










 Serviços customizados
Serviços customizados
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkResearch shows that serious emotional and behavioral problems occur during childhood and adolescence (Ezpeleta et al., 2014; Polanczyk et al., 2015; Solmi et al., 2022). Development from infancy to adolescence involves the acquisition of numerous emotional, cognitive, and social skills in interaction with the multiple contexts in which children grow up (e.g., family, school, society). These interactions are the basis for children and adolescents reaching maturity and autonomy (Kostelnik et al., 2009; Maddux & Winstead, 2016). Throughout this process, the analysis and identification of dysfunctional behaviors and emotional symptoms play an essential role in the early detection of possible mental health problems (Solmi et al., 2022).
The study of mental health in the child-adolescent populations has evolved over the last three decades (Dozois, 2019). The existence of child psychopathology was recognized in the 19th century, and understanding of it improved substantially with the inclusion of childhood disorders in the categorical classifications for clinical diagnosis in the mid to late 1980s (Dozois, 2019; González, 2000). This included categorical classification systems such as the Diagnostic and Statistical Manual of Mental Disorders in its successive versions, up to the current one (American Psychiatric Association, 2013), which remains the predominant standard classification manual internationally for the identification of psychopathological disorders. Recently, in the search for further classificatory alternatives, two broad-spectrum dimensions that characterize child psychopathology were found based on empirical research: internalizing and externalizing problems (Achenbach, 1991; Achenbach et al., 2017). Internalizing disorders are characterized by disordered moods or behaviors such as withdrawal, anxiety, depression, or somatic complaints, whereas externalizing disorders are characterized by disordered behaviors such as rule-breaking and aggressive behavior syndromes. These broadband dimensions have been included even in dimensional taxonomies like the Hierarchical Taxonomy of Psychopathology [HiTOP], which proposes the idea that shared maladaptive symptoms and traits are grouped by nomological criteria into subfactors and spectra (Conway et al., 2019; DeYoung et al., 2022; Forbes et al., 2021; Kotov et al., 2021; Krueger et al., 2018; Ruggero et al., 2019).
Methodologically, to measure the relationships between psychological constructs and observable variables (items and particular manifest behavior), two traditional approaches have been applied: the reflective model congruent with Factor Analysis, where the psychological construct is seen as the common cause of the observed behaviors (e.g., depression is the cause of sadness, crying, etc.), and the formative model, where the observed behaviors define or determine the construct (e.g., diet, exercise, and self-care together define health). These two approaches involve conducting the statistical analysis on the structure of the psychopathological construct (as an aggregate score) but not on the dynamics of manifest symptoms (Borsboom et al., 2011; Fried et al., 2017; Guyon et al., 2017). In response to this important limitation, the network analysis paradigm emerges (Borsboom et al., 2011; Epskamp, 2017; Fonseca-Pedrero, 2017, 2018) as a way of exploring behaviors and symptoms that can lead to a more dynamic, dimensional, and transdiagnostic approach to psychopathology. The network perspective treats psychological constructs as dynamic systems whose components may be autonomous causal agents that influence each other beyond an underlying cause. From this perspective, the concept of latent variable is obviated in the measurement of variables, and instead specific behaviors (not constructs) theoretically and empirically recognized as dysfunctional are proposed (Epskamp, 2017; van Bork, 2019).
Analysis of the network as a dynamic system of relationships identifies the “core” components (i.e., those with the strongest connections) that are responsible for symptom activation and impact on the structure or connectivity of the system or network itself (Borsboom & Cramer, 2013; Fried, 2017; Guyon et al., 2017; Jones, 2017; Jones et al., 2021). On the network model, the notion of mental health would correspond to a stable state of a weakly connected network of symptoms, while psychological disorders would correspond to stable states of strongly connected symptom networks (Borsboom, 2017).
