










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versão impressa ISSN 1130-0108
Rev. esp. enferm. dig. vol.108 no.6 Madrid Jun. 2016
LETTERS TO THE EDITOR
En bloc endoscopic submucosal dissection for a giant neoplastic lesion in the duodenal bulb
Key words: Endoscopic submucosal dissection. Duodenal neoplasm. Duodenal bulb.
Dear Editor,
Endoscopic submucosal dissection (ESD) of duodenal neoplasm is technically difficult for the tortuous lumen and thin wall. This letter describes a case with a giant neoplastic lesion in the duodenal bulb, which was en bloc resected by the ESD technique.
Case report
A 71-year-old man presented to our hospital for surgical treatment of a duodenal lesion found accidentally 8 months ago during health examination. There was no family history of gastrointestinal cancer. Physical examination and laboratory data were not remarkable. Esophago-gastro-duodenoscopy revealed a wide-based, nodular, polypoid lesion, which was mainly located at the front wall of the duodenal bulb with superficial erosion, involving 2/3 of the duodenal bulb circumference (Fig. 1A). Endoscopic biopsy showed moderate to severe dysplasia of glandular epithelium. Magnetic resonance imaging showed no organ and lymph node metastasis.
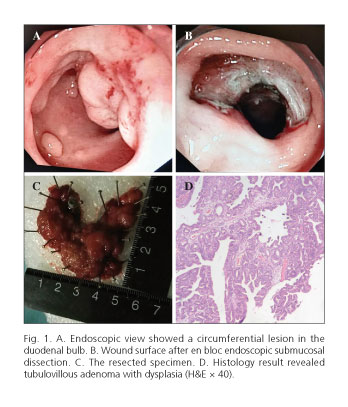
The patient received ESD (Fig. 1B) under general anesthesia. The lesion was en bloc resected with no major complications such as bleeding or perforation. The size of the resected specimen was 10 x 3 cm (Fig. 1C). Histopathological results demonstrated a tubulovillous adenoma with mild to moderate dysplasia, concomitantly focal high-grade intraepithelial neoplasia, with free lateral and basal margins (Fig. 1D). He was discharged 6 days after ESD and no recurrence occurred within a 2-month follow-up.
Discussion
Due to the unique anatomical features, limited operating space and close association with pancreas, duodenal neoplasm is technically challenging in both diagnosis and treatment. Endoscopic therapy is increasingly being performed as a less-invasive alternative to surgery. To the best of our knowledge, the largest duodenal bulb lesion removed by endoscopic resection that has been reported was 4 x 3 cm (1). So the present case is the largest one ever, and demonstrated that ESD could serve as an alternative method for large neoplastic lesions in the duodenal bulb.
Junfeng Zhou, Yuyong Tan and Deliang Liu
Department of Gastroenterology. The Second Xiangya.
Hospital of Central South University.
Changsha, Hunan. China
Junfeng Zhou: liudeliang1964@163.com
References
1. Jin P, Sheng J, Li A, et al. Submucosal tunnel dissection through the pyloric ring for removal of a sessile duodenal adenoma adjacent to a scar. Endoscopy 2013;45(Suppl. 2 UCTN):E303-4. DOI: 10.1055/s-0033-1344557. [ Links ]
