers followed the treatment to which they were randomized during the duration of the trial. Therefore, the final composition of the groups was: 40 volunteers in CALNAT48 group, 34 volunteers in CALDOB54 group and 40 volunteers in CALACT60 group. The graphical distribution of the study is displayed in Figure 1.
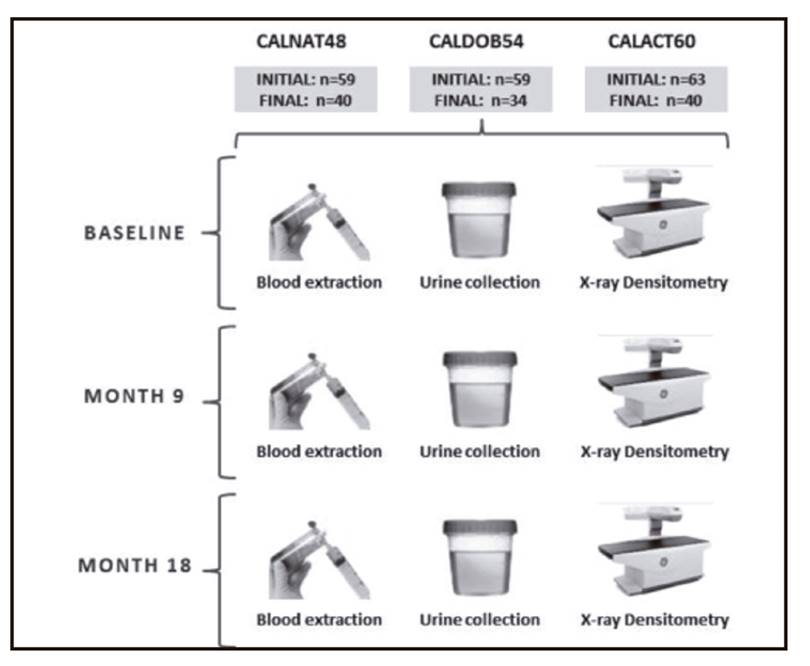
Dairy products were given to the volunteers monthly. In order to ensure compliance on study endorsement, dairy products supplying was accompanied by a food intake questionnaire. Therefore, both dairy supplying and dairy intake monitoring were repeated every month.
Volunteers from all the three groups were submitted to the same monitoring procedures, consisting on blood extraction, urine collection and energy X-ray absorptiometry (DEXA) done in the laboratory. The monitoring was carried on three times: first at month 0 (baseline), the second at month 9 (in the middle of the treatment) and, finally, at month 18 (end of the treatment).
STATISTICAL ANALYSIS
For the descriptive analysis, demographics and other baseline characteristics of the test, subjects have been described using descriptive statistical indices, for patients overall and for each of the groups studied. Continuous variables were described using measures of central tendency (mean) and dispersion measures (standard deviation). Meanwhile, categorical variables were described by tables of absolute and relative frequencies. The comparison of categorical variables was performed using the Chi-square test and the comparison of continuous variables, using the Student's t-test.
The changes from baseline in bone mineral density (DEXA values) were compared between groups using a model of analysis of variance for repeated measures: a within-subject factor (time: initial, month 9 and month 18) and a between-factor (product ingested: CALNAT48, CALDOB54 or CALACT60). The statistical distribution was accomplished by Tukey and Bonferroni, accepting a significance level minor than 0.05 (p < 0.05).
The analysis of variance for repeated measures was also used for the establishment of the differences between the different dairy products. In addition, a study of linear correlation test by Pearson linear correlation between radiological variables and the dietary intake of calcium and vitamins D and K was also carried out.
PARAMETERS STUDIED
Urinary and blood analysis
The measurement of blood and urine samples allowed knowing the concentration of different markers of bone remodeling activity and certain biochemical variables related to bone metabolism.
The blood parameters measured were: creatinine (mg/dl) by kinetic measurement; uric acid (mg/dl) by enzymatic measurement; calcemia, phosphorus and magnesium (mg/dl) by spectrophotometric measurement; bone alkaline phosphatase (mcg/l) by immunoassays; tartrate-resistant acid phosphatase (TRAP) (UI/l) by kinetic measurement; osteocalcin (ng/ml) and vitamin D (1.25 dihydroxycholecalciferol) (pg/ml) by radioimmunoassay; and intact parathyroid hormone (pg/ml) by chemiluminescence.
Densitometry analysis
Despite being clinical, analytical and radiological markers that can approximate the diagnosis of osteoporosis, the basic diagnostic tool is bone densitometry. Generally, it is developed at the lumbar (L1-L4 or L2-L4) or femoral regions (neck, trochanter and Ward's triangle). Densitometry analysis represents good accuracy and reliability (coefficient of variation: 0.5-3%, accuracy error: 3-5%), being a rapid technique that subjects the patient to very low radiation. For the determination of the densitometry values, an X-ray densitometer Norland(r) XR-46 linear beam DXA (pencil beam) was used. It was equipped by an anode stationary air-cooled tube as emitting source of X-ray, with a constant potential of 100 kV, anode current of 1.3 mA and 0.5 mm section focal point.
