










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkIntroduction
It is imperative that children are encouraged to engage in healthy behaviours in order to reduce the possibility of the occurrence of physical and psychological challenges as they develop into adulthood. For example, obesity in early years often persists into adulthood (An et al., 2009) and has been associated with the later emergence of psychological difficulties such as heightened depressive mood, body image problems and low self-esteem in adolescence and adulthood (Antwi et al., 2012; World Health Organization, 2014). Given the persistence of these problems following childhood, a number of authors have suggested that 14 years is the critical age for specific interventions for eating-related problems up until which long-lasting change on eating behaviours can be achieved (Rohde et al., 2015). Indeed, according to the DSM-5, the peak age of onset of eating disorders is between 14 and 20 years (American Psychiatric Association (APA), 2014), with most primary prevention programmes being aimed at elementary school children below this age (Piran, 2005). Kitzmann et al. (2010) found that the expectation that parents would change their own behavior was key in the outcomes of treatment. They found a significant association between the role of parents and enhanced weight control results in their children, who were aged 6 to 12 years and overweight. Moreover, outcomes were better when parents had been trained in nutrition and healthy cooking. In this regard, Roberts (2010) conducted a review of vicarious learning with university students. He found that students learned through experiential learning from talk and storytelling.
Life stories, or the narratives through which people connect their past experiences to the present (McAdams, 2001), play an important role in the health and well-being of an individual (Singer, 2005). These experiences have been unified and given global meaning through their integration into one’s beliefs about oneself (McAdams, 2001). Several studies have shown that past experiences which have marked an individual’s life are combined with future expectations and life goals and are used to characterize their beliefs about themselves (Freeman, 2007; Habermas & de Silveira, 2008; McAdams & Manczak, 2015; Singer et al., 2013). The extent to which one then plans for and engages in healthy behaviours is likely to be determined by one’s previous healthy experiences, one’s memories for these experiences and the extent to which they are integrated into one’s definition of oneself (Buceta et al., 1996). As such, difficulty integrating past experiences into one’s present sense of self has been found amongst people who engage in unhealthy behaviours, such as those with eating disorders (Amianto et al., 2016).
Young people’s early health-related experiences that later shape their health-related beliefs about themselves are, to a large extent, influenced by their parents’ behaviours (Singer, 2004). Memories for these self-defining past experiences have been referred to as Self Defining Memories (SDMs). According to Singer (2005, p. 22) “Self-defining memories are those memories that help you to define most clearly how you see yourself and that help explain who you are to another person”. SDMs lend unity, coherence and stability to a person’s experiences, interacting with the self throughout our lives. Children begin to form their narratives or life stories based on their relationship with their parents, who provide feedback on these stories (Fivush, 2001) and who help to build and consolidate their children’s narratives through interaction (Pasupathi & Wainryb, 2010; Singer, et al., 2013). Children and adolescents therefore construct their narratives under the influence of their family and their immediate environment, as well as social and cultural influences and they use them as a means of affirming who they are (Singer, 2005). The development of these social stories is key during adolescence, and in the development of one’s own identity (Habermas & Bluck, 2000; Habermas & de Silveira, 2008). It has been observed, for example, that mothers, and women in general, place more emphasis on the emotional integration of memories (Pasupathi & Wainryb, 2010). Through conversations and relationships with their children, mothers help build narrative memories during their childhood (Reese & Robertson, 2019). Regarding the integration and elaboration of narrative memories, the fact that mothers elaborate these more is related to how children elaborate their own memories (Fivush et al., 2006; Fivush & Nelson, 2004).
Singer (2005) described five key elements that underpin SDMs: emotional intensity, vividness, repetition, connections to similar memories and a focus on lasting goals or unresolved conflicts. Thus, SDMs tend to be frequently and vividly recalled, leading to a reliving of intense emotions and are connected to other memories involving the same topic (Lardi et al., 2010). Several autobiographical memory researchers have suggested that experiences in adolescence and early adulthood are loaded with importance and are strongly linked to the construction of self (Lardi et al., 2010; McLean & Thorne, 2003). Beyond adolescence, Kingsford, Hawes and Rosnay (2018) drew attention to middle childhood in the development of the self. Specifically, these authors reviewed the development of the moral self. SDMs activate associations with other similar memories or those involving the same topic, making these types of memories more accessible. Thus, SDMs linked to a healthy self could be associated with a set of healthy habits which have significance for the individual. The generation of SDMs has been associated with healthy beliefs, and such behaviours may therefore help individuals to establish central health-related goals. As SDMs characterize one’s identity (Blagov & Singer, 2004; Lardi et al., 2010; Singer, 2005; Singer & Salovey, 1993), it could be that a healthy self may be underpinned by health-related SDMs and the phenomenological variables they involve.