Although the last decade has brought a growing body of research studying psychopathology from the network perspective, there are still very few studies with child and adolescent populations focusing on the dynamics of the symptoms, especially on externalizing problems. McElroy et al. (2018) used network analysis to study the relationships between anxiety and depression symptoms in children from 5 to 14 years old in a sample of 1,147 children. They found that states of being “anxious,” “sad,” “nervous,” and “worthless” were core symptoms in maintaining the network of mixed anxiety and depression over the years studied. Subsequently, in a clinical sample of 37,162 participants with an average age of 13 years, this same research group identified the symptoms that had the greatest impact (expected influence) on the relationships between some internalizing symptoms such as “sudden feelings of anxiety for no apparent reason,” “fear of being ridiculous in public,” “worry,” and “feelings of worthlessness.” Eating problems and compulsive behaviors showed the least expected influence (McElroy & Patalay, 2019).
In a longitudinal analysis, Funkhouser et al. (2021) found three communities of symptoms or domains: Inattention, externalizing problems, and internalizing problems. In these three domains, the most central symptoms, which best predicted the rest, were depressive mood, inattention, and worry. With a sample of 551 Norwegian children (age 3-12) with moderate to high levels of conduct problems, Hukkelberg (2019) found the majority of behaviors clustered into two distinct domains, reflecting inattention and oppositional defiant behavior. Thus, “Does not obey house rules in his/her own (house),” which showed the highest betweenness centrality, appears to be a central behavior in connecting the various behaviors. In addition, the items “has a short attention span” and “verbally fights with friends his/her own age” showed high centrality strengths.
The general aim of this study is to identify the most relevant symptoms responsible for the activation of other associated symptoms. More specifically, the aim is to explore the dynamics of symptoms using a network analysis of the various syndromes of emotional and behavioral problems in children established by Achenbach and Rescorla (2001): Internalizing problems (depression, anxiety, withdrawal, and somatic complaints), externalizing problems (rule-breaking and aggressive behavior), and other problems of a mixed and contextual nature (attention problems, thought problems, and social problems). This allows us to know the dynamics of symptoms of psychological problems and the delimitation of potential mechanisms that give rise to a particular psychological disorder. It would be one of the few studies to explore the relationships among internalizing and externalizing symptoms in children and adolescents using network analysis.
In accordance with the previous studies, we expect symptoms related to negative affect (i.e., anxiety, sadness, fear) to be the most relevant symptoms responsible for activating internalizing symptoms (McElroy et al., 2018), whereas inattention and oppositional defiant behaviors are expected to be the most relevant symptoms for externalizing problems (Hukkelberg, 2019; Funkhouser et al., 2021). Since, to the best of our knowledge, no differential studies focused on each type of disorder have been conducted, no specific hypotheses can be formulated for each particular disorder.
Method
Participants
The sample consisted of 986 Spanish children and adolescents, including 540 girls (55%) and 446 boys (45%). Their ages ranged from 9 to 18 years (M = 13.09, SD = 2.01). Participants were selected from various public and charter schools in several Spanish cities (Logroño, Vitoria, Burgos, Cádiz, Algeciras, Jaen, Madrid, and Segovia). The participants were enrolled at three educational levels (primary school, secondary school, and bachelor's degree). The primary-school students were in grades 4 (9-10 years old) through 6 (11-12 years old), while for those in secondary school and above, all grades and levels were represented from the first-year course in secondary school (ages 12-13) to the fourth (ages 15-16) and from the first year of bachelor's studies (ages 16-17) to the second (ages 17-18). In general terms, the family structures were as follows: children, father, and mother living together (84.9%); children living with mother (6.2%); children living with father (1.1%); and children in shared custody (5.5%). As shown in Table 1, the distribution of participants according to age and sex variables was homogeneous (χ2 = 2.56, gl = 3, p = 0.47).
The inclusion criteria called for participants between the ages of 9 and 18, belonging to both sexes, who were present in the classroom on the days the instruments were administered and who had their parents' authorization to participate in the study (in the case of minors). The exclusion criteria were not having parental authorization to participate in the study and not being present at the evaluation sessions.
