










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkEnfermería Global
versão On-line ISSN 1695-6141
Enferm. glob. vol.22 no.69 Murcia Jan. 2023 Epub 20-Mar-2023
https://dx.doi.org/10.6018/eglobal.513611
Originals
Palliative healthcare needs in the Complex Chronic Degenerative Patient
1Nursing department. National Institute Salvador Zubirán National Medical Center. Mexico City. Mexico
2Research Unit. National School of Nursing and Obstetrics. Mexico City, Mexico. gandhy_ponce@yahoo.com.mx
3Nursing Career Faculty of Higher Studies Zaragoza, National Autonomous University of Mexico. Mexico City, Mexico
Introduction:
Providing necessary healthcare to complex chronic degenerative patients, including palliative care, is a current important demand in order to increase the life expectancy of these populations.
Objective:
To describe the main needs regarding palliative care of persons living with complex chronic degenerative conditions in an institution of 3rd level of attention. The theoretical framework is Wagner's Chronic Care Model.
Methodology:
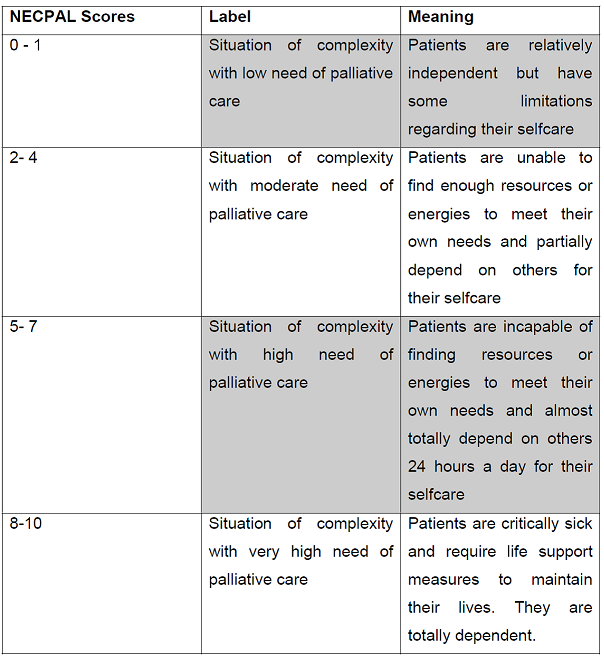
This is a descriptive, transversal, quantitative research. A total of 50 hospitalized patients without oncologic diagnosis from an institution of 3rd level of attention were assessed in order to identify their palliative care needs. The NECPAL CCOMS-ICO© 3.1 (2017) instrument was used. The Kuder-Richardson Reliability Test turned out to be 0.73.
Results:
Most participants showed some degree of cognitive deterioration regarding the areas of attention and language. Based on the Karnofsky index, 60% of the participants were physically disabled to carry out their daily activities. Fragility was evident in 82% of the participants, while 64%, 58%, and 62% showed delirium, pressure sores, and dysphagia respectively.
Discussion and Conclusions:
The present study contributes to the knowledge regarding the special care needs of persons living with complex chronic degenerative conditions. An objective is to reduce the long and costly hospital stays by implementing a home-extended palliative care plan which actively integrates the family members in the care process and decision making.
Keywords: palliative care; complex chronic degenerative illnesses; care needs; nursing
INTRODUCTION
Some changes in the epidemiological transition of the last decade have been characterized by increases in the life expectancy of the populations, and therefore, by increases in chronic degenerative illnesses as well. In order to address this new reality, healthcare professionals are required to adjust their perspective of care and provide the necessary attention to chronic patients, including Palliative Care (PC).
Palliative Care, as a special care approach, is mainly focused on improving the quality of life of chronic patients through addressing the symptoms and secondary effects of the treatments. Palliative Care has a goal of helping patients suffering from a serious illness to live as best as possible and for as lodieng as possible; in other words, to live with quality, or as Cicely Saunders expresses "... to live until the day you die" 1. The WHO estimates that annually 40 million persons - of which 78% live in low or middle income countries - are in need of palliative care 2.
