










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkEnfermería Global
versão On-line ISSN 1695-6141
Enferm. glob. vol.21 no.67 Murcia Jul. 2022 Epub 19-Set-2022
https://dx.doi.org/10.6018/eglobal.503621
Originals
Metabolic alterations in street traders in the city of Cuenca, Ecuador
1University of Cuenca, Cuenca, Ecuador
2Vicente Corral Moscoso Hospital Clinical Laboratory, Cuenca, Ecuador
3Ministry of Public Health Perpetual Relief Health Post, Loja, Ecuador
Introduction:
The metabolic syndrome is conceptualized as a set of metabolic abnormalities whose etiopathogenic expression includes a prothrombotic and pro-inflammatory state that increases the risk of morbidity and mortality in affected patients.
Objective:
The objective of the study was to analyze the behavior of the main clinical and laboratory elements that are part of the diagnostic criteria for metabolic syndrome.
Methodology:
A basic, non-experimental, cross-sectional cohort research was carried out, supported by the results of the occupational health inquiry of the street vendors of the January 9 Association of the city of Cuenca. The universe was made up of 150 merchants and the sample was made up of 109 workers. A questionnaire was applied to each participant to identify general characteristics and blood pressure values, nutritional status, blood glucose and lipid profile were analyzed.
Results:
Among the results, overweight merchants predominated (43.12%). 27.52% had high blood pressure Figures, as well as hyperglycemia in 15.60%; 39.45% presented hypertriglyceridemia and 36.40% hypercholesterolemia. Likewise, 34.86% of merchants with high LDL cholesterol and 29.36% presented low HDL cholesterol values.
Conclusions:
It is concluded that, in the group of street vendors investigated, there is a high presence of alterations in the clinical and laboratory components of the metabolic syndrome. Interventions are needed in this group and in the general population to achieve greater metabolic control and thus reduce the risk of complications related to these disorders.
Keywords: Dyslipidemias; Nutritional condition; Metabolic syndrome
INTRODUCTION
Chronic noncommunicable diseases (NCDs) are one of the world's leading health problems. Health professionals focus their struggle on achieving control of NCDs to minimize morbidity and mortality in this group of diseases1,2.
NCDs include high blood pressure (hypertension), diabetes mellitus (DM), bronchial asthma and metabolic syndrome (MS) among others. This last disease is considered one of the conditions that presents the greatest number of clinical manifestations and complications, being described not only as a disease, but also as a risk factor for other conditions such as hypertension and DM3,4.
MS is conceptualized as a set of metabolic abnormalities including obesity, elevated blood pressure Figures, dyslipidemias and alterations of serum glucose levels as an expression of insulin resistance syndrome. A prothrombotic and pro-inflammatory state secondary to MS is described that increases the risk of morbidity and mortality in affected patients5 6 7.
However, in order to reach the diagnosis of the disease it is necessary to have 3 of the 5 components of it5 6 7; each of them, although they are not part of the MS, they are a determining factor for the appearance of different disorders; among all of them there is a certain degree of dependence, since each one exerts a certain influence on the rest4 5 6.That is why it is of paramount importance the early identification of alterations in these components to avoid the progression of metabolic alterations that could condition the diagnosis of MS.
That is why, taking into account the importance of each of the components of the SM individually or collectively and the influence they can have on people's state of health; it is decided to carry out this research with the aim of analyzing the behavior of the main clinical and laboratory elements that are part of the diagnostic criteria of MS.
METHODS
A basic, non-experimental, documentary and cross-sectional cohort research was carried out, supported by the results of the occupational health inquiry of the street vendors of the 9 of January Association of the city of Cuenca in Ecuador. The research had a mixed approach by using both qualitative and quantitative elements. Logical history, synthetic analytical and deductive inductive were used as research methods.