Table 1. Distribution of participants by sex and age groups.
| Sex | 9-10 years old | 11-12 years old | 13-14 years old | 15-18 years old | Total |
|---|---|---|---|---|---|
| Boys | 47 (4.77%) | 119 (12.07%) | 167 (16.93%) | 113 (11.46%) | 446 (45.23%) |
| Girls | 60 (6.09%) | 157 (15.92%) | 176 (17.84%) | 147 (14.91%) | 540 (54.77%) |
| Total | 107 (10.85%) | 276 (27.99%) | 343 (34.79%) | 260 (26.36%) | 986 |
Note.The percentages in brackets apply to the total sample.
Instruments
Clinical symptoms of depression were measured using the Center for Epidemiological Studies Depression Scale for Children and Adolescents, CES-DC (Radloff, 1977, 1991; Weissman et al., 1980), Spanish version, by Sánchez-Hernández et al. (2018). This scale groups behaviors into Depressed Affect, Somatic Symptoms, Interpersonal Problems, and Positive Affect. It consists of 20 items with four Likert-type response options (1 = almost nothing to 4 = a lot). The reliability of the scale using the Omega coefficient for this sample was ꞷ = .92. The dimensions measured were Depressed Affect (7 items, ꞷ = .91), Somatic Symptoms (7 items, ꞷ = .73), Interpersonal Problems (2 items, ꞷ = .72), and Positive Affect (4 items, ꞷ = .75) (using its natural score of constructs with positive connotation). Using the CES-DC as opposed to using only the Youth Self-Report (YSR) allowed the evaluation of a specific range of depressive symptoms, which was not sufficiently represented in the latter.
The YSR (Achenbach, 1991; Achenbach & Rescorla, 2001; Spanish version by Unitat d'Epidemiologia i de Diagnòstic en Psicopatologia del Desenvolupament, 2001) is a self-report that evaluates emotional and behavioral problems in children and adolescents. It has 112 items measured on a Likert-type scale with three answer options (0 = not true to 3 = true, very often, or fairly often). The higher the score on the subscales, the higher the degree of psychopathology. The test groups the constructs into: (a) Internalizing Problems (Anxiety-Depression, Withdrawn-Depression, and Somatic Complaints); (b) Externalizing Problems (Aggressive Behavior and Rule-Breaking Behavior); and (c) Problems of a Mixed Personal-Contextual Nature (Thought Problems, Attention Problems, and Social Problems). For the present study, certain symptoms referring to depression were excluded (items 14, 52, 91, and 33 of Anxiety-Depression; items 5, 102, and 103 of Withdrawn-Depression) because they were already contained in the CES-DC. Therefore, the respective reliabilities of the subscales for Internalizing Problems, applying the Omega coefficient for the present sample, were: Anxiety (8 items, ꞷ = .66), Withdrawn (5 items, ꞷ = .70), and Somatic Complaints (10 items, ꞷ = .71). Under Externalizing Problems, the reliabilities were: Aggressive Behavior (17 items, ꞷ = .84) and Rule-Breaking Behavior (15 items, ꞷ = 79). Under Problems of a Mixed Personal-Contextual Nature, the reliabilities were: Thought Problems (12 items, ꞷ = .75), Attention Problems (9 items, ꞷ = .78), and Social Problems (11 items, ꞷ = .71) .
Procedure
The Ethics Commission of the National University of Distance Education (UNED) authorized the study and affirmed its compliance with the ethical and data protection standards required by European legislation. Authorization was then requested from the schools and informed consent sought from the participants' parents and the participants themselves. To guarantee the participants' anonymity, all questionnaires were identified using a code that allowed anonymization. Participation was voluntary, and it was ensured that the instructions and evaluation conditions were similar for all participants.
The children answered the questionnaires collectively at the school building under researcher supervision. Since the administration was tightly controlled, practically all the children answered the questionnaires. Two 45-minute periods were used, adjacent to recess, during which students completed the sociodemographic questionnaire and assessment protocol. The guess response of each participant was neither evaluated nor controlled.