Around 75% of all people will die due to one or several chronic progressive illnesses, meaning that simultaneously, they will require a great deal of attention, will face important ethical and clinical decisions, and will use diverse healthcare and social services 3; therefore, the timely identification of patients requiring palliative care can increase the likelihood of improving their quality of life, while at the same time, respecting their values and beliefs through the best care practices 2,4.
Palliative Care Needs
It is estimated that in 2015, 41 million people worldwide died due to chronic degenerative illnesses. According to the National Institute of Statistics and Geography of Mexico, in 2018, 101,257; 149,368; 93,372; and 35,300 persons died due to complications of diabetes, heart illnesses, tumors, and cerebrovascular illnesses respectively 5. These patients are in need of permanent monitoring because of their special fragility. This is why they are referred to as complex patients. In other words, complex chronic degenerative patients are those who are suffering from one or more chronic illnesses in advanced stages and other chronic related illnesses, disabilities, as well as insufficient social support to address their needs. Some characteristics of these patients are:
A high probability of suffering crises or decompensations.
A need of being monitored and followed up.
The use of urgency or emergency services.
A limited life expectancy forecast.
The use of diverse medical appliances.
A situation of fragility with high risk of functional and cognitive decline.
An adverse social situation.
The World Health Organization defined Palliative Care (PC) as the improvement of the quality of life of patients and their families through prevention and relief of suffering by means of an early identification and appropriate treatment to the physical and spiritual symptoms 6.
In Mexico, access to palliative care is limited because less than 10% of patients requiring this kind of healthcare actually receive it. The four main illnesses groups which require more palliative care for their addressing are: cardiovascular, oncologic, chronic respiratory, and metabolic.
People who die from cancer generally have a predictable short terminal course. In contrast, patients with cardiac, pulmonary, hepatic, or renal insufficiency can experience a slow and fluctuating decline over the years (1 to 5 years). Nevertheless, those patients rarely have palliative care.
Chronic non transmissible illnesses are closely related to the aging process and the adoption of unhealthy lifestyles 7. Behind these conducts are the psychological and social factors, including the socioeconomic status, the education level, the family environment, etcetera, which all need to be thoroughly considered as well. This situation is similar worldwide but it becomes even more critical in countries with lower incomes. Therefore, it is very important that all governments join efforts in fostering healthy environments.
For healthcare providers, it is particularly relevant to timely identify the special needs of patients requiring palliative care; to reassure the control of pain and other symptoms; and to promote the psychological, emotional, and spiritual wellbeing to both the patients and their families. Wagner's Chronic Care Model is one of the first widely shared system which addresses all these special issues. The model has been in use for about 20 years. It is focused on the interactions of well informed and active patients with proactive and well prepared healthcare teams 8. Moreover, this model requires a health system which is well organized and linked to the resources of the community. Simultaneously, the healthcare teams should have the appropriate skills on the usage of assessment instruments, clinical guidelines, and related information technologies.
The synchronization of patients and their families with the functions of nurses is an interacting process aimed at improving the communications, solving doubts, and lowering the number of hospitalizations for situations which can be handled by telephone, video-calling, or home visits.
MATERIALS AND METHODS
This is a quantitative, descriptive, transversal, and correlational study on a population of 50 patients with complex chronic degenerative illnesses, hospitalized in an institution of 3rd level of care in the City of Mexico [N=157]. The unit of analysis was the hospitalized patient (in floors 1,2, or 3), of both sexes, who were in the hospital because of illness (1 to 3 months).
A pilot was carried out with 11 patients having similar characteristics. The NECPAL CCOMS-ICO© 3.1 9 instrument adapted by Ayala, Carmona and Ponce 2019 was used.
The criteria of inclusion were:
Hospitalized patients on units of 1st, 2nd, or 3rd floors of a selected institution of 3rd level of attention with the corresponding authorization and informed consent from the patient or the responsible family member.
