










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkEnfermería Global
versão On-line ISSN 1695-6141
Enferm. glob. vol.21 no.66 Murcia Abr. 2022 Epub 05-Maio-2022
https://dx.doi.org/10.6018/eglobal.491181
Originals
Space-time dynamics and factors associated with suicide among young people in Northeastern Brazil: an ecological study
1 Departamento de Enfermería, Universidad Estadual de Piauí , Parnaíba-PI, Brasil. taynaralaissilva@gmail.com
2 Departamento de Enfermería, Universidad Estadual de Ceará , Fortaleza-CE, Brasil.
Objective:
To analyze the space-time pattern and the factors associated with suicide mortality among young people in northeastern Brazil.
Method
An ecological study that analyzed suicide deaths among young people aged 15 to 24 years in the Northeast region. Joinpoint software was used for temporal analysis and spatial analysis was carried out using local empirical Bayesian methods, Global and Local Moran Index and scanning spatial statistics technique. The multivariate model Ordinary Least Squares Estimation was used to identify the factors associated with mortality. The Scan scanning method identified six statistically significant spatial suicide clusters.
Results
Suicide among young people showed significant growth (p<0.001) of 2.8% per year in the Northeast region in the period studied. Moran's scattering analysis identified spatial clusters of deaths in the states of Piauí, Ceará, Rio Grande do Norte and Paraíba. The indicators: percentage of unemployed from 15 to 24 years (β = -0.05; p=0.02) and percentage of vulnerable to poverty (β =-0.06; p=0.03) had a negative association, while the illiteracy rate from 18 to 24 years (β= 0.15; p=0.01) and the percentage of people aged 18 to 24 years with complete elementary school (β = 0,09; p<0,001) positive association with suicide mortality among young people.
Conclusions
There was a significant increase in suicide among young people in the Northeast region. Clusters with the highest suicide rates were located in the state of Piauí. Four socioeconomic indicators were associated with suicide among young people in the region.
Keywords: Suicide; Youths; Mortality; Spatio-Temporal Analysis
INTRODUCTION
Annually, it is estimated that more than 800 thousand people die by suicide worldwide and, for every adult who commits suicide, at least another 20 try to take their own life1. This phenomenon is complex and multifactorial, considering that social, psychological and cultural factors can interact to lead a person to suicidal behavior and from a contextual analysis it is possible to understand and prevent higher risk situations, such as depressive disorders, abuse/dependence of alcohol/drugs and social isolation2.
Among young people aged 15 to 29 years, the situation is quite delicate, as suicide is the third leading cause of death in this population worldwide3. Youth refers to the stage of life that corresponds to the period between childhood and adulthood. It is a stage for the acquisition of social skills, assignment of duties, responsibilities and affirmation of identity. The choices made at this stage of life have a strong influence on the future4. Most teenagers have several factors that individually increase their vulnerability to anguish and emotional suffering, elements that, cumulatively, can lead to suicidal behavior5.
Adolescent mortality from self-harm in Brazil has shown a growing trend in recent years, especially in the male population, particularly in the Northeast region of Brazil6. Thus, suicidal behavior in adolescence and youth should be considered an absolute priority of public health care policies, as, in addition to the individual and family impacts, the death of individuals in this age group compromises the country's development, since in the future they could be part of the economically active population7.
Considering that the high suicide mortality rates are related to the socioeconomic characteristics of the environments where the populations live, it is essential to understand the relationship between the increasing occurrence of the disease and its distribution in time and space, correlating to the socioeconomic situation of Brazilian cities8. Therefore, it is necessary to analyze the occurrence of the problem in the young age group, considering its spatial and temporal location and associated factors in order to understand how the phenomenon of suicide occurs. So, this study has as objective to analyze the spatio-temporal pattern and factors associated with suicide mortality among young people in Brazilian northeastern region.
MATERIAL AND METHOD
This is an epidemiological study, of the ecological type, in which were analyzed the characteristics of young people population aged 15 to 24 years who committed suicide in the Northeast region of Brazil. The age definition of youth can vary from country to country, however, in Brazil the definition of the United Nations (UN) has been used4.