The parameters provided by densitometry were: BMC (g) and BMD (g/cm2). These values were expressed as mean values ± SD. The parameters were measured at the lumbar spine (L2-L4), femoral neck, trochanteric region and total hip.
Bone densitometry, in addition to measuring bone mineral density (BMC or BMD) of a particular individual in absolute and relative terms, allows comparison of population-based reference values using the T and Z scales or scores. T-score describes the comparison between individual BMC and BMD of young (20-35 years old) and healthy same-sex adults. That is, the coefficient T-score reflects the amount of bone mass of an individual regarding the maximum amount of bone mass that presents the population to which they belong. Finally, the Z-score informs about the distribution of the volunteers on the studied population. Z-score describes the comparison between individual BMD and BMD of individuals of the same age and sex. Physiologically, this value should remain constant over time. The individual changes on the bone mineral density of a patient run parallel to changes produced in the corresponding population (age and sex).
The World Health Organization (WHO), through a group of experts, establishes the densitometric criteria used as a parameter for the above-mentioned T-score. They standardized the risk of fracture, being largely accepted nowadays. It has been established that for each standard deviation decreasing the T-score of bone mass, the relative risk of fracture increases approximately 1.5-2 times.
RESULTS
Both BMI and age of all the volunteers were determined, with a very small statistical variation (p > 0.05).
BIOMARKERS OF BONE RESORPTION
In the present study, the concentration of the different biomarkers varied along the 18 months of the intervention. The differences observed varied depending on the individual biomarkers.
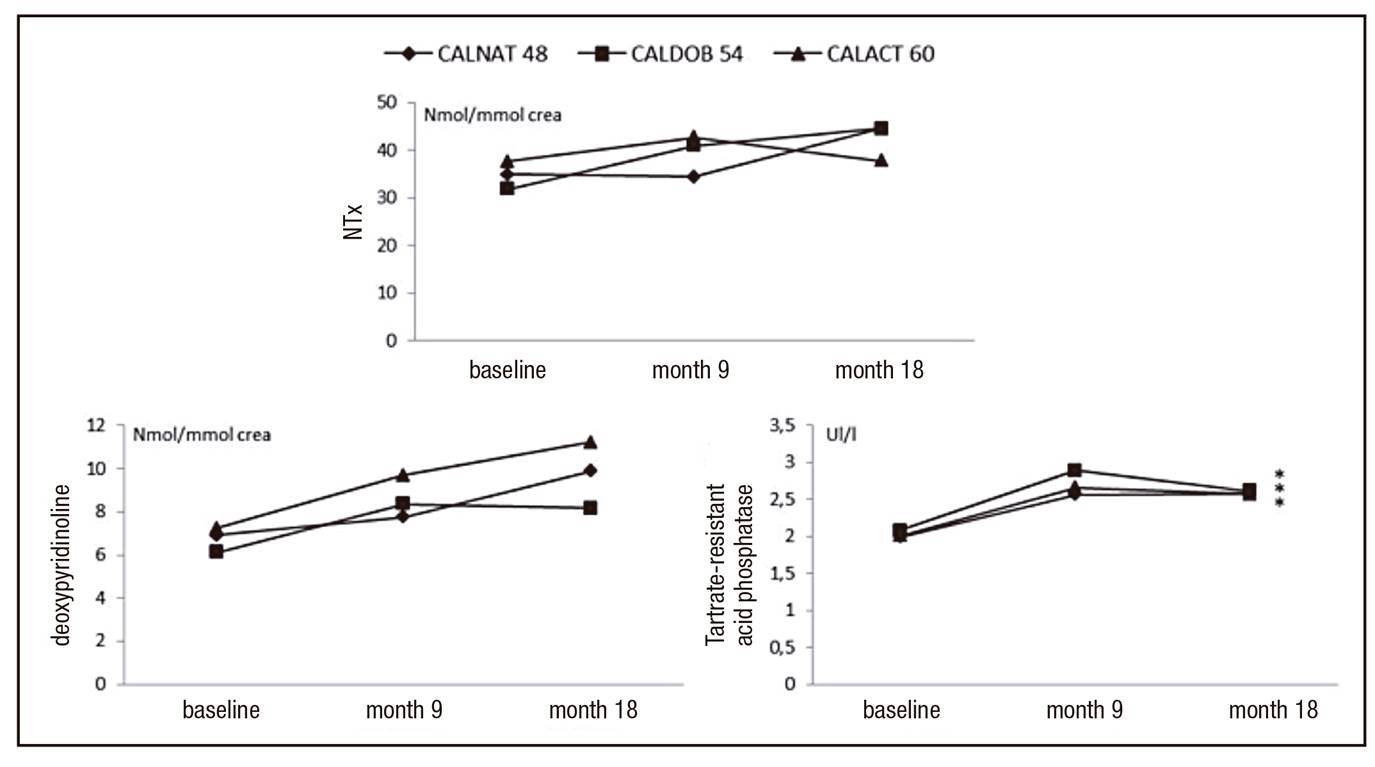
The urinary excretion of deoxypyridinoline increased along the 18 months of the study after the intake of the different beverages compared to baseline (Fig. 2). However, the changes observed were not statistically significant (p > 0.05). Similarly, the urinary excretion of deoxypyridinoline at month 9 did not showed statistically significant differences compared to baseline or month 18 (p > 0.05). Finally, no differences were observed after the intake of the different types of dairy beverages (p > 0.05).