Patients with chronic illnesses in situation of advanced or terminal stages (oncologic, and/or chronic pulmonary, cardiac, neurological, hepatic, renal).
Patients with decompensations due to other illnesses including chronic and autoimmune.
The sample was by convenience due to the current sanitary emergency because of COVID-19. The variables of interest considered were:
01: Function decline.
02: Cognitive decline.
03: Nutrition decline.
04: Severe dependency.
05: Geriatric syndrome.
06: Psychosocial aspects.
The Kuder-Richardson Reliability Test turned out to be 0.73 suggesting a good internal consistency. The clinical history, medical appliances checklist, and patients and their families interviews were used. Patients were assessed from the 7th day of their registration during a 2-3 days period. Descriptive statistics; instrument scores weights; and inferential statistics were all calculated.
Data were processed using SPSS version 25. The study was approved by the ethics committee of the hospital. An informed consent was obtained from all the participants regarding their assessments and data gathering. The study followed the guidelines of the General Law of Health article 4th as well as those of the Deontological Code of Nursing.
RESULTS
The average age of the participants was 58 years old. Fifty eight percent were female. The average hospital stay was 44 days. Most participants had their residencies in other states; and 56.6% were married. The average of existing comorbidities in the participants was 3. Chronic pulmonary illnesses accounted for 30% of the total. Cardiac illness accounted for 27% of the total. The average weight loss was 3.38 kilograms (Graph 1).
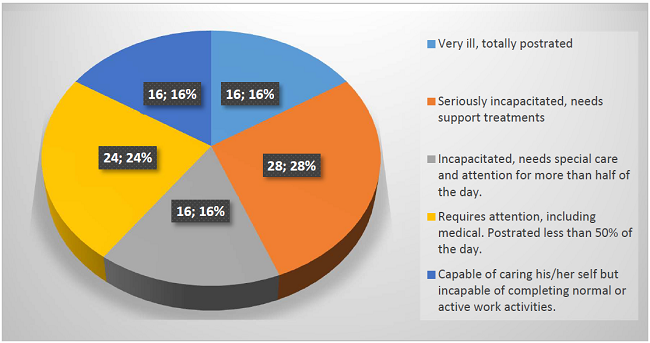
44% of the participants were postrated on bed 24 hours a day with a serious health status; nevertheless, 84% of these hospitalized patients required some degree of nursing medical attention, including total support (Graph 2).
Cognitive decline in terms of orientation, memory, and language was detected in 54% of these patients in a moderate to severe level, making it necessary to have nursing interventions.
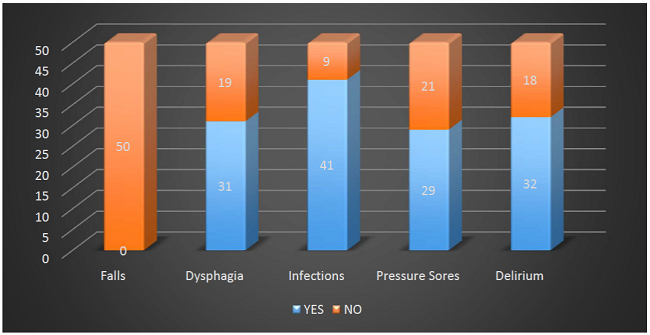
Fragility was found in 82% of these patients regarding infections (41%), delirium (64%), and dysphagia (62%) (Graph 3).
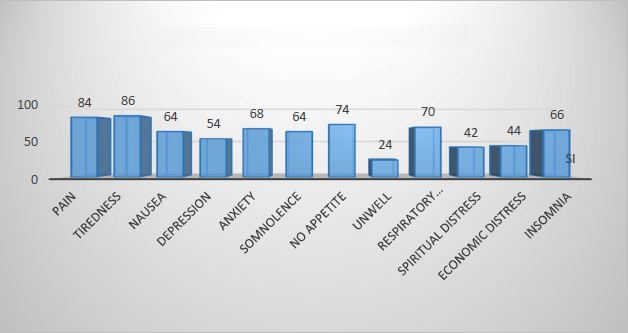
Regarding persistent symptoms, 84% of these patients manifest chronic pain, 74% had no appetite, 70% showed respiratory distress, 64% were in a state of somnolence most of the day (Graph 4).