Data Analysis
The R software package Version 4.0.3 (R Core Team, 2020) was used to conduct all analyses. First, an exploratory descriptive analysis of the items was performed. In total, the highest percentages of missing data were 2% for the CES-DC items and 3% for the YSR items. It is standard to consider percentages under 20% to be candidates for imputation (Hair et al., 2014). Multiple imputation is recommended as the best method for Likert-type scales (Brown, 2015; Enders, 2010), even for CES-DC (Bono et al., 2007); and among the available multiple imputation techniques, considering the various patterns of missing data, the most appropriate one, is the random forest approach (Kokla et al., 2019; Shah et al., 2014; Tang & Ishwaran, 2017). Hence, in the present study, missing data were imputed with multiple imputation via the random forest technique using the MICE package Version 3.10.0 (van Buuren & Groothuis-Oudshoorn, 2011).
To explore the relationships between symptoms, regularized partial correlation networks were estimated, which graphically represent a model in which statistically significant relationships between symptoms are displayed. To identify the most salient symptoms, standard centrality measures were evaluated: strength [St] (sum of absolute partial correlation coefficients between a node and all other nodes), betweenness [Bet] (how many of the shortest paths between two nodes go through the node in question), closeness [Clo] (how strongly a node is indirectly connected to other nodes in the network), and expected influence [EI] (which takes into account negative associations among nodes) (Costantini et al., 2015; Epskamp, 2017). Both analyses were estimated using the qgraph, centralityTable, and centralityPlot functions in the qgraph package, Version 1.6.5 (Epskamp et al., 2012). The global strength impacts (GSI) (how a node affects the overall connectivity of the network) and network structure impacts (NSI) (how a node could cause changes in the network structure) of the nodes were studied. They were estimated using the impact function with the networktools package, Version 1.2.3 (Jones, 2020). Both indexes refer to the concept of impact and are related to the degree to which the nodes impact or could be affecting the network structure (Jones, 2017).
Results
Internalizing Problems
Figure 1 shows the centrality measures, impact coefficients, and regularized networks of each of the Internalizing Problems. The depressive symptoms that best activate others, facilitate rapid activation, and mediate the activation between symptoms in the network, as shown in Panel A, are: “Feels lonely” (CES14) (St = 2.05, EI = 1.63, Bet = 1.65, Clo = 1.38) and “Thinks life has been a failure” (CES9) (St = 1.30, EI = 1.12, Bet = 3.38, Clo = 2.23). A third symptom that stands out in the dynamics of depression is “Feels sad” (CES18), since it has a high influence on activating the network (St = 1.88, EI = 1.52) and has the greatest impact (GSI = 2.00) on connectivity. However, its activation speed (Clo = 0.38) and role as an intermediary (Bet = 0.46) are moderate.
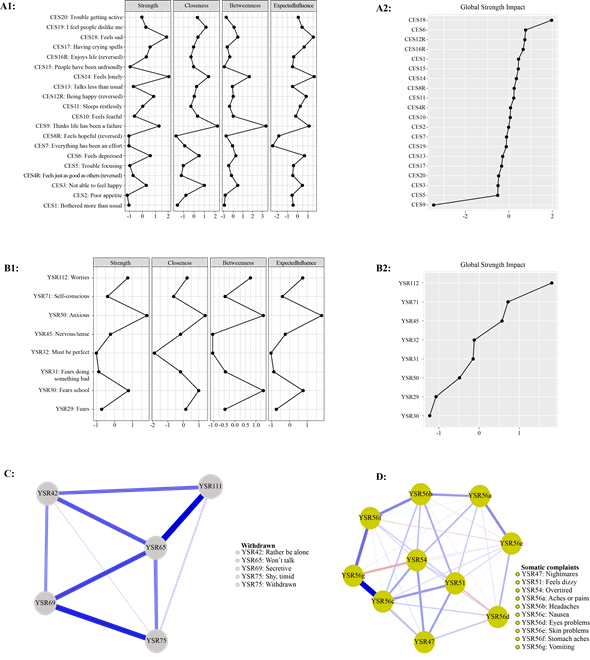
The symptoms that activate anxiety, as shown in Panel B, are characterized by being prominent intermediaries and connecting nodes in the network (high proximity), although the number and weight of their connections tend to be moderate : “Anxious” (YSR50) (St = 1.80, EI = 1.80, Bet = 1.35, Clo = 1.41), “Fears school” (YSR30) (St = 0.76, EI = 0.76, Bet = 1.35, Clo = 1.00), and “Worries” (YSR112) (St = 0.74, EI = 0.74, Bet = 0.75, Clo = 0.26). The latter has the greatest impact on the connectivity of symptoms (GSI > 1.00).