Other compounds released during the process of bone resorption are the C-telopeptide (ICTP, CTX) and amino-terminal (NTx) collagen. They have shown a significant correlation with BMD in pre- and postmenopausal women. Therefore, CTX and NTx are considered as the most useful markers of bone resorption in clinical practice 17,18.
In turn, the urinary excretion of NTx increased after the intake of CALNAT48 and the intake of CALDO54 while decreased after the intake of CALACT60 during 18 months. Despite noteworthy, those changes in the excretion of NTx were not statistically significant (p > 0.05). Similarly, changes observed after nine months of treatment did not showed to be statistically significant (p > 0.05). As observed for deoxypyridinoline, no differences were found after the intake of the different types of dairy beverages (p > 0.05).
The most noteworthy change on the biomarkers of bone resorption was showed by plasmatic TRAP. At month 9, differences were statistically significant when compared with baseline (p < 0.05). Similarly, those differences remained statistically significant after 18 months of treatment (p < 0.05), reaching increases up to 29.5%, 20.7% and 28% after the intake of CALNAT48, CALDOB54 and CALACT60, respectively. No differences were observed between the intakes of the three dairy preparations.
BIOMARKERS OF BONE FORMATION
The values of osteocalcin did not varied at month 9 after the intake of any dairy beverage. Similarly, osteocalcin did not show an increase after the whole time of treatment (18 months). In fact, the intake of CALACT60 during 18 months derived on the non-statistically significant decrease of plasmatic osteocalcin (p > 0.05). Finally, the values observed after the intake of every beverage were similar between the different beverages.
Plasmatic level of intact parathyroid hormone (PTH-I) showed a similar trend than previously observed for osteocalcin, with non-significant differences (Fig. 3). After the intake of every dairy beverage, values of intact parathyroid hormone remained unchanged at month 9 (p > 0.05), but increased too slightly at month 18. Analyzing the evolution of alkaline phosphatase in every group of study, a non-significant increment during the first nine months after the intake of CALACT60 and CALDOB54 was found (Fig. 3). In the second half of the treatment period (from month 9 to month 18) a decrease up to initial values in this variable was observed. Only the intake of CALACT60 derived on the reduction of the concentration of alkaline phosphatase between months 9 and 18 (p < 0.05). No significant differences were observed after the evolution of the three types of dairy products during 18 months.
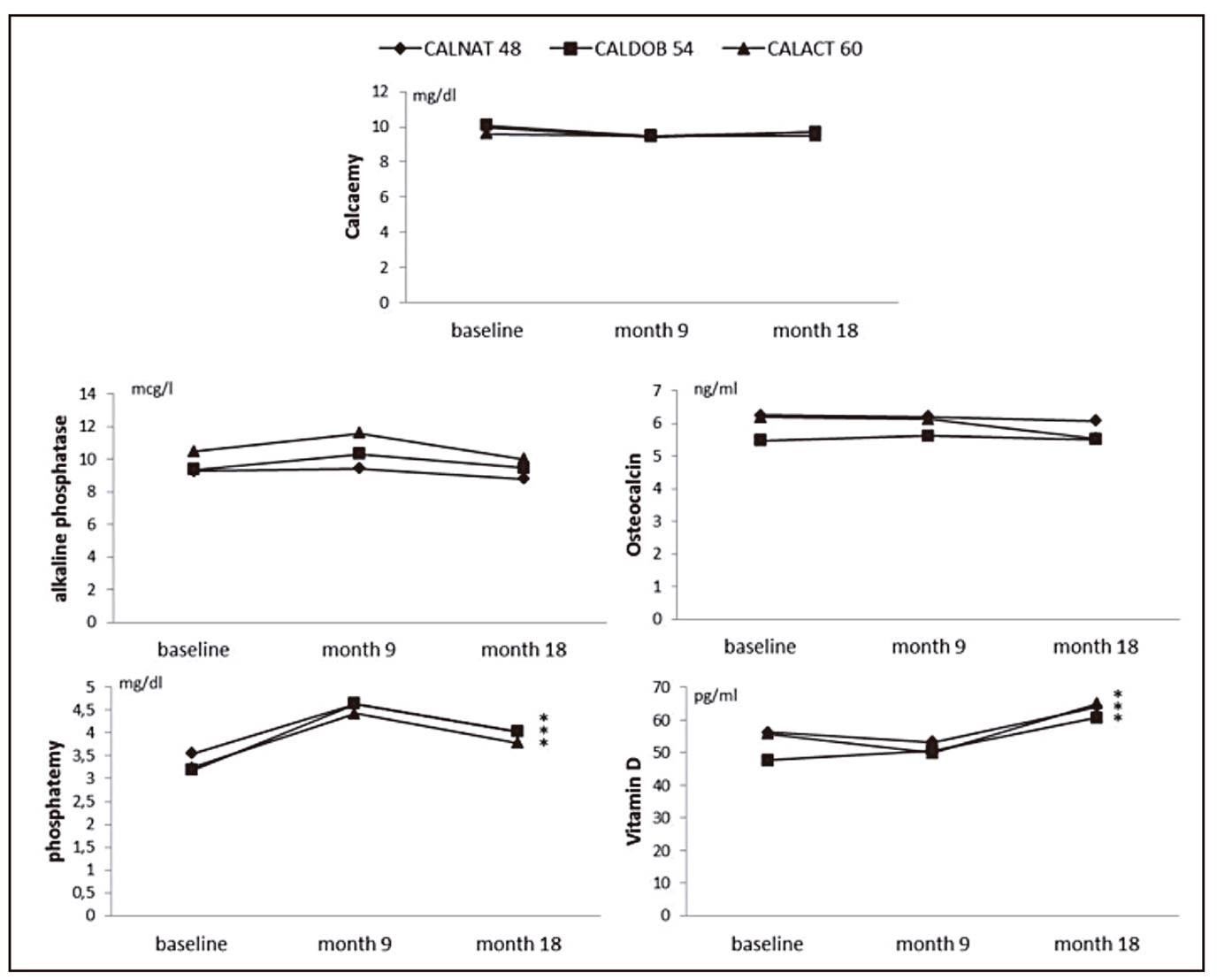