All patients (100%) showed progressive illnesses with 8 or more persistent symptoms.
The NECPAL dimensions are shown in Graph 5. Nine out of ten participants manifested psychological distress, and 7 out of 10 presented social vulnerability. All these indicators highlight the magnitude of the pain, risk, and vulnerability which these patients undergo.

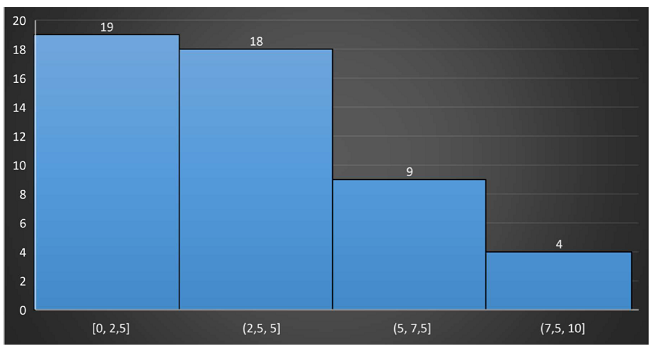
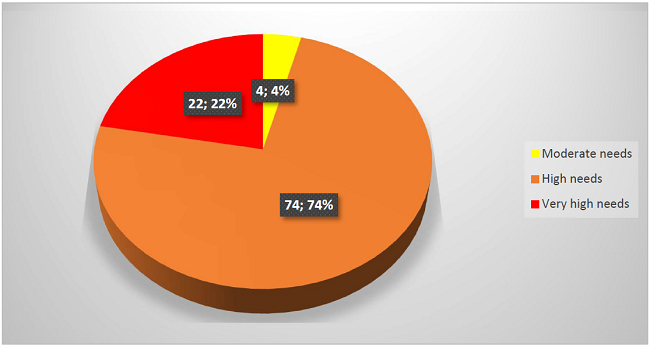
The needs regarding palliative care were from high to very high in 95% of the population (Graph 6).
Inferential statistics were calculated with a confidence interval of 95%. The Spearman's R for non parametric samples (n = 50) yielded the following significant values:
Regarding the dimensions of fragility and age, a weak and positive association was found (R Spearman = .471, p=.001), suggesting that the older the patients are, the more symptoms of fragility they suffer.
Regarding the dimensions nutritional decline and physical distress, a weak and positive association was found, reflecting what happens in 40% of cases of the study, and suggesting that the more nutritional decline the patients have, the more physical distress they suffer (R Spearman = .424, p= .002).
A weak and positive association was found between fragility and nutritional decline which reflects what happens in 33% of the cases in this study, suggesting that the more fragility the patients show, the more nutritional decline they have (R Spearman .336 , p=.017).
A mid size and positive association was found between fragility and the palliative care need (R Spearman .424 y p= .002), suggesting that, the more fragility the patients show, the more palliative care needs they have. This was clear in 42% of the cases of the study.
A mid size and positive association was found between cognitive decline and palliative care (R Spearman .550, p=.000), suggesting that the more cognitive decline the patients have, the more palliative care they need.
An association was also found between palliative care needs and nutritional decline (R Spearman .550, prob= .000), suggesting that the more nutritional decline the patients have, the more palliative care they need.
Regarding differences in sex and palliative care needs, Mann-Whitney U test was calculated. There were no significant differences between women and men ( p≥.05).
DISCUSSION
The nutritional decline of these patients reveals that 7 out of 10 participants have some degree of weight loss. A similar finding was reported in Colombia 10. Moreover, in women between 60 and 74 years old, a weight loss of more than 5% has been associated with a double risk of disability in comparison with those without weight loss11.