Withdrawn Behaviors are shown in the visualized partial correlation network in Panel C. This network is characterized by being scattered; the behaviors most notable for their connections are “Won't talk” (YSR65) (St = 1.72, EI = 1.72, Bet = 1.57, Clo = 1.52), and “Secretive” (YSR69) (Bet = 0.45, Clo = 0.44), which stands out as an intermediary and activator, having connections that are few, but strong (St = 0.03, EI = 0.03).
Somatic Complaints are shown in Panel D. This network is dense, and the most relevant behaviors due to the number of their connections and their being the best mediators are “Nausea” (YSR56c) (St = 1.79, EI = 1.71, Bet = 1.19) and “Vomiting "(YSR56g) (St = 1.18, Bet = 1.93).
Externalizing Problems
In Figure 2, centrality measures and impact coefficients of Externalizing Problems are presented. In Panel A, Aggressive Behaviors can be seen to be densely connected; but the most prominent for having the strongest connections, revealing itself as the best intermediary and quickly activating the network, is “Threatens others” (YSR97) (St = 1.56, EI = 1.15, Bet = 1.36, Clo = 1.26). Other relevant behaviors are: “Attacks people” (YSR57) (St = 0.77, EI = 1.09), which is relevant for its strength, and “Loud” (YSR104) (Bet = 1.69), “Teases a lot” (YSR94) (Bet = 1.36), and “Argues a lot” (YSR3) (Bet = 1.69, Clo = 1.26), which are relevant for their high mediation. The last of these is the only one with high proximity, which is why it tends to quickly activate the behaviors that are connected to it. The behaviors with the greatest impact on network connectivity (GSI > 1.00) are: “Argues a lot” (YSR3) and “Suspicious” (YSR89).
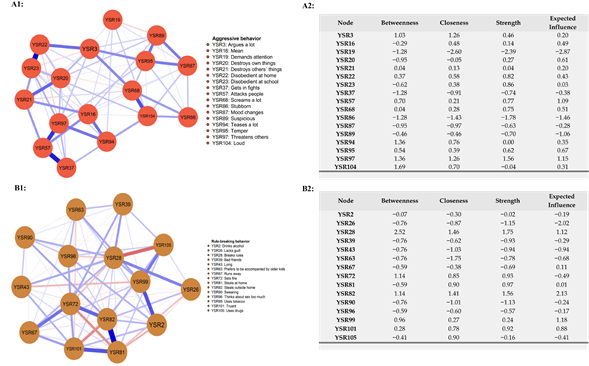
In relation to Rule-Breaking Behavior in Panel B, the behaviors most outstanding for having the strongest connections, showing the best intermediaries, and quickly activating the network are: “Breaks rules” (YSR28) (St = 1.75, EI = 1.12, Bet = 2.52, Clo = 1.46) and “Steals outside home” (YSR82) (St = 1.56, EI = 2.13, Bet = 1.14, Clo = 1.41). Regarding the impact of behaviors on the strength of connections (GSI > 1.00), the most relevant are: “Swearing” (YSR90), “Lying” (YSR43), “Lacks guilt” (YSR26), and “Prefers to be accompanied by older kids” (YSR63).
Personal and Contextual Problems
The findings on Attention Problems, Thought Problems, and Social Problems are presented in Figure 3. As can be seen in Panel A, the symptoms that have strong connections, act as intermediaries, and more rapidly activate this syndrome are: “Confused” (YSR13) (St = 1.13, EI = 1.13, Bet = 2.02, Clo = 1.16), “Inattentive” (YSR78) (St = 1.15, EI = 1.15, Bet = 1.36, Clo = 1.41), and “Can't concentrate” (YSR8) (St = 1.29, EI = 1.29, Bet = 0.04, Clo = 1.09). At the same time, “Impulsive” (YSR41) has a greater impact on connectivity (GSI > 1.00), and “Can't sit still” (YSR10) and “Inattentive” (YSR78) have a greater impact on the network structure (NSI > 1.00).
