










Meu SciELO
 Serviços customizados
Serviços customizadosServiços Personalizados
Journal
Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkEnfermería Global
versão On-line ISSN 1695-6141
Enferm. glob. vol.22 no.69 Murcia Jan. 2023 Epub 20-Mar-2023
https://dx.doi.org/10.6018/eglobal.512081
Originals
Nutritional status and nutritional support strategies in Pediatric Intensive Care Cali-Colombia
1University of Valley. Cali. Colombia. luis.alexander.lovera@correounivalle.edu.co
2Imbanaco Medical Center, School of Nursing- University of Valley. Cali. Colombia
Introduction:
Hospital malnutrition is the result of the conjugation between nutritional alterations generated by the underlying pathology and nutritional risk factors given by hospitalization. It is one of the main complications and the main cause of increased morbidity and mortality in pediatric intensive care units.
Objective:
To describe the nutritional status and nutritional support strategies used in a pediatric intensive care unit.
Materials and Methods:
A descriptive cross-sectional study was carried out, using convenience sampling in 30 children hospitalized in a pediatric intensive care unit. Univariate and bivariate analysis was performed, based on the theoretical model proposed by the nursing theorist Virginia Henderson.
Results:
70% of the children were admitted with pathologies that generate a high risk of malnutrition, 43% were admitted with depleted nutritional status, 97% had nutritional support early, 87% of the children received caloric intake adequate to their needs, 6% of the children presented malnutrition during hospitalization, these results allowed the assessment of the need to eat and drink in children.
Conclusions:
Biological factors such as admission pathologies, previous nutritional status, and age, represented a negative influence on the satisfaction of the need to eat and drink in the children in the study and, therefore, on the risk of hospital malnutrition.
Keywords: hospital malnutrition; nutritional risk; pediatric intensive care; nursing theory
INTRODUCTION
Child malnutrition (ID) represents a public health problem worldwide, according to estimates by the World Bank/WHO/UNICEF in 2015, every year fifty million children in the world suffer from acute malnutrition, of this total, sixteen million have severe acute malnutrition and thirty-four, severe acute malnutrition moderate (1)(2)(3. According to the epidemiological bulletin issued by the National Institute of Health (INS) of Colombia in epidemiological week 17 of 2018, 4,193 cases of acute malnutrition in children were reported nationwide, with a prevalence of 0.09% per 100,000 children under 5 years4.
ID is the result of insufficient food intake that does not cover the protein-energy needs of the child, this being the main cause, which is determined in turn by different biological, social, political, and economic factors 5,6. This problem can generate irreversible harmful effects on the future of the children who suffer from it7.
Malnutrition is no longer a problem that occurs only in the outpatient, because it not only affects children who live in different communities, but also occurs in the group of children who for one or another clinical reason must be hospitalized8. This problem is aggravated in critically ill children who must be admitted to pediatric intensive care units (PICU), where factors such as decreased food intake, increased caloric loss, and increased energy expenditure secondary to the response metabolic stress, substantially increase the chances of developing malnutrition during hospitalization9,10.
Hospital malnutrition (DH) is the result of the conjugation between the nutritional alterations generated by the underlying pathology and the nutritional risk factors given by hospitalization 11. It is one of the main complications and the main cause of increased morbidity and mortality in PICUs. 12 Hospital malnutrition has been the subject of research in the last 25 years, giving rise to multiple studies in which, in general, it is estimated that between 25-50% of patients admitted to hospitals have some degree of malnutrition, increasing its incidence during hospitalization 13,14.
Children are especially vulnerable to malnutrition because all of their systems are immature and developing 15. The establishment of nutritional support must be early and adapted to the biological conditions of age, given that the nutritional support strategies used in PICUs pose a challenge for health personnel, since they constitute the only way to counteract or reduce the negative impact of the underlying pathology and hospitalization conditions on nutritional status 15,16.