According to the last demographic census, in 2010 the Northeast region had a population of 53.1 million inhabitants, of which 10.3 million were young, constituting the second-largest population in this age group among Brazilian regions. Nowadays, it is estimated a population of approximately 57.4 million inhabitants, of which 26% are young9. We emphasize that the Northeast region is composed of 1,794 cities that integrates nine states: Maranhão (MA), Piauí (PI), Ceará (CE), Rio Grande do Norte (RN), Paraíba (PB), Pernambuco (PE), Alagoas, Sergipe (SE), and Bahia (BA).
Secondary data were obtained electronically at the portal of the Information Technology Department of the Unified Health System (DATASUS) of the Brazilian Ministry of Health and coming from the Mortality Information System (SIM). For that, we selected the deaths of young people living in the Northeast region that occurred in the period from 2010 to 2019 and whose codes X60 to X84 were mentioned according to the 10th International Classification of Diseases (ICD-10).
Demographic data of the young population of the states and cities of the Northeast region were obtained from the website of the Brazilian Institute of Geography and Statistics (IBGE) available at DATASUS and correspond to the 2010 Demographic Census and Intercensus Estimates9. The socioeconomic data were obtained from the website of the Atlas of Human Development10. The indicators collected were Gini Index, 18 to 24-year-old unemployment rate, Municipal Human Development Index (MHDI), dependency ratio, illiteracy rate, percentage of 18 to 24-year-old people having complete primary education, income per capita, percentage of vulnerable to poverty, percentage of people aged 18 to 24 in school, percentage aged 15 to 24 who do not study, do not work and are vulnerable, in the vulnerable population of this age group. It is noteworthy that data collection and tabulation were performed by the authors, who also performed the analyses.
The analysis of the temporal tendency of regression by inflection points was performed for the general population of young people who live in the Northeast region and by sex, as well as values were obtained for each of the nine states in the region. For this, the software Joinpoint Regression Program version 4.6.0.0 was used, in which it was evaluated whether a line with multiple segments describes the model better than just a straight line. Annual Percentage Change (APC) was calculated using a 95% confidence interval (95%CI), in which a negative APC value indicates a decreasing tendency and a positive value indicates an increasing tendency. A 5% significance level was established to test the null hypothesis that the APC of the series was equal to zero. For the APC analysis, results with p<0.05 or 95%CI only positive (increasing tendency) or only negative (decreasing tendency) are significant11.
The year of occurrence of the suicide was chosen as an independent variable and as a dependent variable the mortality rate in each year by state, calculated directly in the program. Thus, the number of deaths was selected as the numerator and the population of the year selected as the denominator, considering the coefficient for 100,000 inhabitants.
Crude suicide mortality rates among young people aged 15 to 24 in each city in the Northeast region were also calculated. The rates were calculated using the number of deaths from suicide in the cities in each year as the numerator, and as the denominator, we opted for standardization by the indirect method, in which it was used the population average regarding the two central years of the study. (2014-2015), multiplied by 100,000 inhabitants. However, in order to minimize the instability of the crude rates, they were later softened using the Local Empirical Bayesian method to correct random fluctuations, especially in cities with a few inhabitants12.
The dependency structure among observed suicide values in northeastern cities was analyzed using the spatial auto-correlation function. Initially, the Global Moran Index was applied to test the spatial dependence hypothesis and provide a general measure of association for the entire study area.
Once the presence of global spatial auto-correlation was found, the Moran Local Index (Local Index Spatial Analysis - LISA) was applied to verify the presence of spatial clusters and quantify the degree of spatial association in each city from the sample set. This technique allows you to graphically visualize the degree of similarity between neighbors through the Moran scatter diagram or Moran Map, in which the High/High pattern (in red) represents cities with high suicide rates surrounded by cities with equally high rates, and the Low/Low pattern (in green) indicates cities that have low suicide rates and are surrounded by cities with similarly low rates. Cities in yellow (High/Low) and blue (Low/High) indicate areas of epidemiological transition.
The formation of purely spatial clusters of deaths by suicide among young people was evaluated using the spatial statistical Scan technique. To identify clusters, the discrete it was adopted the Poisson model, which considers that the number of events in each area is proportional to the size of the population at risk, as well as the following requirements: do not present geographic overlap of the clusters, maximum cluster size equal to 5.0% of the exposed population, clusters in a circular shape and 999 replications (BRASIL, 2006). Together, spatial maps of relative risk (RR) were generated for the formation of death clusters in the region.