The universe was made up of 150 people who work as street traders and who are members of the 9 of January Association of Merchants. To calculate the sample size, the mathematical formula for known populations was used:8
The nomenclature used was as follows:
n= Sample size
PQ= Population variance constant (0,25)
N= Population size (52.126 people)
e= Error (al 2%)
Z= Trust level (1,96)
Mathematical calculations determined that the sample size should include 109 workers. To form it, the simple random method was used so that each person had the same possibility of being part of the study sample. All street traders included in the investigation met the inclusion criteria and did not meet the exclusion criteria defined for the study.
Exclusion criterio
Street vendors not affiliated to the Association of Merchants January 9 of the city of Cuenca.
Street vendors who had not complied at the time of the investigation with the realization of the occupational health check.
Street vendors who showed no interest in participating in the research so they did not sign the informed consent.
To carry out this research, the following research variables were identified:
General characteristics: included the subvariants age, sex, presence of comorbidities and type of comorbidities.
Components of MS: this variable included the analysis of blood pressure values, serum cholesterol, HDL cholesterol, LDL cholesterol, glycemia and the nutritional status of the workers investigated.
During the development of the research, two research techniques were used, the documentary review and the interview. The documentary review allowed to obtain, from the clinical history of each worker, the data related to the two research variables. The interview allowed to inform the workers about the objectives and methods of the research as well as the final report of the results of the same.
It is important to mention that the research team was based on the results of periodic health check-up of the workers which is a requirement as part of occupational health monitoring. During the development of the study, no direct action was taken with the people who were part of the research.
For the classification of blood pressure Figures, the diagnostic criteria of the World Health Organization were taken into account which establish as normal values Figures below 140/90 mmHg; higher values can be considered as confirmatory of HTN9,10.
To identify nutritional status, the determination of body mass index (BMI) was used as an anthropometric measure. The formula for calculating BMI is based on the division of body weight expressed in kilograms, over the height of the person expressed in square centimeters.
The reference values defined by the WHO, and that were used in this research were:
Low weight: BMI less than 18.5 points
Normal weight: BMI between 18.5 and 24.9 points
Overweight: BMI between 25.0 and 29.9 points
Obesity: BMI equal to or greater than 30.0 points
The analysis of the laboratory tests was based on the reference values established by the clinical laboratory of the Diagnostic Center and Biomedical Research of the Faculty of Medical Sciences of the University of Cuenca and that defines the following parameters of normality.
Fasting blood glucose: between 75 and 115 mg/dl
Total cholesterol: up to 200 mg/dl
HDL cholesterol: greater than 40 mg/dl
LDL cholesterol: less than 100 mg/dl
Triglycerides: up to 150 mg/dl
The research instrument used was an eight-question questionnaire, created specifically for the study and that it was submitted to expert criteria and a pilot test prior to its final application. The questionnaire was oriented towards the identification of the general characteristics of the workers included in the study.
The information processing was carried out automatically using the statistical programStatistical Package for Social Sciences (SPSS)in its version 26 for Windows. Absolute frequencies and percentages were determined for the processing of qualitative variables and measures of central tendence and dispersion for quantitative variables.
The confidence level was defined at 95% with a margin of error of 5% and statistical significance was defined at a p ≤ 0.05. The results were expressed in the form of Tables and statistical graphs to facilitate their understanding.
The research complied with the standards set out in the Declaration of Helsinki 2 for conducting research on human beings. Each participant was informed, prior to the start of the study, about the objectives and methods used. The incorporation of the people was voluntary and each of them expressed, through the signature, the informed consent your desire to participate in the study and the authorization for your medical history data to be used. No personal identity data or other elements that could reveal the identity of the participants were used; only alpha numeric codes were used in strictly necessary cases. The database with the information collected was definitively deleted after the final report of the study was made.
RESULTS
The main results of this study are shown below:
Table 1shows the distribution of people according to the general characteristics identified. An average age of 53.62 years with SD of 21.38 is observed. There was a predominance of females (65.10%) and 32.11% reported at least one associated comorbidity. Among the comorbidities that were most frequently referred are hypertension (42.86%), hypothyroidism (34.28%) and fibromyalgia (14.28%).