Regarding the functional decline measured with the Karnoksky scale 12, and considering the retrospective study by Zamora et al., in Spain 13, it is believed that pain and other oncologic signs are related with the functional decline; nevertheless, in this study such association was not found.
Camargo and Laguado in Colombia 14 refer that 41.7% of the participants in their study showed some cognitive decline in the dimensions of orientation, balance, memory, and language. In this study, 54% of patients demonstrated such association.
Escuin et al15., detected in more than 50% of the participants in their study some nutritional, functional, and cognitive decline, as well as severe dependency in more than 90% of the cases which also presented geriatric syndromes and persistent symptoms. This finding is similar to what was found in the present study.
Regarding the presence of a component of fragility in terms of Wagner's Model 16, in relation to a syndrome of biological reduction and accumulation of stress and multiple physiological problems in older adults with complex chronic problems, a study carried out in Latin America showed that fragility was clearly associated with the number of comorbidities and the degree of cognitive decline 17.
CONCLUSIONS
The present study contributes to acknowledging the needs of palliative care which older adults with complex chronic conditions require. Moreover, the palliative care can reduce the burden of economic and social costs to the families.
The promotion of planning of palliative care avoids unnecessary treatments, a situation which can reduce further body intervention complications. The healthcare teams should share the objectives of palliative care in order to provide comfort to the patient and also reduce the stress on a single healthcare provider.
This study also promotes a reflection on the design of better palliative care protocols based on the early identification of needs and the use of modern and validated instruments in order to address the diverse and complex needs of these populations.
Palliative care should be extended to patients with chronic illnesses who are not necessarily in advanced stages. People requiring palliative care are not only persons with cancer, but also those suffering from complex chronic illnesses of the heart, lungs, kidneys, or because of complications from HIV. Palliative care should always consider the relief of pain and suffering and the security all basic needs.
A fundamental function of healthcare teams is to contribute to the improvement and support of patients in their final stage of life. These healthcare teams should constantly be trained and updated, just as Murray and Sheikh suggest. The Model of Palliative Care of Wagner for chronic patients is a successful reference guide. Therefore, the health system in Mexico should evolve in its health politics and personnel formation regarding the provision of palliative care.
Acknowledgment
We thank the participation of the patients who agreed on being included in this study. We are also thankful to the Institute and its areas Palliative Care for their support in the data collection process
REFERENCES
1. Saunders C. The care of the dying patient and his family. Doc Med Ethics. 1975;(5). doi: 10.1080/13520806.1972.11759235. PMID: 11662275. [ Links ]
2. Organización mundial de la salud. Cuidados Paliativos. Datos y cifras. [on line] publicación del 20 agosto de 2020. Disponible en: https://www.who.int/es/news-room/fact-sheets/detail/palliative-care#:~:text=Se%20estima%20que%20anualmente%2040,necesitan%20asistencia%20paliativa%20la%20reciben. [ Links ]
3. McNamara B, Rosenwax LK, Holman CD. A method for defining and estimating the palliative care population. J Pain Symptom Manage. 2006;32:5-12. [ Links ]