It is vitally important to recognize the nutritional status of these patients and evaluate the nutritional support strategies used, since this allows the health team to direct nutritional care that responds to the clinical conditions and real needs of the patient. Different studies have been carried out worldwide, in Latin America and at the national level, where the nutritional status of children hospitalized in the PICU is evaluated 11-13. However, in the department of Valle del Cauca, there is little evidence describing the nutritional status of these patients and the nutritional support strategies used in the PICU.
The present investigation was raised from the need to describe the nutritional status and nutritional support strategies used in children of a PICU in the city of Cali, with the purpose of recognizing the nutritional conditions in which this specific population is. and what are the nutritional support strategies used in the nutritional care of children admitted to the PICU.
MATERIALS AND METHODS
A descriptive cross-sectional study was carried out, using a non-probabilistic sampling for convenience, where the sampling frame was constituted by 30 children admitted to a pediatric intensive care unit in the city of Cali, between the month of November of the year 2017 and June 2018, which met the following inclusion criteria: age between 1 month and 10 years, stay greater than or equal to 7 days and with the criterion of stay in intensive care, the children who were excluded from the study were those whose clinical condition did not allow the anthropometric evaluation of weight and height on day 7 of hospitalization.
The patients were approached in the PICU with prior institutional authorization and from the human ethics review committee of the Universidad del Valle with approval certificate 017-017 and prior signed consent by the parents. The information was obtained from the implementation of a collection instrument with a spreadsheet of Microsoft Excel, which was adjusted and adapted, which was developed for the purposes of the study and adapted to the target population. The aim of the study was to describe the nutritional status and nutritional support strategies used in a pediatric intensive care unit. This instrument was applied on the first and seventh day of hospitalization.
The following variables were evaluated: sociodemographic data, age, admission pathology, weight and height on day 1 and day 7 of hospitalization in the PICU, type of nutritional support received, method of administration of nutritional support, caloric intake and total fluid intake.
The nutritional status was determined by calculating the weight/height index - height/age index on day 1 and for day 7 only the weight/height index was evaluated, since height did not show significant changes in 7 days. and changes in the weight/height index represent acute changes in nutritional status. Subsequently, the children were classified according to the type and degree of malnutrition, by means of the classification of Waterlows 17.
The information obtained was recorded in a data matrix in the Excel 2016 program, the analysis of the information was carried out in light of Virginia Henderson's model of human needs 18,19. Bearing in mind that, in this theory, Henderson states that needs are determined by biological, social, cultural, spiritual and environmental factors, the study variables were organized according to the type of factors to which they belong, as follows: a). social factors: sociodemographic variables, b). biological factors: the patient's age, previous nutritional status, underlying disease, weight loss, and nutritional status on the seventh day. Environmental factors in the PICU: caloric requirements and nutritional support received by patients.
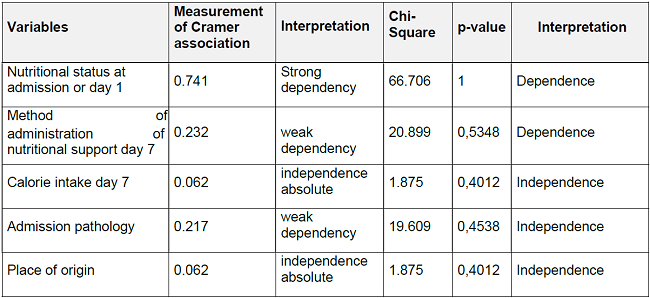
The analysis univariate and bivariate analysis was performed using the statistical software SPSS version 12, generating for the analysis univariate Tables and graphs of frequency distribution, the bivariate analysis consisted of the cross between the dependent variable: nutritional status on day 7 of hospitalization and the other independent variables of the investigation. This bivariate statistical analysis was carried out by means of two statistical significance tests: to determine the existence or not of an association between the dependent variable and the independent variables, the Pearson Chi-Square statistical coefficient was used, and the intensity of the association was determined by Cramer's V coefficient. The null hypothesis of the study was the independence of the variables
RESULTS
It was found in the data obtained that 80% of the children were between 1 month and 24 months old, of which 46% were minor infants and 34% were older infants, 20% were between 3 and 8 years old. Regarding the sex of the patients, 43% were female and 57% male, in relation to place of residence it was found that 24% reside in the rural area and 76% in the urban area, regarding the socioeconomic stratum, 83.4% belong to stratum 1 and 2, 16.7% to strata 3 and 4. Biological factors: Admission pathologies: Related to the pathologies for which children are admitted to the PICU, we found that 26.6%% of the children were admitted for decompensated heart disease, 26.6% with respiratory pathology, 16.6% were due to cardiac surgery, 10 % of children admitted due to infectious pathology and 6.6% of children admitted due to pop laparotomy, 3.3% due to traumatic brain injury, 6.6% admitted due to pathology of neurological origin.