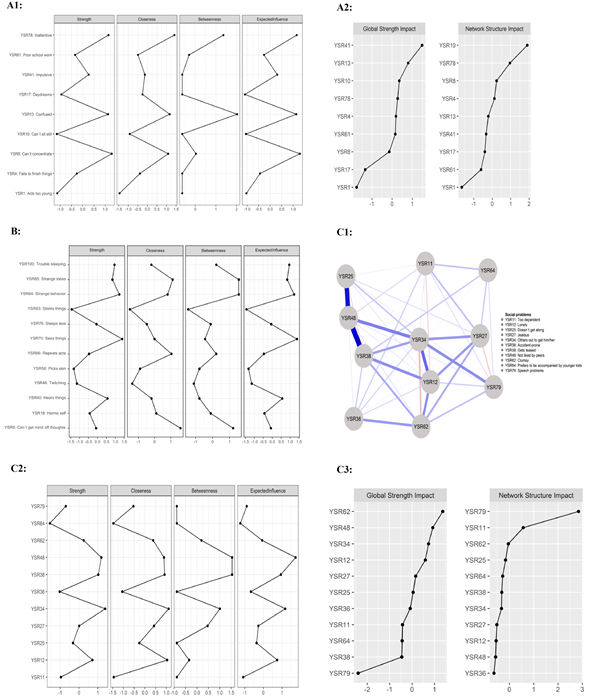
While the most prominent symptoms distinguished in Panel B are the ones with a high activation, such as: “Sees things” (YSR70) (St = 1.39, EI = 1.39) and “Strange behavior” (YSR84) (St = 1.23, EI = 1.23, Bet = 1.54, Clo = 0.81), the latter is also a good intermediary. Others that are good intermediaries and activate the network quickly are: “Can't get mind off thoughts” (YSR9) (Bet = 1.21, Clo = 1.61), “Strange ideas” (YSR85) (Bet = 1.54, Clo = 1.12), and “Repeats acts” (YSR66) (Clo = 1.05).
In Panel C, the symptoms that stand out for their connections and their role as intermediaries and quick activators are: “Others out to get him/her” (YSR34) (St = 1.39, EI = 1.18, Bet = 1.00, Clo = 1.11), “Not liked by peers” (YSR48) (St = 1.19, EI = 1.73, Bet = 1.54, Clo = 0.89), and “Gets teased” (YSR38) (St = 1.03, Bet = 1.54, Clo = 0.92). Standing out as only a fast activator is “Lonely” (YSR12) (Clo= 1.04). Those with the greatest impact (GSI and NSI > 1.00) are: “Clumsy” (YSR62) and “Speech problems” (YSR79).
Discussion
In this study, the central symptoms that facilitate the activation of others within syndromes were identified-specifically, symptoms with the role of intermediaries, symptoms that allow rapid activation of the syndrome, and symptoms with the greatest impact on the connectivity or structure of each psychological network. The particular benefit of this for the study of psychological phenomena is that the network analysis could improve understanding of two aspects of the syndromes: which variables are relevant and which relationships sustain structures that might be working in a dysfunctional way for the subject. Once the fundamental variables or nodes are detected, together with how these nodes are related to others, a psychologist can use this information to promote changes in the subject's psychological network, attenuating the nodes and relations that are malfunctioning. From an exploratory perspective, this network analysis report could help change the understanding of psychological phenomena because it offers alternative ways to operationalize how the variables are measured and how are they related (Fonseca-Pedrero, 2017).
Taking an overview of the results, it can be noted that the most relevant symptoms have an intra- and interpersonal nature. This is consistent with psychopathological theories on both the maintenance and the etiology of mental disorders and their modification through effective psychological interventions that are based on or refer to the role of irrational thoughts or cognitive biases and contextual interactions or influences (Maddux & Winstead, 2016; Riso et al., 2007).