The variation observed in the plasmatic concentration of vitamins and minerals was homogenous. The evolution of plasmatic vitamin D, phosphatemia and magnesemia during the 18-month study showed statistically significant increases (p < 0.05) (Fig. 3). In turn, the evolution of calcemia during the 18 months of the study, regardless of the type of dairy beverage consumed, decreased significantly (p < 0.05). Therefore, consuming fortified milk produces an increase in plasmatic values of vitamin D, an increase in values of phosphatemia, the increase of magnesemia, and the decrease of calcemia values. Finally, the evolution of the three different groups after consuming the different types of dairy beverages for 18 months did not varied between groups.
BONE MINERAL CONTENT (BMC) AND BONE MINERAL DENSITY (BMD)
The main objective of this study was the comparative analysis of the in vivo effect of the intake of three types of dairy products, differing in their content on calcium and vitamin D. The comparison between the three types of milk in response to the changes observed in BMC and BMD in various anatomical regions during 18 months did not varied widely. Therefore, the three types of dairy product had the same effectiveness in modifying those densitometry variables, preventing or reducing bone loss.
The baseline parameters of the volunteers are showed in Table 2. The evolution of the BMC along the 18 months of treatment was different depending on the area studied. In this way, the values of BMC obtained in lumbar spine, femoral neck, trochanteric region and total hip did not follow a uniform trend (Fig. 4).

Figure 4. Bone mass content (BMC) values of the different regions evaluated for each studied group at different times of intervention. Values are expressed as g.
The results obtained after the measurement of BMC in the different locations are different depending on the measurement date. At month 9, the evolution of the BMC measured in the lumbar spine, trochanteric region and total hip did not present significant differences in any case (p > 0.05). Therefore, those volunteers belonging to the groups CALNAT48, CALDOB54 and CALACT60 showed similar BMC values when measured in these three areas at month 9. However, despite non-significant, some variations are noteworthy. The BMC measured in the lumbar spine and trochanteric region at month 9 showed increased values (p > 0.05) after treatment with CALDOB54 and CALACT60, but decreased (p > 0.05) in the CALNAT48 group. Moreover, the BMC measured in total hip showed very slight modifications (p > 0.05), decreasing after the treatment with CALNAT48 and CALACT60 and increasing after the treatment with CALDOB54. Finally, the evolution of the BMC measured in the femoral neck at month 9 showed a statistically significant decrease (p < 0.031) of 6.7% in the CALACT60 group. Meanwhile, the BMC measured in the femoral neck in the CALNAT48 and CALDOB54 groups increased in a minor extent as compared with the decrease observed in the CALACT60 group. Therefore, the evolution of BMC during the first nine months of treatment did not showed a significant decrease, except in case of the BMC measured in the femoral neck in the patients of the CALACT60 group.