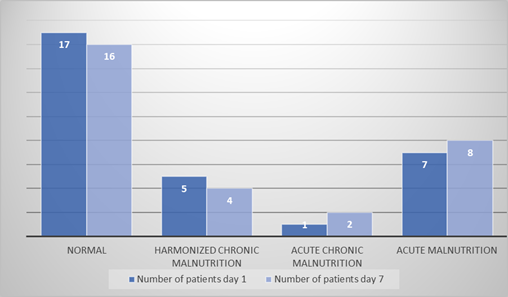
Nutritional status: Figure 1 shows the nutritional status of children on day one (admission) and day seven of hospitalization in a pediatric intensive care unit in the city of Cali. On day 7, the increase of patients with exacerbated chronic malnutrition and acute malnutrition with respect to the day of admission; The reduction of patients with normal nutritional status and Harmonized Chronic Malnutrition with respect to the nutritional status on the day of admission is also appreciated.
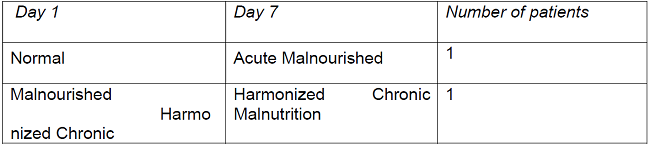
In a detailed analysis of the patients, it is possible to observe the change of two patients on day 7 with respect to the day of admission, thus, it is observed that a patient on day 1 with normal nutritional status on day seven of hospitalization was with acute malnutrition and one patient with harmonized chronic malnutrition became acutely ill on the seventh day of hospitalization, as shown in Table 1.
The pathology of the children who presented malnutrition during hospitalization was in one of the postoperative cases of cardiac surgery and the other case was admitted due to decompensated heart disease.
Changes in children's weight: 53% of children after seven days of hospitalization lost weight, 33% remained the same weight and 13% increased weight. A total of 16 patients lost weight, of which 8 lost between 1 and 5%, 5 between 5 and 10% and three of them between 10 and 20%.
PICU environment factors
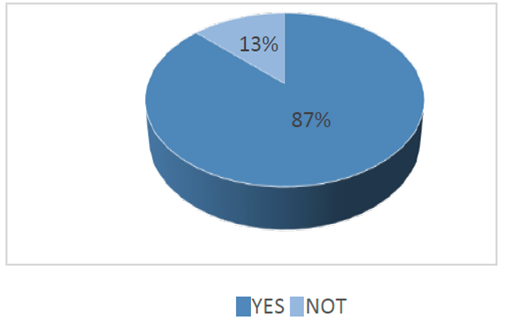
Type of nutritional support: 33% of children received Complete Oral Nutrition, 23% Total Parenteral Nutrition, 17% of children mixed nutritional support, and 13% Enteral Nutritional support, 7% received intravenous maintenance fluids and enteral nutrition, 3% received maintenance lev without any additional nutritional support, in this 3% of the patients the answer to the question of the questionnaire was correlated, where the reason why they do not receive any type of nutritional support is investigated, finding that they do not there was no contraindication to receive it. Nutritional support administration method: it was found that the most frequent methods are the Oral method in 36%, followed by Parenteral with 23%, 13% received enterally, 10% received orally and parenterally. Caloric requirement: Figure 2 shows that 13% of the children do not receive a caloric requirement corresponding to the needs, while 87% do receive the caloric requirement corresponding to the patient's needs.