As we expected, in relation to Internalizing Problems, it was shown that symptoms with the highest levels of centrality are those related to Negative Affect (depressive mood, worry, and anhedonia). This especially stands out for depressive symptoms (the three relevant ones are: “Feels lonely” (CES14), “Perceive life has been a failure” (CES9), and “Feels sad” (CES18)) and for anxiety (“Anxious” (YSR50), “Fears school” (YSR30), and “Worries” (YSR112)-even more so because a central role for these symptoms is supported by the evidence of many other empirical studies (Eccles et al., 2020; Figueras, 2006; Martínez-Hernáez & Muñoz García, 2010a, 2010b; McElroy et al., 2018; Nolen-Hoeksema & Hilt, 2009). These results are also consistent with the tripartite model, suggesting a common component of high negative affectivity or general distress for internalizing problems (Clark & Watson, 1991; De Bolle et al., 2011).
The feeling of loneliness refers to dissatisfaction arising from the discrepancy between the personal desire for social relationships and those that actually exist, with a feeling of physical or emotional disconnection from others (Eccles et al., 2020). This feeling of loneliness can be understood to have a relevant and broad effect on the lives of children and adolescents, particularly because of the essential role that relationships with parents and peers play in providing security and support figures in children's growth (Franco Nerín et al., 2014; Kostelnik et al., 2009).
Likewise, sadness is a basic emotional reaction that, when it becomes dysfunctional, manifests itself transversally in several disorders. It should be noted that this symptom is considered an essential criterion (in addition to irritability) for the clinical diagnosis of mood disorders in both the child and adolescent populations as well as in adults (American Psychiatric Association, 2013) and is highly related to feelings of loneliness (Eccles et al., 2020).
The perception of life as a failure can be understood as an automatic, negative cognitive bias that is difficult to control and affects the interpretation and perception of personal experiences (Riso et al., 2007). Hence the recommendation to address such biases with cognitive therapy and consequently to refer children and adolescents to mental health services (Hatherill, 2007).
As for the dynamic of anxiety, excessive worry (with great impact and strong interconnectivity) together with fear played a basic role in the appearance of anxiety syndrome. This emphasizes the interpersonal nature of the symptom “fear of school” (YSR30), which may be based on difficult relationships with peers in the school context, and its possible connection to social problems and withdrawal behaviors, related to selective mutism or ineffective communication with others. These results are consistent with the findings of McElroy and Patalay (2019) that the fears of going to school, going to bed at night, and what others think are the most central. Taken together, all this suggests the importance of fears in childhood, especially those linked to socialization contexts. Along these lines, being socially accepted and having friends is associated with good adjustment, personal well-being, increased school performance, high self-esteem, and a positive feeling of belonging to the group (Piqueras et al., 2019). Thus, high prevalence rates of school problems such as bullying or peer rejection situations in the classroom have been shown to be a risk factor for the development of psychosocial adjustment problems in childhood (Lara-Ros et al., 2017; Piqueras et al., 2019).
Concerning Somatic Complaints, the central symptoms found were related to gastrointestinal symptoms (“Nausea” (YSR56c) and “Vomiting” (YSR56g)). Many studies have consistently shown that somatic symptoms are common manifestations of various psychological problems, such as generalized depression and anxiety, personal maladjustment, and even personality disorders (Bekhuis et al., 2016; de la Barrera et al., 2019; Ordóñez et al., 2015). Although on a symptomatic level, fatigue and lack of rest were the internalizing complaints that stood out the most among adolescents, these are not identified as relevant. This is not consistent with the study by McElroy and Patalay (2019), who found that feelings of fatigue were higher in expected influence in the oldest age groups (15-18 years) as compared to the youngest group (8-11 years), indicating the way symptom expression can change across development and the relevance of studying the dynamics of the items by age groups.