The importance of the first years of youth to strengthen healthy habits has been demonstrated (Huéscar et al., 2014), as well as the relationships between peers in middle childhood are of particular importance for development (Maunder & Monks, 2019). Continuing with the importance of psychosocial exchanges in the learning process, Harris (2014), after analysing the work of physical education teachers with young adolescents, concluded that these interactions are essential in any physical activity programme. The environment and family practices are essential to develop habits such as the consumption of fruits and vegetables. Wyse, Wolfenden and Bisquera (2015) analysed which specific practice carried out by parents is related to the their preschool children’s increased consumption of fruits and vegetables. They found that the variables that most influence the increase in this habit are parents consuming these products and providing them at home. The observation and interaction with others may determined the health beliefs we acquire and the extent to which they become integrated into our characterization of ourselves. Relatedly, several research teams have suggested that parental (Gallota et al., 2016; Kitzmann et al., 2010) and peer (Hernán et al., 2001) involvement in health-related interventions can subsequently influence the extent to which children acquire healthy habits and continue to adhere to them.
The association between narrative memories and well-being, psychological adjustment or physical health has been corroborated (McLean et al., 2010). Well-being and self-development are connected, either through motivations, the integration of the self or the maturation shown in narratives, for example (Bauer et al., 2008). Mood has also been connected to the memory affectivity (Boyano & Mora, 2015). In previous studies, variables of the SDMs have been linked to well-being or health, (e. g.: Blagov & Singer, 2004; Lardi et al., 2010; Sansom-Daly et al., 2016). For example, higher psychological well-being has been related to narrative memories narrated more related to achievements, which are central to SDMs. It has been found that, by encouraging young adolescents to retrieve narrative memories related to their fathers, their self-esteem was significantly linked to more use of subjective terms in stories about their mothers (Chen et al., 2021). Blagov and Singer (2004) found a connection between the psychological well-being or social adjustment of individuals with the affect they show in their narratives. Continuing with particular aspects of SDMs, Moffitt and Singer (1994) found people whose SDMs are developed around their attainments showed more positive affect about these memories
Regarding the association between SDMs and aspects of health, higher health anxiety levels have been associated with the retrieval of SDMs that were particularly negative (Sansom-Daly et al., 2016). The authors suggested that participants with high levels of health anxiety attributed greater value to negative beliefs about themselves and about illness/death, in line with previous results of Wells and Hackmann (1993).
Despite this association, to our knowledge, no study has examined the association between health-related self-defining memories and people’s health-related behaviours.
Given the importance that early experiences and behaviours can have on later health-related behaviours, this investigation therefore sought to analyse the association between the phenomenological characteristics of children’s health-related SDMs (HSDMs) e.g. their vividness, importance, and their engagement with healthy habits.
The present study
The present study examined the association between the features of the HSDMs retrieved and the places and people associated with them in order to examine how memories for different kinds of experiences and involving different people are differentially associated with health-related behaviours. We also examined the extent to which HSDMs differ from more general self-defining memories.
We proposed the following hypotheses: 1) that children whose HSDMs rated as most vivid, important and positive would show more frequent healthy habits; 2) that children with more healthy habits would include a higher frequency of health situations experienced in the presence of their parents, especially those with their mothers, in their retrieved HSDMs.
Methods
Participants
In order to conduct this study, we collected information from 262 children. These children were enrolled in five urban schools. They were from medium socioeconomic status communities. They were recruited to participate in a study regarding their health habits. The inclusion criteria were being enrolled in fifth or sixth grade of elementary school, parents’ having signed an informed consent form, and agreeing to participate voluntarily. The exclusion criteria were being children with specific educational needs or presenting a significant learning gap, with reduced reading and writing skills. During initial recruitment, 277 participants were initially identified, but a further 15 were excluded because of severe learning difficulties or educational delay as characterized by their local school counselling teams. The mean age of participants was 11.33 years (SD = 0.68), range from 9 to 13. Boys accounted for 50.4 % and girls 49.6 % of participants. A total of 49 % of participants were 5th graders and 51 % were 6th graders.