The benchmark of the evolution of the three groups throughout the 18 months of treatment did not reported significant differences on the BMC compared to the values obtained at month 9 (p > 0.05). The BMC measured in the lumbar spine and total hip was quite similar after nine and 18 months of treatment with the three dairy products. Regarding the trochanteric region, the BMC of the CALDOB54 group suffered a drop, while the BMC of the CALNAT48 and CALACT60 groups increase slightly. Finally, the BMC measured in the femur neck decreased (p > 0.05) in the three groups, especially in CALDOB54.
The comparison between BMC values at baseline and those obtained after 18 months of treatment did not show significant results. The sole statistically significant decrease was found in the BMC measured in the femur neck. In turn, the BMC measured in the lumbar spine increased (p > 0.05) after the intake of CALACT60 and CALDOB54 after 18 months of treatment. Finally, the BMC measured in the trochanteric region and in total hip after 18 months of treatment remained at similar values than at baseline.
As previously observed for the study of the BMC, the evolution of the bone mineral density (BMD) did not present a uniform pattern. Baseline values are showed in Table 2.
Table II. Baseline parameters of the volunteers of the study
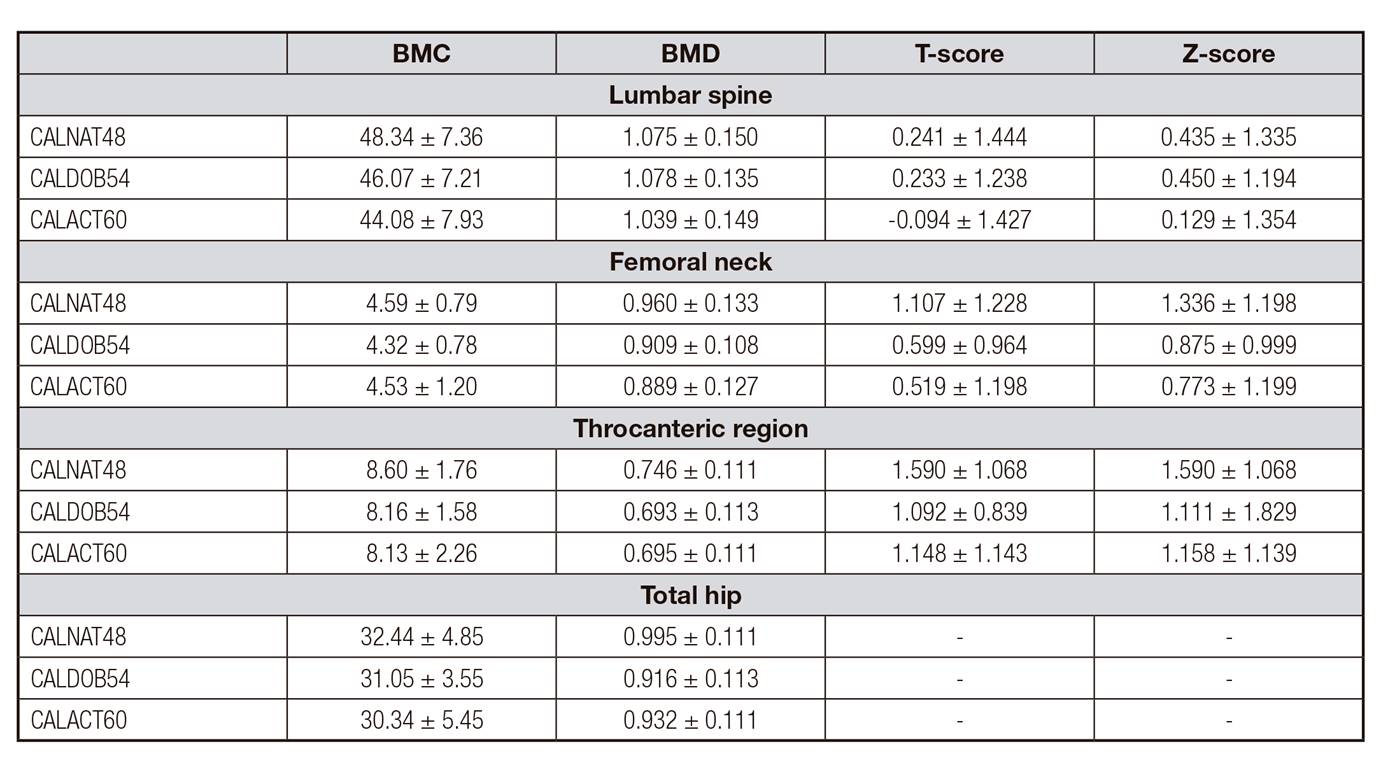
BMC: bone mineral content (g ± SD); BMD: bone mineral density (g/cm2 ± SD). T-score (units) and Z-score (units).