Table 1. Distribution of people according to general characteristics
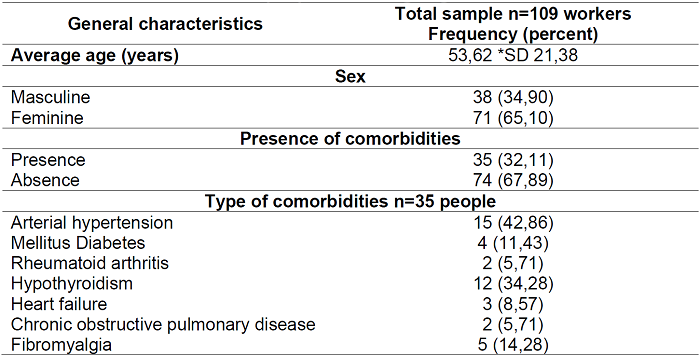
Source: research questionnaire *SD: standard deviation
InTable 2, the analysis of the clinical components of MS showed that 27.52% of the people investigated had elevated blood pressure Figures. In relation to nutritional status, it stands out that 59.63% of people had nutritional alterations due to excess; of these, 43.12% were overweight and 16.51% were considered obese (Table 1).
Quantitative analysis of nutritional status showed a mean BMI of 27.86 points with ED of 4.43, the lowest value was 17.17 points and the highest was 40.90 points.
Table 2. Distribution of people according to clinical components of the metabolic syndrome
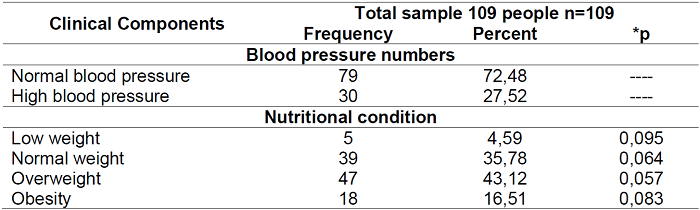
Source: clinical history *p≤ 0.05
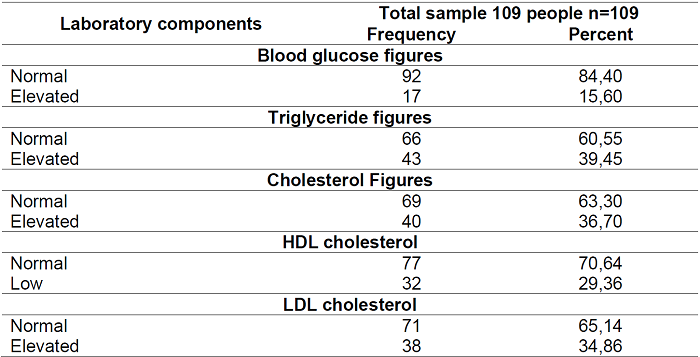
The results ofTable 3are directly related to the components of metabolic syndrome; in this sense, 15.60% of the people investigated with high blood glucose values stand out; 39.45% presented hypertriglyceridemia and 36.40% hypercholesterolemia. There were also 34.86% of traders with high LDL cholesterol and 29.36% had low HDL cholesterol values.
DISCUSSION
The components of MS constitute, individually, risk factors for the appearance of different NCDs such as hypertension and DM among others3,6. Health professionals working at the first level of health care have a responsibility to monitor behavior, clinical and laboratory components, mainly in patients at risk, to identify initial alterations of each of them.
The results of the present research show a high percentage of street vendors with associated comorbidities. Different investigations carried out in Ecuador report in high parameters to hundreds of people with different diseases. A similar result is reported by Solis Cartas and Calvopiña Bejarano11who report about 40% of people with different comorbidities.