Materials
Sociodemographic questionnaire
Participants were required to give information on: date of birth, place of birth, gender, persons with whom they reside, number of siblings (including the participant), father’s occupation, mother’s occupation, medication, illnesses and /or operations.
Self-defining memories task
An adaptation of the task designed by Singer and Blagov (2000) was administered. The children were asked to recall a health-related self-defining memory (HSDM). They were given instructions about the nature and features of SDMs: A self-defining memory has the following characteristics: 1, it’s at least one year old; 2, it refers to an event in your life that you remember very clearly and that still feels important to you even as you think about it; 3, it’s a memory about an important, enduring theme, issue or conflict from your life. This memory helps to explain who you are and might say something more about you if you wanted someone to have a deeper understanding of you; 4, it’s a memory linked to other similar memories that share the same theme or concern; 5, the memory may be positive or negative, or both, depending on how it makes you feel. The only key thing is that it leads to strong feeling; 6, it’s a memory you have thought about many times. It should be familiar to you, like a picture you’ve studied, or a song (happy or sad) that you’ve learnt by heart. To better understand what a self-defining memory is, imagine that a new boy or girl has just arrived at school and you begin to talk and make friends. You want your new friend to know you exactly as you are, to know the “real you”, so you show yourself as you are. You don’t try to play a role or strike a pose. While, inevitably, we sometimes say things that present a picture of ourselves that might not be completely accurate, imagine you are making every effort to be honest and sincere. During the conversation, you describe a memory you feel powerfully conveys how you came to be the person you are now. It is this memory, which you tell the other person while repeating it to yourself, that forms a self-defining memory. Then they were told: Please, go back and recall a Self-Defining Memory related to HEALTH. You have to remember a Self-Defining Memory that defines your identity and who you are with regard to health (your health behaviours, your attitudes towards health, how you define yourself compared to another person with regard to health …). Could you please write a description of the memory?
In the same way as the task designed by Singer and Blagov (2000), after writing down each HSDM, on a Likert-type scale (where 0 is not at all and 6 is extremely) participants rated the extent to which each HSDM evoked the following feelings: happiness sadness, anger, fear, surprise, shame, disgust, guilt, interest, embarrassment, contempt, pride. We conducted an exploratory factor analysis extracting two factors to verify the emotional valence (positive or negative) of the affects scored by the children in this study. The factor analysis of the different affects evaluated by the participants for their HSDMs established happy, interested, surprised and proud as positive affects and sad, angry, fearful, disgusted and guilty as negative affects. Based on this factor analysis, we established the categories of positive affect and negative affect with the mean scores for the affects in each category. Following the same scoring system, the children rated the vividness of the memory (how well they recalled the memory) and the importance they attached to it. They were also asked to write down how old they were when the event took place, where they were and who they were with.
Healthy Habits Questionnaire
This questionnaire, based on the questionnaire for minors from the National Health Survey (2011-2012), designed by the Spanish National Statistics Institute and the Ministry for Health, Social Services and Equality (2013), collected information on: the time the children go to bed and wake up, the physical activity they do during their leisure time and extracurricular activities and the frequency with which they consume different foods throughout an average week.
Procedure
The study was approved by the local Clinical Research Ethics Committee (Record Nº 10/2016 of the CEIC). Following the exclusion criteria, children in the groups where the tests were administered who had specific educational needs or presented a significant learning gap, according to the school counselling team, were not invited to participate in the study.
Before collecting the participants’ data, their parents signed an informed consent form authorizing their children to participate in the study. The form underlined the voluntary nature of participation in the study. The researchers undertook to treat the data collected confidentially, ensuring anonymity in the event of communicating the results. In the lists used for analysis, only randomly assigned codes would appear.
The children answered the questionnaires and completed the memory tasks in pencil and paper format after being given spoken instructions in group sessions. The children answered at their own pace in class, accompanied by their class teacher or another teacher from the school or a member of the research team responsible for administering the tasks and individually dealing with any problems arising during the sessions. The children whose parents declined to participate continued with their normal school work.