TerraView v.4.2.2® software was used to obtain the neighborhood matrix, to calculate crude and Bayesian rates and global and local estimates of spatial auto-correlation. For the application of the spatial statistical Scan technique, it was used the SatScan v.9.6® software. The maps were created using the QuantumGis v.2.14.17® software.
For the multivariate analysis, the variable adjustment of the dependent (suicide mortality rate among young people) and independent (socioeconomic variables) was performed using the Ordinary Least Squares Estimation (OLS) model. The presence of collinearity between the independent variables was verified using the Variance Inflation Factor (VIF). Non-collinear variables were included in the OLS model, adopting a statistical significance of 5%. To calculate the OLS multivariate model, it was used the STATA v.12® software.
The project of this study was approved by the Research Ethics Committee of the State University of Piauí (CEP/UESPI) under resolution nº 3.286.816 and Certificate of Presentation of Ethical Appreciation (CAAE) nº 07557818.4.0000.5209. Furthermore, all ethical and legal aspects were respected as recommended by Resolutions 466/12 and 510/2016 of the National Health Council.
RESULTS
In the Northeast, 4,634 deaths from suicide were reported among young people aged 15 to 24 years in the period from 2010 to 2019, with an average mortality rate in the study period of 5.19 deaths per 100,000 inhabitants. Self-provoked deaths were predominant among male individuals (n=3,480; 75.0%), four to seven years of schooling (n=1,066; 40.1%), single (n=3,981; 92.4 %) and brown color/race (n=3,405; 79.0%). Most deaths occurred in the victim's home (n=2,929; 67.3%), with hanging, strangulation and suffocation being the most chosen method for committing suicide (n=3,164; 68.3%) (Table 1).
Table 1: Sociodemographic characterization of suicide deaths among young people in the Northeast in the period 2010-2019. Parnaíba, Piauí, Brazil, 2021. (N = 4,634)
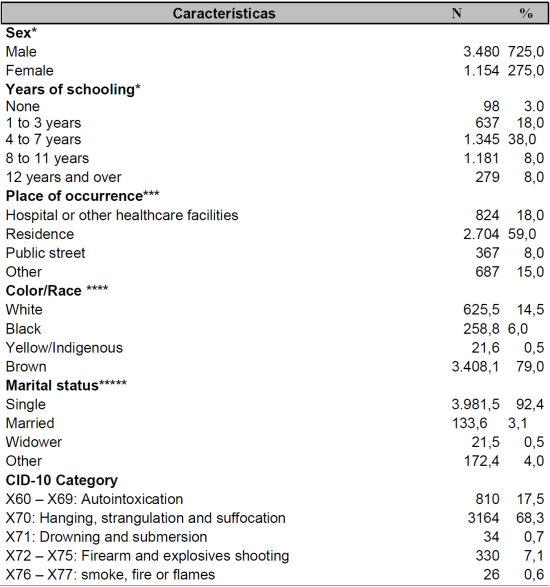
*4 Cases were excluded due to “ignored” sex.
**1.094 Cases were excluded because the years of schooling were listed as "ignored".
***52 cases were excluded because the place of occurrence was listed as “ignored”.
****320 cases were excluded due to their color/race were listed as “ignored”.
*****325 cases were excluded due to marital status were listed as "ignored".
The temporal analysis by Joinpoint shows that in the analyzed period, there was a statistically significant increase of 2.8% (95%CI: 0.5 - 5.1; p<0.001) per year in mortality from suicide among young people in the Northeast region. When the analysis was performed according to gender, it was found that in the period 2010-2019 there was an increase of 3.2% (95%CI: 2.0 - 4.5; p<0.001) per year in self-harm among young men, while in the period 2014-2019 there was a growth of 6.0% (95%CI: 00.1 - 12.3; p<0.001) per year in deaths by suicide among young women. (Table 2). The analysis also showed a statistically significant increase (p<0.001) in mortality from suicide among young people in four northeastern states: Piauí (APC: 4.9; 95%CI: 1.1 - 8.8), Bahia (APC : 4.6; 95%CI: 1.2 - 8.1), Maranhão (APC: 3.9; 95%CI: 0.9 - 6.9) and Pernambuco (APC: 3.3; 95%CI: 0. 1 - 6.6) (Table 2).