Hypertension, hypothyroidism and fibromyalgia were the comorbidities that had the highest frequency of presentation. The prevalence of HBP in Ecuador at the end of 2019, according to data offered by the National Institute of Statistics and Census (INEC), it is around 18.7 percent of the population over 15 years of age; this Figure exceeds the 14.3% prevalence of hypertension in the Americas12.
One element to take into account is the high percentage of street vendors diagnosed with hypothyroidism; this disease has a high presence in the Ecuadorian epidemiological context, is a disease that is among the first 10 reasons for consultations according to INEC; an unreported popular theory relates the increased prevalence of hypothyroidism to the consumption, for many years, of non-iodized salt in the country.
Fibromyalgia is a rheumatic disorder that has increased its incidence and prevalence in recent years, is considered a predominant condition in female patients between 15 and 45 years of age and that it is directly related to stressful situations; in Ecuador, there are few reports of fibromyalgia13.
The analysis of the components of the MS showed some important elements related to the alterations of the values of each one. The determination of the blood pressure taking showed a very high percentage of street vendors with high Figures, it is even a result higher than the prevalence of hypertension in the country according to INEC12.
Many factors may be related to this outcome, nutritional disorders, inadequate diets, and inadequate habits and lifestyles are some of them. Research such as that of Larrea Fabra et al.14reports a direct relationship between the quality of feeding and the risk of the occurrence of hypertension.
For their part, Petermann and collaborators and Conesa Gonzalez and collaborators agree that nutritional disorders are not only a risk factor for HBP but also for other cardiovascular conditions. Other authors such as Miranda Pérez et al.17)describe in their research a relationship between nutritional habits and the risk of cardiovascular disease, including hypertension.
The analysis of nutritional status, according to BMI results, both qualitatively and quantitatively shows a high percentage of street vendors with nutritional alterations due to excess. There are other investigations that also report high percentages of different population groups with overweight and obesity18-19. Obesity and overweight, despite being an important component of MS, are risk factors for diseases as HBP, MD and dyslipidemias20 21 22.
Lipid alterations were also identified in percentages higher than those desired to maintain an adequate state of health. Other research carried out in Ecuador also reports high percentages of dyslipidemias, even reaching 50% of people investigated21-23.
In consideration of the limitations of the present study, first, the cross-sectional study design excluded casual conclusions and further longitudinal investigations were needed to determine the causal relationship. Secondly, some street vendors were constantly mobilized and could not be included in this study. Finally, clinical components and comorbidities need to be more detailed to explain the exact mechanisms and associations with metabolic syndrome, and these factors should be analyzed as covariates in future research.
CONCLUSION
In the group of street vendors investigated, there is a high presence of alterations in the clinical and laboratory components of the MS. Interventions are needed in this group and in the general population to achieve greater metabolic control and thus reduce the risk of complications related to these disorders.