At month 9, the BMD observed in the lumbar spine did not show any change compared to the baseline values. However, despite being non-statistically significant, some variations were observed in the lumbar spine, femur neck, trochanteric region and total hip due to the intake of CALNAT48, CALDOB54 and CALACT60 (Fig. 5). After the intake of CALNAT48, the BMD presented a decrease of 1.1%, 1.5% and 1% when measured in the femur neck, trochanteric region and total hip, respectively. On the contrary, the intake of CALNAT48 lead to 1.2% higher values of BMD measured in the lumbar spine. The oral administration of CALDOB54 leads to a decrease of 1% and 1% when measured in the femur neck and total hip, respectively. In turn, the BMD values obtained in the lumbar spine and trochanteric region were very similar than those obtained at baseline (minor than 1%). Finally, the BMD observed after the intake of CALACT60 was 3% minor when measured in femur neck, while the measurement in the lumbar spine, trochanteric region and total hip did not show significant differences.

Figure 5. Bone mass density (BMD) values of the different regions evaluated for each studied group at different times of intervention. Values are expressed as g/cm2.
As observed before, the study of the evolution of the three groups throughout the 18 months did not report significant differences on the BMD measured in the lumbar spine, femur neck, trochanteric region or total hip (p > 0.05). However, a minor (p > 0.05) BMD was found when measured in the lumbar spine in the CALNAT48 group at month 18. Similarly, the measurement of the BMD in the trochanteric region and total hip also showed minor values (p > 0.05) in the CALNAT48 group and CALACT60, respectively. It is noteworthy that the majority of the BMD values obtained did not differ from month 9 to month 18.
The comparison between the values of BMD obtained at the end of the treatment did not differ widely from the values obtained at baseline. As a whole, the BMD measured in the lumbar spine and femur neck did not vary significantly after the 18 months of treatment, compared to the initial values. Only the CALNAT48 group showed a slight diminution in the BMD values obtained in the trochanteric region after the whole treatment. Similarly, the BMD measured in the total hip showed to be reduced in all the three groups, especially in the CALACT60 group.
T-SCORE AND Z-SCORE
The determination of the T-score was done in the lumbar spine, femur neck and trochanteric region (Table 2). The results throughout the 18 months of treatment are showed in figure 6.
At month 9, the T-score determined in the lumbar spine did not decrease in any of the groups. In fact, a slightly increase was observed in the CALNAT48 group, although it was non-significant (p > 0.05). Moreover, unless non-statistically significant (p > 0.05), some changes were observed when measured in the femur neck. The T-score determined in the femur neck showed a diminution of 0.102 units, 0.048 units and 0.107 units after the intake of CALNAT48, CALDOB54 and CALACT60, respectively. Meanwhile, the T-score determined in the trochanteric region did not decrease after nine months of treatment in the CALNAT48 group or the CALACT60 group. In turn, the CALDOB54 showed a little increment in the T-score determined in the trochanteric region.
The trend followed after 18 months of treatment was similar in all the three regions determined, showing no significant differences after the whole treatment (p > 0.05). It is noteworthy that the T-score measured in the lumbar spine was higher after 18 months of treatment than at month 9, in case of volunteers from the CALBOD54 and CALACT60 groups. Meanwhile, the CALNAT48 group showed a decrease in the T-score value compared to that obtained at month 9. The T-score determined in the trochanteric region did not vary from the middle of the treatment (at month 9) to the end of the study (at month 18) in any of the groups. The T-score determined in the femur neck followed a similar trend, without significant changes at the end of the treatment, compared to month 9.
Finally, the final conclusions comparing the values obtained at the end of the treatment with those obtained at baseline were concluding. Judging by the results, all the three beverages prevented a noteworthy drop of T-score. The final values of the T-score obtained at the end of the treatment were similar to those at baseline when determined in the femur neck and trochanteric region. Surprisingly, the T-score determined in the lumbar spine increased in the CALDOB54 and CALACT60 groups, while in the CALNAT48 group it remained at similar values than at baseline.
As occurred in T-score, the determination of the Z-score was done at the lumbar spine, femur neck and trochanteric region. The results at baseline are also presented in Table 2. Meanwhile, the evolution throughout the 18 months of the study is represented in figure 6.
At month 9, the Z-score observed in the lumbar spinal did not change significantly (p > 0.05) after any treatment, compared to baseline. However, as observed for T-score, some changes were observed when measured in the lumbar spine and femur neck. In case of the femur neck, the variation observed was a diminution of 0.078 units and 0.087 units after consumption of CALNAT48 and CALACT60, respectively. In turn, the Z-score after the intake of CALDOB54 during nine months did not suffer notable variations. On the contrary, the variation observed in the Z-score in the trochanteric region was a general increase in all the volunteers of the three groups (especially the CALNAT48 group).