Table 2: Annual percentage variation by suicide mortality among young people according to sex and state of residence from 2010 to 2019. Parnaíba, Piauí, Brazil, 2021.
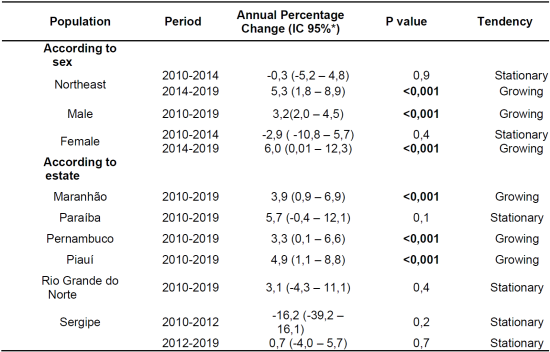
*IC95%: 95% confidence index.
The spatial distribution of the average crude suicide mortality rate for the period 2010-2019 is shown in Map A. It can be seen that, even though it is a map of gross mortality rates, the distribution of the highest rates is mostly in the state of Piauí. After softening by the Bayesian method, clusters of deaths were found (in orange and brown) that covered a significant portion of the cities in the states of Piauí, Ceará and Southern Maranhão, with rates ranging from 8.47 to 25.42 deaths per 100,000 inhabitants (Map B) (Figure 1).
The Moran Global index showed a statistically significant positive spatial auto-correlation (I = 0.12; p=0.001). Once the spatial dependence was verified, the Local Moran Index was calculated in order to identify clusters of the problem. Thus, in map C, the classification of the cities in the Northeast is observed in terms of mortality rates from suicide among young people, according to the Moran scatter plot. Cities with a High/High spatial pattern (in red) are predominantly located in the states of Piauí, Ceará, Rio Grande do Norte and Paraíba. Cities with a Low/Low distribution pattern (in green) are located especially in Bahia, Maranhão, Rio Grande do Norte and Paraíba.
All cities that presented a spatial pattern in the Moran Map (Map C) were significant in the Lisa Map (Map D) with p<0.05. However, it can be observed that almost all cities with a High/High spatial pattern and a statistical significance of 99.9% (p=0.001) are in the state of Piauí (Figure 1).
Figure 1 also shows the maps of clusters and relative risk of deaths from suicide among young people, calculated using the purely spatial Scan method. In map E, 11 clusters were identified, in which only six were statistically significant (p<0.05). The primary cluster (in red), which is the one with the highest likelihood, included 155 cities, predominantly in the northeastern subregion Meio Norte, in the state of Piauí. Furthermore, as in the spatial auto-correlation test, some cities in Ceará, Rio Grande do Norte and Paraíba, although secondary, also showed significant spatial clusters (in yellow). Map F, on the other hand, shows that the municipalities of Jurema (PI), Rio Grande do Piauí (PI), Santa Cruz do Piauí (PI) and Aroeiras do Itaim (PI) (in dark blue), have a risk of suicide of 7, 04 to 10.57 times higher than the risk observed in the entire Northeast region.
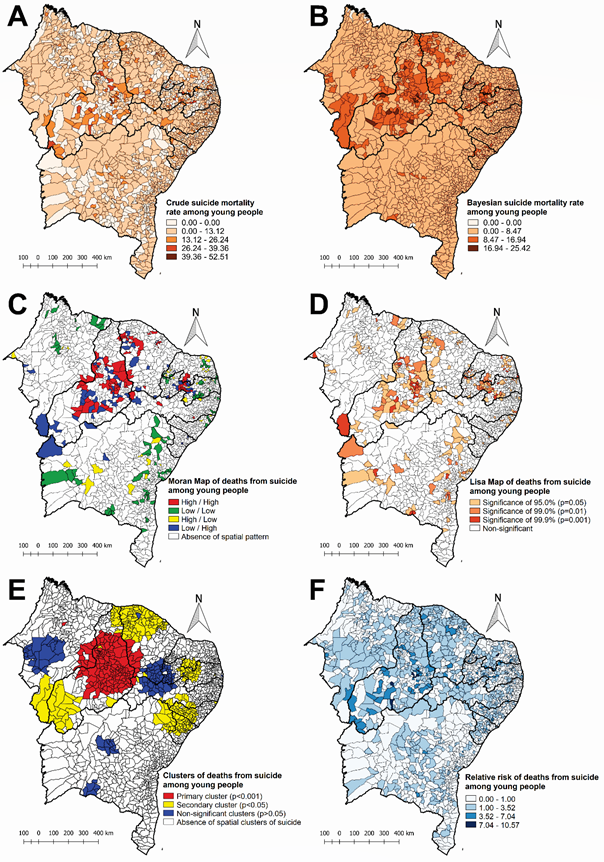
Figure 1: Spatial pattern of suicide mortality among young people in the Northeast in the period 2010-2019. Parnaíba, Piauí, Brazil, 2021.
