










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versão impressa ISSN 1130-0108
Rev. esp. enferm. dig. vol.108 no.9 Madrid Set. 2016
PICTURES IN DIGESTIVE PATHOLOGY
Over-the-scope clip closure of gastrocutaneous fistula
Eduardo Rodrigues-Pinto, Pedro Pereira, Filipe Vilas-Boas and Guilherme Macedo
Department of Gastroenterology. Centro Hospitalar São João. Porto, Portugal
Case Report
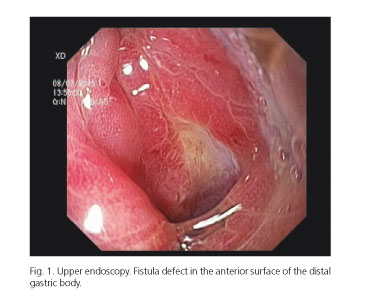
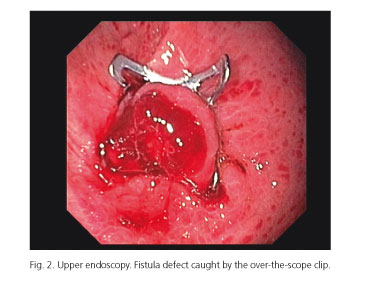
A 35-year-old female patient, with Batten's disease, submitted to a surgical gastrostomy in 2005, and had it replaced in 2007, 2011 and 2014 with one with a filled balloon as its internal retention mechanism. In 2015, she presented to the emergency room due to stomal enlargement, leakage and chemical dermatitis and cellulitis. Despite removal of the tube, nothing-by-mouth, acid suppression and antibiotics, there was clinical deterioration with associated sepsis. Abdominopelvic computed tomography revealed large volume ascites with inflammatory changes around gastrostomy. Upper endoscopy revealed a fistula defect in the anterior surface of the distal gastric body (Fig. 1). A 12 mm over-the-scope clip (OTSC, Ovesco, Tübingen, Germany) was placed, after anchoring the fistula edges with the twin grasper and suction of the defect into the applicator cap (Fig. 2). Endoscopic resolution of the fistula was achieved.
Discussion
Persistent gastrocutaneous fistula (GCF) after gastrostomy tube removal is a recognized sequela of long-term use, with a reported incidence of 2 to 44% (1). A persistent GCF has been defined as persistence of the gastrostomy tract a month after gastrostomy tube removal (2). The most important predictive factor for persistent gastrocutaneous fistula is the length of time the tube is in place (3). The aim of conservative medical therapy is to increase gastric emptying, increase gastric pH and decrease intragastric pressure (4). OTSC success is related to the ability of the OTSC to incorporate the entire thickness of the visceral wall; however, results are affected by fibrosis and scarring, that may prevent complete incorporation of the defect into the applicator cap and successful OTSC application. In the setting of complications after gastrostomy tube removal (ascites), a more proactive approach may be indicated, in order to avoid clinical deterioration. OTSC allows a faster resolution than conservative and pharmacologic treatment.
References
1. Haws EB, Sieber WK, Kiesewetter WB. Complications of tube gastrostomy in infants and children. 15-year review of 240 cases. Ann Surg 1966;164:284-90. DOI: 10.1097/00000658-196608000-00015. [ Links ]
2. Gordon JM, Langer JC. Gastrocutaneous fistula in children after removal of gastrostomy tube: Incidence and predictive factors. J Pediatr Surg 1999;34:1345-6. DOI: 10.1016/S0022-3468(99)90008-8. [ Links ]
3. Siddiqui AA, Kowalski T, Cohen S. Closure of a nonhealing gastrocutaneous fistula using an endoscopic clip. South Med J 2007;100:75-6. DOI: 10.1097/SMJ.0b013e31802f86a2. [ Links ]
4. Kobak GE, McClenathan DT, Schurman SJ. Complications of removing percutaneous endoscopic gastrostomy tubes in children. J Pediatr Gastroenterol & Nutr 2000;30:404-7. DOI: 10.1097/00005176-200004000-00010. [ Links ]