Below is a conceptual map that presents the findings and the analysis carried out in light of Virginia Henderson's theory of human needs (Figure 3).
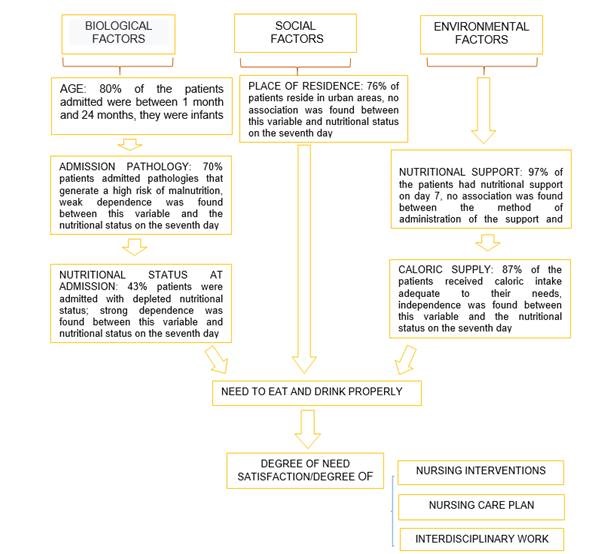
DISCUSSION
Hospital malnutrition in the framework of the model of human needs proposed by the nursing theorist Virginia Henderson18,19 can be considered as the dissatisfaction of the child's need to eat and drink properly, where different constant or pathological factors can affect the satisfaction of this need, it is important to evaluate the interaction of the different biological, social and environmental factors, to To be able to understand their behavior and possible influence on the satisfaction or not of the nutritional need and therefore on the development or not of in-hospital malnutrition of hospitalized children, these factors interact and influence the nutritional status of children, according to their Specific conditions; for example, the age of less than 2 years in children when entering the unit, is a factor that increases the risk of malnutrition, this is due to the fact that infants have a lower liver glycogen reserve and capacity gluconeogenic decreased compared to older children. This condition in the context of admission to an intensive care unit, where there is an increase in caloric expenditure and there may be a decrease in protein and caloric intake (insufficient nutritional support), can exhaust the adaptation mechanisms and generate a hypercatabolic state which can end in rapid nutritional depletion, which is evidenced by severe weight loss during hospitalization in intensive care, being a severe weight loss if it is greater than or equal to 2% during the first week 20. However, this aspect must be analyzed within the framework of the specific conditions of the hospitalized child, since other conditions can generate this severe weight loss in this population.
Henderson, (18,19 describes that there are pathological factors associated with the dissatisfaction of the nutritional need. She lists the basic pathologies. Different studies have shown that admission pathologies such as cardiac, respiratory, and neurological pathologies can represent a risk factor for acquiring hospital malnutrition by generating special nutritional needs, increased caloric expenditure and alterations in the adequate intake of nutrients 21)(22)(23)(24).
Adequate nutritional support to the needs of patients is a fundamental environmental factor to prevent child hospital malnutrition. There is an international consensus about the advantages of early nutritional support; The American Society for Enteral and Parenteral Nutritional Support (ASPEN) recommends early initiation of nutritional support (within 24-48 hours of admission to the PICU) as this can prevent weight loss in the first week after the beginning of the hospitalization of the child in the unit, they also recommend the administration of nutrition by enteral and oral route preferably, since it represents physiological, nutritional and immunological benefits, in terms of caloric intake ASPEN recommends a caloric intake of up to two thirds of the nutrient goal in the first week of critical illness to avoid hospital malnutrition 25.