Three independent raters, studied and trained the criteria of categorization according to (Blagov & Singer, 2004) and to (Singer & Blagov, 2000). The team categorized individually a part of the memories that participants had remembered, HDMs and general SDM (without instruction to be a memory about health) too. Cohen´s k equal to 0.69 was found in the categorization of true, and Cohen´s k is equal to 0.72 in the categorization not SDM.
Data analysis
First, descriptive analyses were conducted on the frequencies of eating habits and physical activity from the Healthy Habits Questionnaire and the characteristics of the children’s HSDMs (themes, actors and places). A general index of health was created. This index was formed of three sub-indices of health: healthy diet, physical activity and sleep. The first two indices were scored from 0 to 1 and the sleep index was scored from 0 to 3. To calculate the index of healthy diet the frequencies of consumption of healthy food were added (fruit, vegetables, fresh fruit juice, legumes, dairy products, meat, eggs, fish, pasta, potatoes, rice, bread, cold meats, sweets, sugary soft drinks, fast food, and salted snacks). Each food consumed with an appropriate frequency according to the Spanish Agency for Food Security and Nutrition (García & Muñoz, 2007) added .067 points to the index. To calculate the index of healthy physical activity, participants received .5 points if they engaged in physical activity as an extracurricular activity during school time and a further .5 points if they engaged in physical activity during their leisure time. The index of healthy sleep added 1 point when the children slept the appropriate time, between 8 and 10 hours (Aznar & Webster, 2006). Therefore, a higher score indicates greater incidence of healthy behaviours.
As we detected a non-normal distribution in these indices, correlational analyses between the phenomenological variables that support HSDMs and general SDMs (vividness, importance and affect) and the health indices were performed using Spearman’s correlation coefficient. The Wilcoxon test was used to analyse the differences between the phenomenological variables of the SDMs and the HSDMs.
The Mann-Whitney U test was used to assess the differences in phenomenology (vividness, importance, and affects/emotions) according to whether the HSDMs were related to events experienced with children’s mothers or fathers compared with other persons. The Kruskal-Wallis test was used to analyse whether the importance, vividness and positive and negative affect qualities attributed to the HSDMs varied according to the places the children were and the persons they were with when the events occurred.
Results
Descriptive Data on Healthy Habits
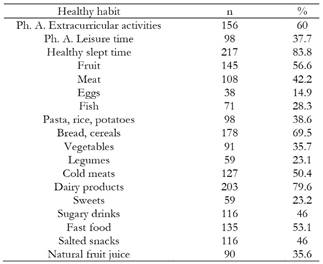
We found that 156 participants (60 %) took part in extracurricular physical activities and 98 (37.7 %) engaged in physical exercise during their leisure time. Data on the frequency and percentage of healthy habits can be found in Table 1.
HSDMs features
Of the 262 participants, 241 retrieved HSDMs in the SDM task as requested in the instructions. The remaining 21 either wrote nothing in this part of the task, or wrote a narrative that cannot be considered a memory (for example: I eat fruit every day, the food I eat has little fat and sugar because my mother and sister have high cholesterol, so I take care of my health). Some examples of a HSDMs are: “A day when I got ill in my village; or I went swimming last year and when I got out of the pool I was pushed, fell and broke my ankle. I had to rest so that when it healed, I could swim again; or when my mother was told she had kidney stones and she started eating healthier. since then I eat better too”. The mean self-reported age of the children when the event in the 241 retrieved HSDMs occurred was 7.26 years (SD = 2.58). The mean score for vividness and importance of the memories was M = 4.92 (SD = 1.48) and 4.46 (SD = 1.85), respectively. Mean Positive Affect attributed to the HSDMs was 2.48 (SD = 1.84) and mean Negative Affect was 1.26 (SD = 1.41).
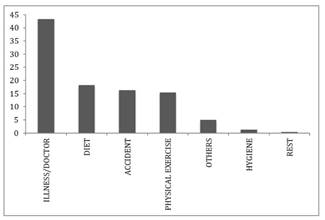
Themes in the HSDM narratives
The themes of the HSDMs were categorized as: diet, physical exercise, hygiene, rest, illness/doctor/accident. A residual category was defined for the memories that could not be classified into any of those above (for example: I was five years old. My parents were drinking whisky and went up for a nap, there wasn’t much left so I drank a bit and started to feel sick, but a minute later I felt better.). Graph 1Graph 1 shows the data on the frequency and percentages of these themes.