The monitoring of the components of the SM will not only allow early identification of alterations and correct them to minimize the incidence and prevalence of the syndrome; it will also facilitate the control of some NCDs and the reduction of the risk of complications, for this reason, it is suggested that this study from another point of view of health professionals to analyze how the variables are seen from their perspective
REFERENCIAS
1. Serra Valdés M, Serra Ruíz M, Viera García M. Las enfermedades crónicas no transmisibles: magnitud actual y tendencias futuras. Rev. Finlay [Internet]. 2018 [citado 2021 Feb 13];8(2):140-8. Disponible en:http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S2221-24342018000200008&lng=es [ Links ]
2. Miguel Soca P, Sarmiento Teruel Y, Mariño Soler A, Llorente Columbié Y, Rodríguez Graña T, Peña González M. Prevalencia de enfermedades crónicas no transmisibles y factores de riesgo en adultos mayores de Holguín. Rev. Finlay [Internet]. 2017 [citado 2021 Feb 15];7(3):155-67. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S2221-24342017000300002&lng=es [ Links ]
3. Mora Marcial GR, Verdecia Tamallo K, Rodríguez Vergara TM, del Pino Bárbara N, Guerra Cabrera C. Adherencia terapéutica en pacientes con algunas enfermedades crónicas no transmisibles. Rev Cubana Med Gen Integr [Internet]. 2017 [citado 2021 Feb 18];33(3):270-80. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-21252017000300001&lng=es [ Links ]
4. Guerrero Wyss L, Durán Agüero S. Consumo de legumbres y su relación con enfermedades crónicas no transmisibles. Rev. chil. nutr. [Internet]. 2020[citado 2021 Feb 13];47(5):865-9. Disponible en: https://scielo.conicyt.cl/scielo.php?script=sci_arttext&pid=S0717-75182020000500865&lng=es [ Links ]
5. Carvajal Carvajal C. Síndrome metabólico: definiciones, epidemiología, etiología, componentes y tratamiento. Med. leg. Costa Rica [Internet]. 2017 [citado 2021 Feb 18];34(1):175-93. Disponible en: http://www.scielo.sa.cr/scielo.php?script=sci_arttext&pid=S1409-00152017000100175&lng=en [ Links ]
6. García García Y, Díaz Batista A, Arpajón Peña Y, Estévez Perera A, Aldama Figueroa A, Conesa González AI, et al. Enfermedad arterial periférica asintomática en pacientes con factores de riesgo del síndrome metabólico. Rev Cubana Angiol Cir Vasc [Internet]. 2018 [citado 2021 Feb 16];19(2):91-103. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1682-00372018000200004&lng=es [ Links ]
7. Huamán J, Alvarez M, Gamboa L, Marino F. Índice cintura-estatura como prueba diagnóstica del Síndrome metabólico en adultos de Trujillo. Rev Med Hered [Internet]. 2017[citado 2021 Feb 14];28(1):13-20. Disponible en: http://www.scielo.org.pe/scielo.php?script=sci_arttext&pid=S1018-130X2017000100003&lng=es [ Links ]
8. Rodríguez J, Pierdant A, Rodríguez E. Estadística para la Administración. Segunda ed. Grupo Editorial Patria, editor. México; 2016. [ Links ]
9. Shunchao K, Xueqing L, Blanco Aspiazu MÁ, Bacallao Gallestey J. Comorbilidad de pacientes ingresados con diagnóstico de Hipertensión arterial en salas de Medicina Interna. Rev haban cienc méd [Internet]. 2019[citado 2021 Feb 17];18(1):45-59. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1729-519X2019000100045&lng=es [ Links ]
10. Pérez Caballero MD, León Álvarez JL, Dueñas Herrera A, Alfonzo Guerra JP, Navarro Despaigne DA, de la Noval García R, et al. Guía cubana de diagnóstico, evaluación y tratamiento de la hipertensión arterial. Rev cubana med [Internet]. 2017 [citado 2021 Feb 14];56(4):242-321. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0034-75232017000400001&lng=es [ Links ]
11. Solís Cartas U, Calvopiña Bejarano SJ. Comorbilidades y calidad de vida en Osteoartritis. Rev Cuba Reumatol [Internet]. 2018 [citado 2021 Feb 14];20(2):e17. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1817-59962018000200002&lng=es [ Links ]
12. Instituto Nacional de Estadística y Censo (INEC). Enfermedades crónicas no transmisibles. Panorama nacional. Ministerio de Saliud Pública, Quito, Ecuador. 2020. [ Links ]