Table 3 presents detailed information on clusters of suicide deaths in the young population identified by the purely spatial Scan method. The primary cluster has a radius of 218.8 km and its cities have, on average, 2.18 times more risk of suicide compared to the entire studied area (Northeast).
Table 3: Spatial clusters of deaths from suicide in young people in the Northeast in the period 2010-2019, defined by purely spatial scanning statistics. Parnaíba, Piauí, Brazil, 2021.
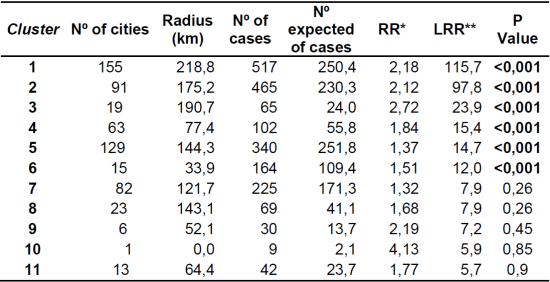
*RR: Relative risk for the cluster compared to the rest of the state;
**LLR: Logarithmic likelihood ratio test.
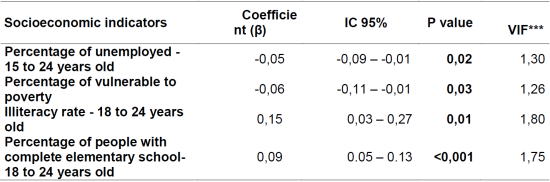
Table 4 shows the adjustment of the OLS model for the suicide mortality rate among young people. In this model, the coefficient of determination (R²) was 0.0166, which means that the set of selected socioeconomic indicators was able to partially explain the variability of suicide at 1.66%.
The socioeconomic indicators percentage of unemployed aged 15 to 24 years (β = -0.05; p=0.02) and percentage of vulnerable to poverty (β = -0.06; p=0.03) showed a negative association with the suicide in the young population. In turn, the indicators: illiteracy rate from 18 to 24 years old (β = 0.15; p=0.01) and percentage of people from 18 to 24 years old with complete primary education (β = 0.09; p<0.001) showed a positive association with mortality (Table 4).
DISCUSSION
The results lead us to confirm that there was an increase in mortality from suicide in the young population of the studied region. Young women presented the higher increase in suicide mortality in northeastern Brazil in recent years. The same fact was observed in a study performed in Spain, which showed that suicide mortality among women increased from 2010 to 2016, while among men the rates remained sTable, requiring further studies to justify the determinants of this increasing according to gender13.
In this study, spatial clusters of deaths by suicide were identified, with emphasis on the state of Piauí. This finding corroborates with a study which showed that among the ten cities with the highest suicide rates in the Northeast region, five belonged to Piauí14. Although poverty and income inequality in the Northeast region of Brazil have declined in recent decades, this region still has the worst social indicators compared to other regions of the country, in addition it presents strong patterns of socioeconomic heterogeneity in its territory14. In the states of Maranhão and Piauí are concentrated cities with a high percentage of poverty, a high Gini index and the lowest per capita income, surrounded by other municipalities in the same situation, located mainly in the northeastern subregion of Meio Norte. This subregion represents a transitional area between the Amazon and the semi-arid backlands of the northeast, composed by the states of Maranhão and West of Piauí, which is economically poorly developed, prevailing activities such as plant extractivism, traditional agriculture and extensive livestock farming15.
The state of Ceará also presented clusters of deaths from suicide among young people. It is observed that the historical trajectory of the Northeast presents resistant patterns of socio-spatial inequalities. However, the region's achievements in recent decades are notorious, such as poverty reduction, income growth, strong growth and changes in economic dynamics15. In this context, Ceará state has passed for a broad process of transformation in recent decades, with important advances in economic and social indicators, which has presented as consequence an improvement in the population's well-being16.