After 18 months of treatment, no changes were found between beverages. The Z-score determined in the trochanteric region did not vary after 18 months of treatment, similar to that observed at month 9. The Z-score determined in the femur neck followed the same trend than that observed in the trochanteric region, showing similar values at month 18 than at month 9. The mayor changes in the Z-score after 18 months of treatment were observed in the lumbar spine. The Z-score value increased in the CALDOB54 and CALACT60 group, compared to values of month 9. On the contrary, the Z-score showed by the CALNAT48 group was minor at month 18 than at month 9.
DISCUSSION
BIOMARKERS OF BONE RESORPTION
Bone resorption can be determined by different markers, with clear differences between each one. Many markers as urinary calcium concentration can be used as a biomarker of osteoporosis. Moreover, TRAP is produced by osteoclast, being a low sensitive marker for the measurement of osteoporosis 19. However, other markers of osteoporosis as N terminal telopeptide (NTx) or deoxypyridinoline are highly specific biomarkers, being able to precisely determine the bone status 20. As previously observed by Bowen et al. 21, both NTx and deoxypyridinoline are excreted in urine, as a result of collagen type 1 destruction or degradation by osteoclasts respectively 22.
Judging by the results, the duration of the intervention period is essential for the correct determination of the action derived to the intake of dairy products. In this way the best results were obtained after 19 month of treatment, more than at month 9 (the middle of the treatment).
BIOMARKERS OF BONE FORMATION
The formation of bone tissue is crucial on bone homeostasis, and can be decisive on the development of osteoporosis 23,24. Bone formation can be determined by the measurement of many biomarkers as osteocalcin, alkaline phosphatase or intact parathyroid hormone 22,23,25. As a whole, the measurement of those biomarkers including serum vitamin D, calcium, phosphate and magnesium did not show to be determined by the intake of the dairy beverages. However, some exceptions have been noted.
Some studies have reported similar results, showing maintenance or slight reduction of PTH-I after the administration of calcium or dairy products during few months 26,27-28. In fact, the increment of calcium phosphorous ratio and the intake of protein from dairy beverages are inversely related to the increment of PTH-I in plasmatic serum 28,29-30.
Regarding the different groups, a decrease in the serum levels of calcium (p > 0.05) was appreciated, being reduced about 2.3% in the CALNAT48 group, 4.1% in the CALDOB54 group and about 1% in the CALACT60 group. The increment on the protein intake could lead to higher intestinal calcium absorption, owing to increased urinary calcium excretion 31. However, the decrease observed in the present study was minor than that observed by other researchers 21,31. Other studies reported a similar trend to the one observed in our study, showing similar values of urinary calcium in elderly men and postmenopausal women 32. That fact could be explained by a maintenance on the acid load after the intake of the dairy beverages, leading to a maintenance on the urinary excretion of calcium 33.
Performing benchmark in the evolution of the three different groups after consuming the different types of dairy beverages for 18 months, no significant differences were observed between groups (p > 0.05). Similarly, phosphatemia levels increased (p < 0.05) in the CALNAT48 group (13.5%), the CALDOB54 group (26.5%) and the CALACT60 group (16.4%). Finally, magnesemia also increased (p < 0.05) after the intake of CALACT60 (6.1%), CALNAT48 (8.6%), and CALDOB54 (6.2%).
When analyzing the evolution of plasmatic vitamin D in each of the study groups, it was appreciated a significant increase of 27.3% in the CALDOB54 group (p < 0.05), 14% in the CALNAT48 (p < 0.05) group and 16.7% in the CALACT60 group (p < 0.05). Other studies have reported descend on the plasmatic concentration of vitamin D 18,34, due to the lack of long-term sun days in winter, not related to the intake of dairy products. All the beverages containing vitamin D increased the concentration of that biogenic amine on serum, even the CALDOB54 with minor concentration of vitamin D. Therefore, the increment of vitamin D in serum seems to be influenced by other factor, such climatic conditions, apart from the intake of exogenous vitamin D.
The results obtained in the present long-term interventional study reveal that the acutest effects were detected after 18 months of treatment. Meanwhile, the consumption of dairy products for nine months showed minor influence on the variation of calciotropic hormones and bone resorption biomarkers. Therefore, changes observed in the concentration of the different molecules indicate that long-intervention periods might be necessary in order to reach significant differences in the variation of bone remodeling biomarkers.