13. Solís Cartas U, Lema Tayupanda JG, Haro Chávez JM, Calidad de vida relacionada con la salud en pacientes con fibromialgia. Revista Caribeña de Ciencias Sociales, Servicios Académicos Intercontinentales SL. 2019(09). Disponible en: https://ideas.repec.org/a/erv/rccsrc/y2019i2019-0931.html [ Links ]
14. Larrea Fabra R, Duarte González G, Chávez Vega R. Diagnóstico de la hipertensión secundaria. (Revisión bibliográfica). Rev Cubana Med [Internet]. 2020 [citado 2021 Feb 16];24(3):[aprox. 9 p.]. Disponible en: http://www.revmedicina.sld.cu/index.php/med/article/view/2150 [ Links ]
15. Petermann F, Durán E, Labraña AM, Martínez MA, Leiva Ana M, Garrido-Méndez A, et al. Factores de riesgo asociados al desarrollo de hipertensión arterial en Chile. Rev. méd. Chile [Internet]. 2017[citado 2021 Feb 14];145(8): 996-1004. Disponible en: https://scielo.conicyt.cl/scielo.php?script=sci_arttext&pid=S0034-98872017000800996&lng=es [ Links ]
16. Conesa González AI, Yanes Quesada M, Zayas Torriente GM, González Padilla K, Domínguez Alonso E. Estado nutricional y factores de riesgo vascular en pacientes ingresados en el Centro de Atención al Diabético de La Habana. Rev Cubana Endocrinol [Internet]. 2017[citado 2021 Feb 18];28(2). Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1561-29532017000200005&lng=es [ Links ]
17. Miranda Pérez Y, Peña González M, Ochoa Roca TZ, Sanz Candía M, Velázquez Garcés M. Caracterización nutricional del adulto mayor en el policlínico. ccm [Internet]. 2019[citado 2021 Feb 18];23(1):122-43. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1560-43812019000100122&lng=es [ Links ]
18. Villacreses S, Gallegos Espinoza S, Chico P, Santillán E. Estado alimentario y nutricional de las comunidades originarias y campesinas de la región central del Ecuador. Rev Cubana Aliment Nutr [revista en Internet]. 2017 [citado 18 Feb 2021];27(1):[aprox. 24 p.]. Disponible en: http://revalnutricion.sld.cu/index.php/rcan/article/view/325 [ Links ]
19. Espinosa H, Abril-Ulloa V, Encalada L. Prevalencia de malnutrición y factores asociados en adultos mayores del cantón Gualaceo, Ecuador. Rev. chil. nutr. [Internet]. 2019 [citado 2021 Feb 14];46(6):675-82. Disponible en: https://scielo.conicyt.cl/scielo.php?script=sci_arttext&pid=S0717-75182019000600675&lng=es [ Links ]
20. Díaz-Martínez X, Petermann F, Salas-Bravo C, Garrido-Méndez A, Martínez MA, Leiva AM, et al. Efectos de la actividad física sobre la asociación entre obesidad y diabetes mellitus tipo 2: resultados de la Encuesta Nacional de Salud 2009-2010. Rev. méd. Chile [Internet]. 2017 [citado 2021 Feb 15];145(11):1394-402. Disponible en: https://scielo.conicyt.cl/scielo.php?script=sci_arttext&pid=S0034-98872017001101394&lng=es [ Links ]
21. Ruiz López JC, Letamendi Velasco JA, Calderón León RA. Dylispidemia prevalence in obese patients. MEDISAN [Internet]. 2020 [citado 2021 Feb 16] ;24(2):211-22. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1029-30192020000200211&lng=es [ Links ]
22. González Tabares Rubén, Acosta González Frank Abel, Trimiño Galindo Leydiana, Guardarrama Linares Layanis. Metabolic Risk Factors and Cardiovascular Disease Associated with Obesity in an Actively Working Population. Rev Cubana Med Gen Integr [Internet]. 2020[citado 2021 Feb 14];36(1): e1040. Disponible en: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-21252020000100003&lng=es [ Links ]
23. Uribe-Risco V, Holguín-Pilligua J, Valero-Cedeño N, Yépez-Martínez J. Prevalencia de dislipidemias en pacientes de la zona sur de Manabí, Provincia de Manabí-Ecuador. Polo del Conocimiento [Internet]. 2020[citado 2021 Feb 17]; 5(6):520-39. Disponible en: http://dx.doi.org/10.23857/pc.v5i6.1509 [ Links ]
Received: December 08, 2021; Accepted: January 15, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