Knowledge and evaluation of the interaction of biological, social and environmental factors is necessary to generate nursing interventions within the framework of interdisciplinary work with the care team, seeking to reduce the prevalence of hospital malnutrition and therefore reduce the impact on morbidity and mortality and improve the welfare conditions of boys and girls hospitalized is essential. In the same sense, the continuous education that is imparted to nurses and male nurses, not only undergraduate and postgraduate, in nutritional matters26. Likewise, in pediatric intensive care, nutrition is one of the fundamental axes of care for boys and girls in critical condition.
Study limitations
One of the limitations during the investigation was an administrative change in the institution where the study was conducted, which substantially reduced the admission of patients to the PICU, and therefore had a negative impact on obtaining patients for the sample of the study. research.
CONCLUSIONS
Satisfaction of the need to eat and drink properly can be negatively affected in the study patients by admission pathologies, the nutritional status at admission and positively impacted by an adequate caloric intake for the needs of the patients and a nutritional intake in mostly oral and enteral.
The nutritional status at admission and the admission pathologies in the PICU children evaluated represent conditions that can favor the development of in-hospital malnutrition.
Age less than 2 years is a basic factor that can influence rapid weight loss and the possible development of hospital malnutrition in our study.
The caloric intake adequate to the needs and the total enteral nutritional support on the seventh day of hospitalization were not sufficient measures to avoid hospital malnutrition in two research participants.
Virginia Henderson's theory was appropriate and allowed an assessment of the status and nutritional support provided to patients, thus answering the research question. East The human needs model allowed an approach to the nutritional status of PICU patients, laying the foundations for the analysis and subsequent implementation of direct nursing interventions, not only from the care perspective, but also in the generation of proposals and programs that allow improve the satisfaction of this need in the PICU. Similarly, it is highlighted about the continuing education in nurses, not only undergraduate and postgraduate, since nutritional issues in intensive pediatric care, They are one of the fundamental axes of care for children in critical condition.
REFERENCIAS
1. Ministerio de Salud y Protección Social, Fondo de las Naciones Unidas para la Infancia - UNICEF. Lineamiento para el manejo integrado de la desnutrición aguda moderada y severa en niños y niñas de 0 a 59 meses de edad [Internet]. Ministerio de Salud y Protección Social - UNICEF; 2017. Disponible en: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/PP/lineamiento- desnutricion-aguda-minsalud-unicef-final.pdf [ Links ]
2. Bouma S. Diagnosing Pediatric Malnutrition. Nutr Clin Pract. 2017;32(1):52-67. [ Links ]
3. Dipasquale V, Cucinotta U, Romano C. Acute Malnutrition in Children: Pathophysiology, Clinical Effects and Treatment. Nutrients. 2020;12(8):1-9. [ Links ]
4. Wisbaum W. La desnutrición infantil: causas, consecuencias y estrategias para su prevención y tratamiento. UNICEF España; 2011. [ Links ]
5. Vargas M, Hernández E. Los determinantes sociales de la desnutrición infantil en Colombia vistos desde la medicina familiar. Medwave. 2020;20(2):1-8. [ Links ]
6. Wells J. The capacity-load model of non-communicable disease risk: understanding the effects of child malnutrition, ethnicity and the social determinants of health. Eur J Clin Nutr. 2018;72(5):688-97. [ Links ]
7. Vikram K, Vanneman R. Maternal education and the multidimensionality of child health outcomes in India. J Biosoc Sci. 2020;52(1):57-77. [ Links ]