BONE MINERAL CONTENT (BMC) AND BONE MINERAL DENSITY (BMD)
Most clinical trials concerning the efficacy of different products for the prevention or treatment of osteopenia and osteoporosis use bone mineral content and bone mineral density as primary variables 35. Increased values of BMD about 1.5% can be understood as beneficial for the bone maintenance and maximized peak bone mass in young volunteers. For example, Uenishi et al. (36) reported increased values of BMD of 1.57% after consumption of a dairy product compared to placebo (0.3%). As commented before, some nutrients from dairy products can be beneficial for the treatment or prevention of osteoporosis. Calcium, phosphorus or vitamin D can determine the effectiveness of milk and dairy products in the treatment of oleuropenia and osteoporosis 4,23,35.
The determination of BMD and BMC after nine months of treatment did not show significant changes after the intake of any of the dairy beverages. Therefore, the acute treatment with dairy products could not be enough to exert beneficial effects on BMD or BMC. In fact, the different studies carried out with dairy products on the BMD and BMC content have a length of several months 7,36,37. However, other studies reported healthy benefits after few months of treatment with dairy products, as Uenishi et al. 36, who found increased values of BMD after six months of treatment in young female volunteers.
The evolution of BMD and BMC during the 18 months of intake was different depending on the region studied. In case of BMD measured in the lumbar spine, no significant changes were appreciated, so BMC did not show a significant increase. In other anatomical locations, both BMC and BMD showed a decrease ranging between 0.5% and 1.5%. Contrarious to premenopausal and postmenopausal women who suffer an unavoidable loss of bone mass and bone mineral density, the BMD of young population, as adolescents, increases until reaching their maximum bone peak 2,4,9. Previous researchers have shown that increment even in control patients administering placebo product, instead of dairy products 38,39. Toheed (2016), in a study with postmenopausal rural women, recently reported that more than half of the women had either low BMD or osteoporosis, significantly related to low intake of milk and milk products 40. The results obtained in this study are similar to those observed in other studies of similar characteristics, based on the consumption of mineral- and vitamin-enriched milk, reducing the loss of bone mass 41,42.
T-SCORE AND Z-SCORE
The evolution of the Z-score throughout the whole study showed different tendencies, regarding the location of the measurement. The Z-score of the trochanteric region remains at similar values than that observed at baseline. Meanwhile, the determination of the Z-score in the femur neck showed a tiny decrease compared to baseline parameters. Finally, the Z-score determined in the lumbar spine showed an increase at the end of the treatment in all the volunteers of the three groups, being statistically significant in the CALDOB54 group (p < 0.05).
Therefore, consumption of fortified dairy products produces a positive effect in the Z-score values. Their consumption prevented the decrease of that parameter and even increased when it was measured in the lumbar spine.
The analysis of the T-score and Z-score provides clarifications to the above conclusions. The T-score and the Z-score determined in the femur neck and the trochanteric region showed no or slight differences compared to baseline, which indicates the capability of reducing bone loss. Noteworthy, the T-score and the Z-score determined in the lumbar spine increased after the treatment with the three types of dairy products. Specially, the intake of CALDOB54 was able to increase both the T-score and the Z-score (Z-score in a statistically significant way). Therefore, for the lumbar region, increases achieved in these scores confirm the results obtained in other studies 42. In the femoral region (neck and trochanter) results are different; intake of different types of milk had no effect improving bone mass in this region, delaying bone loss. These results are comparable to those of other studies, reporting mayor changes for the lumbar spine than in the femoral region 42,43-44.
Despite carrying out the present investigation in the best possible way, the article presents some limitations. The development of the study is parallel, since the crossing of the groups is not possible for obvious reasons. The menstrual status of the volunteers was not uniform throughout the study, given the personal variability of each one, and the age difference between them.
Regarding parameters, evaluated densitometry reports bone mineral density, but not bone architecture. In addition, bone density is different in each location, so only a relative correlation between the results of the different measurement points can be evaluated. Therefore, results of densitometry provide information of the location where it was performed and should always be performed in the same location. Finally, given that densitometry results should be assessed for prediction of fracture risk, bone density is a major determinant of fracture risk. However, there are other fracture risk factors not associated with bone fracture.
CONCLUSIONS
In summary, the development of bone loss gets delayed along the different treatments. The intake of the three dairy products enriched with calcium and vitamin D for 18 months improves bone mass in the lumbar spine more than in the lumbar region. However, no differences in efficacy were obtained when comparing the three types of dairy products. Changes observed in the concentration of the different biomarkers indicate that long-intervention periods seem to be necessary for the disparity of bone remodeling biomarkers. Especially, tartrate-resistant acid phosphatase seems to be strongly influenced by the intake of every dairy product. However, the differences observed between the different dairy products were not remarkable, which shows that none of the micronutrients studied is more important than another for the prevention of the disease. Therefore, the intake of dairy products leads to a less enhanced bone resorption in premenopausal women (regardless of the product supplementation), which is determinant for the prevention of osteoporosis.