As far as Externalizing Problems are concerned, the most prominent symptomatology in Aggressive Behavior (e.g., “Threatens others” (YSR97), “Argues a lot” (YSR3), “Attacks people” (YSR57), “Teases a lot” (YSR94)) reflects particularities related to students' own developmental characteristics, such as the search for their own identity and autonomy, conflict with parents regarding communication problems, and behaviors showing opposition to authority (Kostelnik et al., 2009; Papalia et al., 2007). Meanwhile, the symptoms with the greatest impact on Rule-Breaking, such as “Breaks rules” (YSR28) and “Steals outside home” (YSR82), are consistent with the central symptoms of adolescent psychopathology found by Hukkelberg (2019). Hence, prevention or general intervention programs that include components such as assertive communication, trust in significant figures, the assumption of responsibilities, and the adequate development of autonomy should be key recommendations and priorities for the promotion of mental health in the child-adolescent populations.
Regarding the problems of a personal and contextual nature, specific symptoms also emerged. Thus, with respect to thought problems, difficulties in cognitive management were revealed in some symptoms such as “Confused” (YSR13), “Can't concentrate” (YSR8), and “Sees things” (YSR70) (which may refer at this age to maladaptive daydreaming). All these symptoms seem related to beliefs about what others think and the cognitive-emotional perception of the effects that the behaviors of others could have on the children and adolescents themselves (Maddux & Winstead, 2016; Piqueras et al., 2019).
In contrast, the symptoms of the more prominent Social Problems (i.e., “Not liked by peers” (YSR48), “Others out to get him/her” (YSR34), and “Gets teased” (YSR38)) highlight those who have a character trait of interpersonal sensitivity, suspicion, or self-referentiality. This suggests guidelines for the design of interventions in both the school and the family context whereby the identification, reflection, and management of referential attributions, as well as positive thoughts and beliefs about others (attributions of intention, alternative thoughts, etc.), could serve as protective resources or coping strategies to deal with this symptomatology (Graham & Reynolds, 2013; Sukhodolsky et al., 2004).
In summary, the symptoms identified in this study reveal specific indicators that can be detected in daily interactions with a child or adolescent through their verbal communication or their attitudes in the various socialization contexts, indicators that go beyond the global manifestation of a disruptive or aggressive nature typical of a general diagnostic category (Solmi et al., 2022). Considering the possible practical implications, it is worth highlighting that the various central symptoms identified in this study can be used as signs, clues, or alarm signals pointing to several mental health problems and can serve as targets for preventive and intervention programs, especially taking into account current proposals for evidence-based psychological treatment in children and adolescents (Fonseca-Pedrero et al., 2021).
This study could contribute to the accumulation of empirical evidence regarding psychological problems during childhood and adolescence. However, the validity of these conclusions has yet to be tested to determine whether these results are robust and replicable. In general terms, for this issue, the scientific method suggests three methodological criteria to be examined: a) model quality (has the technique discovered the “true” model?); b) precision (how many errors are present in the estimated parameters?); and c) replicability: once any theoretical conclusion is proposed based on the results of the network analysis, the question is whether the same phenomenon can be reproduced in other samples (Borsboom et al., 2018; Epskamp, Borsboom et al., 2018). In keeping with the recommendations of Borsboom et al. (2018), it is our view that much more empirical evidence needs to be collected to confirm the conclusion that the results obtained are robust and replicable. Nevertheless, the first step has been taken in this direction.
Future studies applying network analysis should overcome some of the limitations of this study. For instance, the structural dynamics, hierarchy, and roles that apply to the constructs require exploration; at the symptom level, the activation trajectories of specific phenomena call for further study. To improve the assessment of comorbidity, it would be possible to better detect symptoms that act as a bridge in the concurrent presence of disorders in addition to detecting those symptoms whose change or modification in intensity or frequency generate an impact on the global symptomatological picture presented (Bringmann et al., 2013; Jones et al., 2021; Letina et al., 2019). There is also a need to investigate differences by sex and age groups (Epskamp, van Borkulo, et al., 2018; Howe et al., 2020; van Borkulo et al., 2022). Further limitations can also be highlighted, such as the non-random sampling for the selection of participants, the absence of control scales (e.g., measures of infrequency, lying, defensiveness, faking good, and faking bad), and the use of self-reports, which consider only the child's perspective. Future studies will have to overcome all these limitations.