Differences between HSDMs and SDMs
The Wilcoxon test showed significant differences between positive affect, vividness and importance between HSDMs and general SDMs. Compared to HSDMs, general SDMs were reported as significantly more associated to positive affects scores: z = -7.04, p < .001 (mean general SDMs = 3.58, Sx = 1.70; mean HSDMs = 2.50, SD = 1.83); vividness score: z = -3.19, p = .001(mean general SDMs = 5.27, SD = 1.12; mean HSDMs = 4.93, SD = 1.52); importance score: z = -6.20, p < .001 (mean general SDMs = 5.33, SD = 1.29; mean HSDMs = 4.49, SD = 1.86). Non-significant differences were found for negative affect scores.
Association between HSDMs and healthy habits
A total of 38.2 % of the children who retrieved HSDMs engaged in physical activities in their leisure time, and 61.3% attended extracurricular physical activities. Of these children, 85% slept between 8 and 10 hours a day, within the recommended guidelines for childhood (Aznar & Webster, 2006). Table 1 shows the frequency and percentage of healthy habits of the children as well as the frequency with which the schoolchildren consumed different foods. Correlation analysis did not find significant results between the phenomenological variables that HSDMs and the health indices.
HSDMs locations
Table 2 shows the frequency and percentage of places where HSDMs occurred. To calculate the Kruskall-Wallis test we re-categorized the places that the children associated with their HSDMs in the following variables: at home, at the doctor’s or hospital, at school, at the grandparents’ house, and other places outside the home, but where no specific place was mentioned. The Kruskall-Wallis test revealed significant differences between the place where the children situated the HSDMs and the negative affect associated with them (H (4 df) = 11.57; p = .021). The post hoc pairwise comparisons showed significant differences between the negative affect generated by the HSDMs on events outside the home compared to those situated at home (H = 29.39; p = .033). The mean negative affect score for HSDMs situated at home (M = 1.46, SD = 1.37) was higher than that for those occurring away from the home (M = 0.95, SD = 1.3). Importance and vividness were not related to HSDMs places.
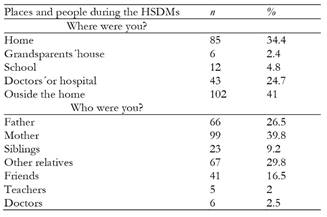
The people present in HSDMs
Table 2 shows the frequency and percentage of HSDMs that referred to particular people who the children were with during their HSDMs. According to the Mann-Whitney U-test, the HSDMs featuring the mother were reported as significantly more important than those in which she was not involved (Mann-Whitney U score = 5.543,5 z = -2.44, p = .015). The mean of importance scores for HSDMs in which the mother was present were higher (M = 4.79, SD = 1.71) than for those in which she was not present (M = 4.24, SD = 1.93). A Kruskall-Wallis test was performed where the people that the children associated their HSDMs were recategorized as follows: direct relations, the mother, the father, friends, siblings, the mother, the father, friends, siblings, other relatives, doctors and teachers. Using this coding system, the Kruskal-Wallis test did not show significant differences between the self-reported scores for importance, vividness and positive and negative affect of the HSDMs based on who they were associated with.
Discussion
The children in our study retrieve more HSDMs related to home and their mothers than in other places and with other people. Moreover, the importance of the HSDMs associated with mothers are scored more highly than other HSDMs. This finding is in line with the recognized influence of family in the construction of children’s narrative memories (Singer, 2005), and how these form part of the integration of a person’s past and present in the development of the self (McAdams, 2001). It may be that sharing with loved ones the events that children will later recall as associated with health helps to internalize health information and healthy habits, either as a result of emotional connection, instruction or modeling. It has been proven that mothers participating in the construction of childhood memories with their children influences their recovery of earlier memories of their childhood (Reese & Robertson, 2019). As discussed in the introduction, children learn to organize and elaborate their memories based on the interactions and modeling of their close adults. In this sense, children whose mothers have built more elaborate autobiographical memories will also present more elaborate memories (Fivush et al., 2006; Fivush & Nelson, 2004). Moreover, the mothers’ use of a more elaborate language, or the act of alluding to internal or contextual experiences when retrieving narrative memories is related to the way in which their children construct theirs (Fivush, 2008).