Furthermore, research developed in Rio Grande do Norte showed that deaths by suicide were not related to worse living conditions, as socioeconomic indicators were associated with high mortality rates, especially in well-developed regions17. Likewise, an investigation carried out in India showed that populations who lived in less economically developed states were associated with a lower risk of suicide compared to more developed states18. We emphasize the complexity of the suicide problem which, as it has a multifactorial cause, requires a contextual analysis of individuals in order to act in situations of higher risk and prevent its occurrence2.
Regarding the analysis of associated factors, it was observed that the variable percentage of unemployed persons aged 15 to 24 years had a negative association with mortality from suicide among young people in the Northeast. A study performed with young adults in France showed that unsTable and unfavorable jobs can increase the possibilities of suicidal behavior, which must be monitored, especially in economic crisis periods19.
In this context, the working population can often be exposed to precarious working conditions, low wages, transportation difficulties and long commutes to work, which can have disastrous effects on the physical and mental health of individuals. Such conditions indicate that work-related overload and emotional suffering can be so accentuated that the worker's risk of suicide is higher than the risk attributed to the unemployed20.
The percentage of people vulnerable to poverty also had a negative association with suicide mortality among young people, which means that the lower the income, the higher the suicide mortality rate. A similar finding was observed in a study carried out in Rio Grande do Sul, a state with cities with the highest suicide rates in the country, which indicated that cities with the highest percentage of people in poverty had higher numbers of suicides. Therefore, we emphasize that the results should be interpreted with caution, due to the complexity of the factors that influence the intention to commit suicide, not reducing them only to economic factors 8).
The illiteracy rate variable was a risk factor for suicide mortality, which means that the higher the illiteracy rate, the greater the risk of suicide mortality among young people. The low level of education has been identified as a risk factor for suicide in many investigations developed in Brazil 21)(22)(23)(24 and in other countries 18,25. It is important to emphasize that a systematic review with meta-analysis showed that school-based educational suicide prevention interventions had a positive effect on the prevention of suicide attempts 26.
On the other hand, the variable percentage of people with complete elementary education also showed a positive association with suicide mortality. A similar finding was observed in a study carried out in South Africa, which found that people with any education (primary school and above) were more likely to die from suicide compared to people who had no education. This investigation also demonstrated that the risk of death from suicide increased as the level of education increased 27.
This study presents as limitation the use of secondary data, which may present inconsistencies due to inadequate filling and underreporting. In addition, indicators and population data refer to the 2010 Demographic Census and Inter-Census Estimates, as the new national census scheduled for 2020 has not been done. Furthermore, some results of this study should be interpreted with caution, as even the predictor variables of suicide having shown statistical significance in the OLS model, their estimated coefficients are very close to zero, demonstrating that their effect on the outcome variable is small. Despite this, such limitations do not make the research impracticable and do not reduce its importance.
CONCLUSION
Through this study, it was possible to observe a significant tendency of increasing mortality from suicide among young people in the Northeast region, especially in Piauí and Bahia. In addition, six spatial clusters of suicide were identified, and the primary cluster predominantly included cities from the Middle North part of Piauí. Finally, the socioeconomic indicators, percentage of unemployed aged 15 to 24 years, percentage of vulnerable to poverty, presented negative association with suicide among the young population. The illiteracy rate between 18 and 24 years old, and the percentage of people between 18 and 24 years old with complete elementary school presented a positive association.
The findings of this study produce evidences that contributes to understand the epidemiological profile and the way in which suicide is distributed among young people in the time and space of the Northeast region, and they also show social indicators that are presented as protective or risk factors for this public health problem. Such information may support the development of specific prevention policies for this age group. In this context, it is important to emphasize the necessity of directing prevention strategies to the cities which present more frequent cases, so that public health actions would be more effective.