8. Nangalu R, Pooni P, Bhargav S, Bains H. Impact of malnutrition on pediatric risk of mortality score and outcome in Pediatric Intensive Care Unit. Indian J Crit Care Med. 2016;20(7):385-90. [ Links ]
9. Kang M, Kim H, Ryu S, Moon J, Park H. Korean Society for Parenteral and Enteral Nutrition (KSPEN) Clinical Research Groups. Prevalence of Malnutrition in Hospitalized Patients: a Multicenter Cross-sectional Study. J Korean Med Sci. 2018;8(33):1-10. [ Links ]
10. Gigato M, Hernández G, Martínez D, Aguilar M. Impacto de un programa de capacitación en nutrición sobre la atención de enfermería en el cuidado del paciente crítico. Rev Cubana Aliment Nutr. 2014;24(1):1-14. [ Links ]
11. Correia MITD, Perman MI, Waitzberg DL. Hospital malnutrition in Latin America: A systematic review. Clinical Nutrition. 1 de agosto de 2017;36(4):958-67. [ Links ]
12. Garcia M, Meireles M, Führ L, Donini A, Wazlawik E. Relationship between hand grip strength and nutritional assessment methods used of hospitalized patients. Rev Nutr. 2013;26:49-57. [ Links ]
13. Waitzberg D, Ravacci G, Raslan M. Desnutrición hospitalaria. Nutr Hosp. 2011;26(2):254-64. [ Links ]
14. Botina D, Ayala V, Paz I, Limas L, Mafla A. Estado nutricional y riesgo de malnutrición en pacientes hospitalizados del Hospital Universitario Departamental de Nariño. Revista de la Universidad Industrial de Santander. 2013;45(3):1-13. [ Links ]
15. Silva N, Ribeiro-Silva R, Rasella D, Alves F, Campello T, Fiaccone R, et al. Shifts towards overweight and double burden of malnutrition among socio-economically vulnerable children: a longitudinal ecological analysis of Brazilian municipalities. Public Health Nutr. 2021;24(15):4908-17. [ Links ]
16. Joosten K, Eveleens R, Verbruggen S. Nutritional support in the recovery phase of critically ill children. Curr Opin Clin Nutr Metab Care. 2019;22(2):152-8. [ Links ]
17. Ferreira H. Anthropometric assessment of children's nutritional status: a new approach based on an adaptation of Waterlow's classification. BMC Pediatr. 2020;20(65):1940-6. [ Links ]
18. Henderson V. Principios Básicos de los cuidados de enfermería. Primera. Washington: OMS; 1961. 59 p. [ Links ]
19. Ahtisham Y, Jacoline S. Integrating Nursing Theory and Process into Practice; Virginia's Henderson Need Theory. International Journal of Caring Sciences. 2015;8(2):443-50. [ Links ]
20. Mehta N, Skillman H, Irving S, Coss-Bu J, Vermilyea S, Farrington E, et al. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: Society of Critical Care Medicine and American Society for Parenteral and Enteral Nutrition. JPEN J Parenter Enteral Nutr. 2017;41(15):706-42. [ Links ]
21. Fernández M, López M, Álvarez P, Arias J, Varela J. Farmacia Hospitalaria. Síndrome de realimentación. 2009;33(4):183-93. [ Links ]
22. Burgos R. Desnutrición y enfermedad. Nutr Hosp Suplementos. 2013;6(1):10-23. [ Links ]
23. Reber E, Gomes F, Vasiloglou M, Schuetz P, Stanga Z. Nutritional Risk Screening and Assessment. J Clin Med. 2019;8(1065):1-9. [ Links ]
24. Kaegi-Braun N, Mueller M, Schuetz P, Mueller B, Kutz A. Evaluation of Nutritional Support and In-Hospital Mortality in Patients With Malnutrition. JAMA Netw Open. 2021;4(1):1-13. [ Links ]
25. Valencia E, Marin A. Guias de Soporte Metabolico y Nutricional, ASPEN 2016. Con actualización de Graficas y traducción completa [Internet]. 2016. Disponible en: https://www.researchgate.net/publication/305488154_Guias_de_Soporte_Metabolico_y_ Nutricional_ASPEN_2016_Con_actualizacion_de_Graficas_y_traduccion_completa [ Links ]
26. Martínez A. Ecos de la primera Jornada Nacional de Enfermería en Nutrición en el marco de la Jornada Nacional de la Sociedad Cubana de Nutrición Clínica y Metabolismo. Revista Cubana de Enfermería. 2012;28(1):2-3. [ Links ]
Received: February 22, 2022; Accepted: April 23, 2022
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