It would be necessary to take more account of the period of middle childhood in research on the development of the self, which traditionally has not been very much taken into account (Kingsford et al., 2018). The mean age at which the participants in the current study situated the events in their HSDMs was 7.26 years, which is consistent with the idea of that these early years play and important role in shaping health behaviours. This also suggests that introducing intervention strategies in childhood focused on experiential and significant health experiences. For this it would be necessary to train families in the involvement in active healthy activities with their children. It would be useful to consider this when designing intervention to create and promote learning experiences and the internalization of healthy habits and protective health beliefs in contexts that are close to them (e.g., leisure time activities, school time, neighborhood...).
The children recovered their HSDMs after asking them to remember intense and important memories related to their identity and beliefs regarding health. What we observe is that even valuing these memories as intense, vivid and important, they are not as important as their general SDMs. HSDMs share phenomenological characteristics with general SDMs, although to a lesser extent. Since the SDMs can be taken as a reflection of the identity of the individual, we assume that what happens is that children, whose identity is under construction, do not have sufficiently internalized beliefs and connections of health with themselves during this pre-teen stage. This suggests that it may be necessary to further strengthen the internalization of health habits and beliefs by children. We can hypothesize, then, a correct diet with well-chosen foods and cooking methods is the key starting point for health promotion interventions in children. From there, correct diet can be linked to other habits, so that both the former and the latter serve as guidelines and reinforcement. Recommended dietary guidelines can be found in numerous institutional guides on childhood nutrition (Spanish Agency for Food Security and Nutrition, 2010; Bartrina et al., 2016; García & Muñoz, 2007). The way they score the phenomenological variables of their HSDMs is coherent with the way they behave. This coherence forms part of the construction of one’s self, based precisely on the development of SDMs (Singer, 2005). This coherence was found, for example, in a sample of more than 5,000 adolescents, in which those with unhealthy weight control behaviours exhibited higher levels of negative affect. In girls, this negative affect was lower among those with healthy weight behaviours (Vander Wall, 2011). Various authors recommend initiating prevention of eating disorders at early ages (Gumz et al., 2017; Nicholls et al., 2011). Aiming to identify how weight stigmatization influences body satisfaction and eating behaviours in preadolescent children aged from 6 to 11 years, Jendrzyca and Warschburger (2016) highlighted the importance of conducting programmes for high-risk eating behaviour prevention and early detection of dysfunctional eating behaviours to prevent these types of disorders. Furthermore, not only is it important to implement programs at an early age, but also to take into account the role of families and the social environment (Gallota et al., 2016; Kitzmann et al., 2010; Roberts, 2010; Wyse et al., 2015).
Conclusion
The importance of the present work lies in the study finds descriptive data about phenomenological variables in the HSDMs of children and its connection with their families, especially with their mothers. As mentioned above, these phenomenological variables are not as intense as general SDMs. This suggests it would be appropriate to encourage children to healthy experiences that are meaningful to them and can permeate the development of their HSDMs and their self. Our conclusions provide starting points on which to design strategies to promote healthy beliefs and habits in children during the stage of primary education. It would be appropriate to begin working with children and their families at around the age of 7 years, so that their beliefs and habits generate positive HSDMs as a basis for the development of healthy behaviours and beliefs that increase the development of an adequate self about health and self-care.
This study would have benefited from objective measures of the children’s state of health. A methodological limitation of the work might be that we did not counterbalance the order of administration of the questionnaires. In future studies, the information analysed in this work could be complemented by objective data on health such as the children’s body mass index or asking participants about the satisfaction they feel when engaging in physical activities or consuming healthy food. The data on healthy habits followed by the children were collected by self-report. Future research should contrast this data with those provided by their mothers and fathers or those acquired through observation.
From the differences between general SDMs and HSDMs, it is unclear whether the memories recovered by the children are true self-defining memories. since one of our objectives was to analyse the relationship between remembered HSDM and healthy habits in children, this sets us apart from our goals.
In any event, this study provides information on SDMs in children, and their association with behaviour. The findings presented here suggest that enhancing the positive affect with which health-related self-defining events are experienced or the way in which memories for these experiences are later retrieved could contribute towards engagement in more healthy behaviours.
Diclosure Statement: No potential conflict of interest was reported by the authors.