REFERENCIAS
1. World Health Organization (WHO). Preventing suicide: a global imperative. Geneva; 2014.1-141p. Disponível em: https://www.who.int/publications/i/item/9789241564779 [ Links ]
2. Ribeiro NM, Castro SS, Scatena LM, Haas VJ. Ánálise da tendência temporal do suicídio e de sistemas de informações em saúde em relação às tentativas de suicídio. Texto Context Enferm. 2018;27(2):1-11. Disponível em: https://doi.org/10.1590/0104-070720180002110016 [ Links ]
3. Pan-American Health Organization - PAHO. The Health of Adolescents and Youth in the Americas: Implementation of the Regional Strategy and Plan of Action on Adolescent and Youth Health 2010-2018. PAHO: Washington, D.C.; 2019. Disponível em: https://www.paho.org/adolescent-health-report-2018/ [ Links ]
4. Fundo das Populações das Nações Unidas (UNFPA). Direitos Da População Jovem [Internet]. 2010. 126p. Disponível em: http://www.unfpa.org.br/Arquivos/direitos_pop_jovem.pdf [ Links ]
5. Valadez-Figueroa I, Chávez-Hernández A, Vargas-Valadez V, Hernández-Cervantes Q, Ochoa-Orendain MC. Tentativa suicida y uso del tiempo libre en adolescentes escolarizados mexicanos Suicide attempt and leisure in Mexican. Ter Psicológica 2019 [Internet]. 2019; 37:5-14. Available from: https://dx.doi.org/10.4067/S0718-48082019000100005 [ Links ]
6. Cicogna JIR, Hillesheim D, Hallal AL de LLC. Mortalidade por suicídio de adolescentes no Brasil: tendência temporal de crescimento entre 2000 e 2015. J Bras Psiquiatr [Internet]. 2019 Mar;68(1):1-7. Disponível em: https://doi.org/10.1590/0047-2085000000218. [ Links ]
7. Silva L. Suicídio entre crianças e adolescentes: um alerta para o cumprimento do imperativo global. Acta Paul Enferm [Internet]. 2019 Jun;32(3):III-IVI. Disponível em: https://doi.org/10.1590/1982-0194201900033. [ Links ]
8. Fraga WS de, Massuquetti A, Godoy MR. Determinantes Socioeconômicos do Suicídio: um estudo para os municípios do Brasil e do Rio Grande do Sul. Rev Econômica [Internet]. 2016 Mar 29;18(2):1-37. Disponível em: https://doi.org/10.22409/economica.18i2.p300 [ Links ]
9. Instituto Brasileiro de Geografia e Estatística (IBGE). Estimativas de população. Brasília: IBGE, 2020. Disponível em: https://www.ibge.gov.br/estatisticas/sociais/populacao/9103-estimativas-de-populacao.html?=&t=resultados Acesso em: 13/04/2021. [ Links ]
10. Programa das Nações Unidas (PNUD). Atlas do Desenvolvimento Humano no Brasil. Rio de Janeiro; 2021. PNUD, IPEA, Fundação João Pinheiro. Disponível em: http://www.atlasbrasil.org.br/consulta/ Acesso em: 20/03/2021. [ Links ]
11. Sousa GJB, Garces TS, Pereira MLD, Moreira TMM, da Silveira GM. Temporal pattern of tuberculosis cure, mortality, and treatment abandonment in Brazilian capitals. Rev Lat Am Enfermagem. 2019;27. Disponível em: https://doi.org/10.1590/1518-8345.3019.3218 [ Links ]
12. Ministério da Saúde (BR). Abordagens espaciais na saúde pública. Brasília, DF(BR): MS, 2006 [acesso em 2020 Ago 10]; Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/serie_ geoproc_ vol_1.pdf [ Links ]
13. Cayuela A, Cayuela L, Sánchez Gayango A, Rodríguez-Domínguez S, Pilo Uceda FJ, Velasco Quiles AA. Suicide mortality trends in Spain, 1980-2016. Rev Psiquiatr Salud Ment. 2020;13(2):57-62. Disponível em: https://doi: 10.1016/j.rpsm.2018.07.002 [ Links ]
14. Santos EG de O, Barbosa IR. Conglomerados espaciais da mortalidade por suicídio no nordeste do Brasil e sua relação com indicadores socioeconômicos. Cad Saúde Coletiva. 2017 Oct;25(3):371-8. Disponível em: https://doi.org/10.1590/1414-462X201700030015 [ Links ]