4. Gómez, B. Blay, C; Martinez MM, Lasmarias C, Vila L, Espinosa J, Costa X, et al. The Catalonia WHO Demonstration Project of Palliative Care: Results at 25 Years (1990- 2015). Journal of pain Symptom Management, 2016. Vol. 52 (1): 92. [ Links ]
5. Instituto Nacional de Geografía e Informática. Características de las defunciones registradas en México durante 2018. [on line] Comunicado de Prensa Núm. 538/19. 31 de octubre de 2019. Disponible en: https://www.inegi.org.mx/contenidos/saladeprensa/boletines/2019/EstSociodemo/DefuncionesRegistradas2019.pdf [ Links ]
6. Gobierno de México. InfoCáncer México. Cuidados Paliativos. [on line] Accessed 20 Marzo de 2021. Disponible en: https://www.infocancer.org.mx/?c=emociones-y-cancer&a=cuidados-paliativos#:~:text=La%20definici%C3%B3n%20que%20da%20la,alivio%20del%20sufrimiento%20por%20medio . [ Links ]
7. Organización mundial de la salud. Enfermedades no transmisibles. Datos y cifras. [on line] publicación del 01 de junio de 2018. Disponible en: https://www.who.int/es/news-room/fact-sheets/detail/noncommunicable-diseases [ Links ]
8. Costa KC, Cazola LHO, Tamaki EM. Assessment of Chronic Illness Care (ACIC): avaliação da aplicabilidade e resultados. Saúde debate. 2016; 40:106-117 [ Links ]
9. Gómez-Batiste X, Blay C, Martínez-Muñoz M, Lasmarías C, Vila L, Espinosa J, et al. The Catalonia Palliative Care WHO Demonstation Project: Results at 25 years. J Pain Symptom Management. 2016;52:92-9. [ Links ]
10. Sociedad española de Geriatría y Gerontología. Valoración nutricional en el anciano. Recomendaciones prácticas de los exertos en geriatría y nutrición. [Internet]. 2016. Consultado el 23 de diciembre de 2021 de https://www.segg.es/media/descargas/Acreditacion%20de%20Calidad%20SEGG/Residencias/valoracion_nutricional_anciano.pdf [ Links ]
11. Magda Ginnette Rodríguez, Elba Giomar Sichacá, Mortalidad por desnutrición en el adulto mayor, Colombia, 2014-2016. Rev. Biomédica del Instituto Nacional de Salud. Vol. 39 Núm. 4 (2019). [on line] 2019. DOI: https://doi.org/10.7705/biomedica.4733 Consultado de: https://www.segg.es/media/descargas/Acreditacion%20de%20Calidad%20SEGG/Residencias/valoracion_nutricional_anciano.pdf [ Links ]
12. Crooks V, Waller S, Smith T, Hahn T. The use of the Karnofsky Performance Scale in determining outcomes and risk in geriatric outpatients. J Gerontol Med Sci 1991;46:139-44 [ Links ]
13. Zamora-M A, Nabal VM, Zamora C, García FR, Calderero, AV, Aubi CO, Lostalé LF. Declive funcional y presencia de síntomas en cuidados paliativos: ¿causa o consecuencia?. Revista Española de Geriatría y Gerontología. Vol. 52. Núm. 3. páginas 142-145 (Mayo - Junio 2017 [on line] DOI: https://doi.org/10.1016/j.regg.2016.10.004. [ Links ]
14. Camargo-HKC, Laguado-JE. Grado de deterioro cognitivo de los adultos mayores institucionalizados en dos hogares para ancianos del área metropolitana de Bucaramanga - Santander, Colombia. Univ. Salud [on line]. 2017 19( 2 ): 163-170. https://doi.org/10.22267/rus.171902.79 [ Links ]
15. Escuín R, García. B. Monche, P. Valoración de la necesidad de atención paliativa de pacientes crónicos avanzados en el momento del alta hospitalaria. [on line] Enferm. clín. 2019; 29(1): 18-26, ene.-feb. Accessed 20 Marzo de 2021. Available at: https://pesquisa.bvsalud.org/portal/resource/pt/ibc-181645 [ Links ]
16. Wagner EH, Austin BT, VonKorff M. Organizing carer for patients with chronic illness. Milbank k Q. 1996. 74 (4) 511-44 [ Links ]
17. Partenazi RR, Silva FJ, Farias PM, Oliveira SA, Jose HV, Ferreira SJ. Síndrome de la fragilidad en el adulto mayor y sus factores asociados: comparación de dos ciudades. [on line] Rev. Latino-Am. Enfermagem 2018;26:e3100. https://doi.org/10.1590/1518-8345.2897.3100 [ Links ]
Received: March 03, 2022; Accepted: September 21, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