15. Hissa-Teixeira K. Uma análise da estrutura espacial dos indicadores socioeconômicos do nordeste brasileiro (2000-2010). Eure. 2018;44(131):101-24. Disponível em: http://dx.doi.org/10.4067/S0250-71612018000100101 [ Links ]
16. Bezerra FJA, Bernardo TRR, Ximenes LJF, Junio ASV. Perfil socioeconômico do Ceará [Internet]. Fortaleza: Banco do Nordeste do Brasil; 2015. 194 p. Disponível em: https://www.bnb.gov.br/documents/80223/4476032/CE+Perfil+2015.pdf/d96d6707-78c5-7fb9-f08c-c9cde00e455e [ Links ]
17. Santos EGO, Barbosa IR, Severo AKS. Análise espaço-temporal da mortalidade por suicídio no Rio Grande do Norte, Brasil, no período de 2000 a 2015. Cien Saude Coletiva [Internet]. 2020; 25(2):633-43. Disponível em: https://doi.org/10.1590/1413-81232020252.11042018 [ Links ]
18. Arya V, Page A, River J, Armstrong G, Mayer P. Trends and socio-economic determinants of suicide in India: 2001-2013. Soc Psychiatry Psychiatr Epidemiol [Internet]. 2018 Mar 5;53(3):269-78. Disponível em: http://dx.doi.org/10.1007/s00127-017-1466-x [ Links ]
19. Dalglish SL, Melchior M, Younes N, Surkan PJ. Work characteristics and suicidal ideation in young adults in France. Soc Psychiatry Psychiatr Epidemiol. 2015;50(4):613-20. Disponível em: https://doi.org/10.1007/s00127-014-0969-y [ Links ]
20. Pinto LLT, Meira SS, Ribeiro ÍJS, Nery AA, Casotti CA. Tendência de mortalidade por lesões autoprovocadas intencionalmente no Brasil no período de 2004 a 2014. J Bras Psiquiatr. [Internet] 2017; 66(4):203-10. Disponível em: http://dx.doi.org/10.1590/0047-2085000000172 [ Links ]
21. Bahia CA, Avanci JQ, Pinto LW, Minayo MCS. Lesão autoprovocada em todos os ciclos da vida: perfil das vítimas em serviços de urgência e emergência de capitais do Brasil. Cien Saude Colet [Internet]. 2017 Sep;22(9):2841-50. Disponível em: https://doi.org/10.1590/1413-81232017229.12242017 [ Links ]
22. Santos AD, Guimarães LML, Carvalho YF, Viana LC, Alves GL, Lima ACR, et al. Spatial analysis and temporal trends of suicide mortality in Sergipe, Brazil, 2000-2015. Trends Psychiatry Psychother [Internet]. 2018 Dec;40(4):269-76. Disponível em: https://doi.org/10.1590/2237-6089-2017-0028 [ Links ]
23. Silva IG, Maranhão TA, Silva TL, Sousa GJB, Lira Neto JCG, Pereira MLD. Gender differentials in suicide mortality. Rev Rene [Internet]. 2021 Feb 23;22:e61520. Disponével em: https://doi.org/10.15253/2175-6783.20212261520 [ Links ]
24. Silva TL, Maranhão TA, Sousa GJB, Silva IG, Lira Neto JCG, Araujo GAS. Análise espacial do suicídio no Nordeste do Brasil e fatores sociais associados. Texto Context Enferm. 2022;31. No prelo. [ Links ]
25. Haghparast-Bidgoli H, Rinaldi G, Shahnavazi H, Bouraghi H, Kiadaliri AA. Socio-demographic and economics factors associated with suicide mortality in Iran, 2001-2010: application of a decomposition model. Int J Equity Health [Internet]. 2018 Dec 14;17(1):77. Disponível em: https://doi.org/10.1186/s12939-018-0794-0 [ Links ]
26. Pistone I, Beckman U, Eriksson E, Lagerlöf H, Sager M. The effects of educational interventions on suicide: A systematic review and meta-analysis. Int J Soc Psychiatry [Internet]. 2019 Aug 4;65(5):399-412. Disponível em: https://doi.org/10.1177/0020764019852655 [ Links ]
27. Kootbodien T, Naicker N, Wilson KS, Ramesar R, London L. Trends in Suicide Mortality in South Africa, 1997 to 2016. Int J Environ Res Public Health [Internet]. 2020 Mar 12;17(6):1850. Disponível em: https://doi.org/10.3390/ijerph17061850 [ Links ]
Received: September 06, 2021; Accepted: December 18, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
